PLAN NP-3 Concordia Plus - United Concordia
PLAN NP-3 Concordia Plus - United Concordia
PLAN NP-3 Concordia Plus - United Concordia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
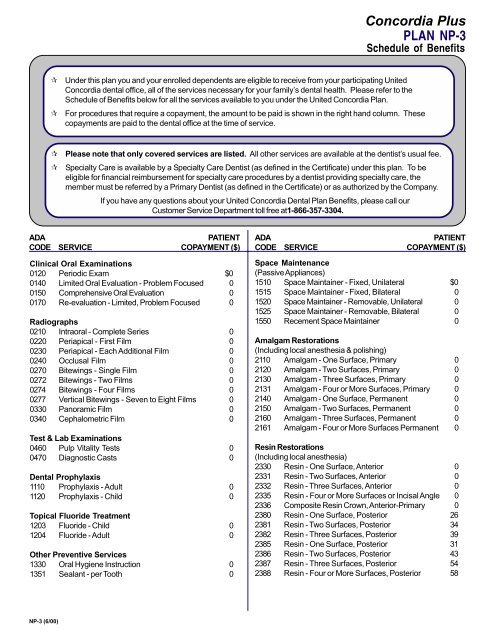
<strong>Concordia</strong> <strong>Plus</strong><br />
<strong>PLAN</strong> <strong>NP</strong>-3<br />
Schedule of Benefits<br />
⌦<br />
⌦<br />
Under this plan you and your enrolled dependents are eligible to receive from your participating <strong>United</strong><br />
<strong>Concordia</strong> dental office, all of the services necessary for your family’s dental health. Please refer to the<br />
Schedule of Benefits below for all the services available to you under the <strong>United</strong> <strong>Concordia</strong> Plan.<br />
For procedures that require a copayment, the amount to be paid is shown in the right hand column. These<br />
copayments are paid to the dental office at the time of service.<br />
⌦<br />
⌦<br />
Please note that only covered services are listed. All other services are available at the dentist’s usual fee.<br />
Specialty Care is available by a Specialty Care Dentist (as defined in the Certificate) under this plan. To be<br />
eligible for financial reimbursement for specialty care procedures by a dentist providing specialty care, the<br />
member must be referred by a Primary Dentist (as defined in the Certificate) or as authorized by the Company.<br />
If you have any questions about your <strong>United</strong> <strong>Concordia</strong> Dental Plan Benefits, please call our<br />
Customer Service Department toll free at1-866-357-3304.<br />
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
Clinical Oral Examinations<br />
0120 Periodic Exam $0<br />
0140 Limited Oral Evaluation - Problem Focused 0<br />
0150 Comprehensive Oral Evaluation 0<br />
0170 Re-evaluation - Limited, Problem Focused 0<br />
Radiographs<br />
0210 Intraoral - Complete Series 0<br />
0220 Periapical - First Film 0<br />
0230 Periapical - Each Additional Film 0<br />
0240 Occlusal Film 0<br />
0270 Bitewings - Single Film 0<br />
0272 Bitewings - Two Films 0<br />
0274 Bitewings - Four Films 0<br />
0277 Vertical Bitewings - Seven to Eight Films 0<br />
0330 Panoramic Film 0<br />
0340 Cephalometric Film 0<br />
Test & Lab Examinations<br />
0460 Pulp Vitality Tests 0<br />
0470 Diagnostic Casts 0<br />
Dental Prophylaxis<br />
1110 Prophylaxis - Adult 0<br />
1120 Prophylaxis - Child 0<br />
Topical Fluoride Treatment<br />
1203 Fluoride - Child 0<br />
1204 Fluoride - Adult 0<br />
Other Preventive Services<br />
1330 Oral Hygiene Instruction 0<br />
1351 Sealant - per Tooth 0<br />
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
Space Maintenance<br />
(Passive Appliances)<br />
1510 Space Maintainer - Fixed, Unilateral $0<br />
1515 Space Maintainer - Fixed, Bilateral 0<br />
1520 Space Maintainer - Removable, Unilateral 0<br />
1525 Space Maintainer - Removable, Bilateral 0<br />
1550 Recement Space Maintainer 0<br />
Amalgam Restorations<br />
(Including local anesthesia & polishing)<br />
2110 Amalgam - One Surface, Primary 0<br />
2120 Amalgam - Two Surfaces, Primary 0<br />
2130 Amalgam - Three Surfaces, Primary 0<br />
2131 Amalgam - Four or More Surfaces, Primary 0<br />
2140 Amalgam - One Surface, Permanent 0<br />
2150 Amalgam - Two Surfaces, Permanent 0<br />
2160 Amalgam - Three Surfaces, Permanent 0<br />
2161 Amalgam - Four or More Surfaces Permanent 0<br />
Resin Restorations<br />
(Including local anesthesia)<br />
2330 Resin - One Surface, Anterior 0<br />
2331 Resin - Two Surfaces, Anterior 0<br />
2332 Resin - Three Surfaces, Anterior 0<br />
2335 Resin - Four or More Surfaces or Incisal Angle 0<br />
2336 Composite Resin Crown, Anterior-Primary 0<br />
2380 Resin - One Surface, Posterior 26<br />
2381 Resin - Two Surfaces, Posterior 34<br />
2382 Resin - Three Surfaces, Posterior 39<br />
2385 Resin - One Surface, Posterior 31<br />
2386 Resin - Two Surfaces, Posterior 43<br />
2387 Resin - Three Surfaces, Posterior 54<br />
2388 Resin - Four or More Surfaces, Posterior 58<br />
<strong>NP</strong>-3 (6/00)
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
Inlay Restorations<br />
2510 Inlay - Metallic, One Surface 100<br />
2520 Inlay - Metallic, Two Surface 161<br />
2530 Inlay - Metallic, Three Surface 171<br />
2542 Onlay - Metallic, Two Surface 190<br />
2543 Onlay - Metallic, Three Surface 190<br />
2544 Onlay - Metallic, Four or More Surfaces 196<br />
Crowns - Single Restoration<br />
2710 Crown - Resin (Laboratory) 87<br />
2740 Crown - Porcelain/Ceramic Substrate 220<br />
2750 Crown - Porcelain, High Noble Metal 215<br />
2751 Crown - Porcelain, Predominantly Base Metal 207<br />
2752 Crown - Porcelain, Noble Metal 211<br />
2780 Crown - 3/4 Cast, High Noble Metal 212<br />
2781 Crown - 3/4 Cast, Predominantly Base Metal 194<br />
2782 Crown - 3/4 Cast, Noble Metal 202<br />
2783 Crown - 3/4 Cast, Porcelain/Ceramic 220<br />
2790 Crown - Full Cast, High Noble Metal 212<br />
2791 Crown - Full Cast, Predominantly Base Metal 194<br />
2792 Crown - Full Cast, Noble Metal 202<br />
2799 Provisional Crown 0<br />
Other Restorative Services<br />
2910 Recement Inlay 0<br />
2920 Recement Crown 0<br />
2930 Prefab Stainless Steel Crown - Primary 0<br />
2931 Prefab Stainless Steel Crown - Permanent 0<br />
2940 Sedative Filling 0<br />
2950 Core Buildup including any Pins 0<br />
2951 Pin Retention 0<br />
2952 Cast Post and Core 0<br />
2953 Each Additional Cast Post - Same Tooth 0<br />
2954 Prefab Post and Core 0<br />
2957 Each Additional Prefabricated Post - Same Tooth 0<br />
2970 Temporary Crown (Fractured Tooth) 0<br />
Pulp Capping<br />
3110 Pulp Cap - Direct 0<br />
3120 Pulp Cap - Indirect 0<br />
Pulpotomy<br />
3220 Pulpotomy 0<br />
3221 Gross Pulpal Debridgement 0<br />
3230 Pulpal therapy - Anterior, Primary Tooth 0<br />
3240 Pulpal therapy - Posterior, Primary Tooth 0<br />
Root Canal Therapy<br />
(Including Treatment plan, clinical procedures follow-up care)<br />
3310 Root Canal Treatment - Anterior 0<br />
3320 Root Canal Treatment - Bicuspid 0<br />
3330 Root Canal Treatment - Molar 193<br />
Re-Treatment<br />
(Including Root Canal Therapy)<br />
3346 Root Canal ReTreatment - Anterior 0<br />
3347 Root Canal ReTreatment - Bicuspid 0<br />
3348 Root Canal ReTreatment - Molar 212<br />
<strong>NP</strong>-3 (6/00)<br />
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
3410 Apicoectomy - Anterior 132<br />
3421 Apicoectomy - Bicuspid 143<br />
3425 Apicoectomy - Molar 156<br />
3426 Apicoectomy - Each Additional Root 60<br />
3430 Retrograde - per Root 10<br />
3450 Root Amputation - per Root 85<br />
3920 Hemisection - per Root 74<br />
Other Endodontic Procedures<br />
3950 Canal Prep & Fitting of Preformed Dowel or Post 0<br />
4210 Gingivectomy - Quadrant 92<br />
4211 Gingivectomy - Per Tooth 30<br />
4220 Gingival Curettage - Quadrant 41<br />
4240 Gingival Flap - Quadrant 88<br />
4245 Apically Positioned Flap 150<br />
4249 Crown Lengthening 111<br />
4260 Osseous Surgery - Quadrant 197<br />
4263 Bone Replacement Graft - first site in quad 98<br />
4264 Bone Replacement Graft - each additional<br />
site in quad 99<br />
4274 Distal or Proximal Wedge 46<br />
Adjunctive Periodontal Services<br />
4341 Scaling and Root Planing - Quadrant 0<br />
4355 Full Mouth Debridement 0<br />
Other Periodontal Services<br />
4910 Periodontal Maintenance 0<br />
Complete Dentures<br />
(Including routine post-delivery care)<br />
5110 Complete Upper Denture 266<br />
5120 Complete Lower Denture 266<br />
5130 Immediate Upper Denture 282<br />
5140 Immediate Lower Denture 282<br />
Partial Dentures<br />
(Including routine post-delivery care)<br />
5211 Upper Partial - Resin Base 213<br />
5212 Lower Partial - Resin Base 220<br />
5213 Upper Partial - Cast Metal Base 282<br />
5214 Lower Partial - Cast Metal Base 282<br />
5281 Removable Unilateral Partial Denture - One<br />
Piece Cast Metal 158<br />
Adjustments to Removable Prosthesis<br />
5410 Adjust Complete Denture, Upper 14<br />
5411 Adjust Complete Denture, Lower 14<br />
5421 Adjust Partial - Upper 14<br />
5422 Adjust Partial - Lower 14<br />
Repairs to Complete & Partial Dentures<br />
5510 Repair Broken Complete Denture Base 27<br />
5520 Replace Missing/Broken Teeth - Complete<br />
Denture 28<br />
5610 Repair Resin Saddle or Base 26<br />
5620 Repair Cast Framework 29<br />
5630 Repair or Replace Broken Clasp 32<br />
5640 Replace Broken Tooth 24
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
5650 Add Tooth to existing Partial Denture 30<br />
5660 Add Clasp to existing Partial Denture 36<br />
Denture Rebase Procedures<br />
5710 Rebase-Complete Upper Denture 81<br />
5711 Rebase-Complete Lower Denture 81<br />
5720 Rebase-Upper Partial Denture 95<br />
5721 Rebase-Lower Partial Denture 95<br />
Denture Reline Procedures<br />
5730 Reline-Complete Upper Denture (Chairside) 52<br />
5731 Reline-Complete Lower Denture (Chairside) 52<br />
5740 Reline-Upper Partial Denture (Chairside) 48<br />
5741 Reline-Lower Partial Denture (Chairside) 48<br />
5750 Reline-Complete Upper Denture (Lab) 77<br />
5751 Reline-Complete Lower Denture (Lab) 77<br />
5760 Reline-Upper Partial Denture (Lab) 81<br />
5761 Reline-Lower Partial Denture (Lab) 81<br />
Other Removable Prosthetic Services<br />
5850 Tissue Conditioning-Upper Denture 0<br />
5851 Tissue Conditioning-Lower Denture 0<br />
Bridge Pontics<br />
6210 Pontic-Cast, High Noble Metal 212<br />
6211 Pontic-Cast, Predominantly Base Metal 194<br />
6212 Pontic-Cast, Noble Metal 202<br />
6240 Pontic-Porcelain, High Noble Metal 215<br />
6241 Pontic-Porcelain, Predominantly Base Metal 207<br />
6242 Pontic-Porcelain, Noble Metal 211<br />
6245 Pontic - Porcelain, Ceramic 220<br />
Bridge Retainers<br />
6740 Crown - Porcelain, Ceramic 220<br />
6750 Crown-Porcelain, High Noble Metal 215<br />
6751 Crown-Porcelain, Predominantly Base Metal 207<br />
6752 Crown-Porcelain, Noble Metal 211<br />
6780 Crown - 3/4 Cast, High Noble Metal 210<br />
6781 Crown - 3/4 Cast, High Noble Metal 194<br />
6782 Crown - 3/4 Cast, Noble Metal 202<br />
6783 Crown - 3/4 Cast, Porcelain/Ceramic 220<br />
6790 Crown-Full Cast, High Noble Metal 212<br />
6791 Crown-Full Cast, Predominantly Base Metal 194<br />
6792 Crown-Full Cast, Noble Metal 202<br />
Other Fixed Prosthetic Services<br />
6930 Recement Bridge 0<br />
6970 Cast Post and Core 64<br />
6971 Cast post as part of fixed partial retainer 55<br />
6972 Prefab Post and Core 55<br />
6973 Core Buildup including any Pins 46<br />
6976 Each Additional Cast Post - Same Tooth 0<br />
6977 Each Additional Prefabricated Post - Same Tooth 0<br />
Simple Extractions<br />
7110 Extraction - Single 0<br />
7120 Extraction - Additional Tooth 0<br />
7130 Root Removal 0<br />
<strong>NP</strong>-3 (6/00)<br />
ADA<br />
PATIENT<br />
CODE SERVICE COPAYMENT ($)<br />
Surgical Extractions<br />
(Including local anesthesia and routine post-operative care)<br />
7210 Surgical Extraction-Erupted Tooth 45<br />
7220 Soft Tissue Impaction 56<br />
7230 Partial Bony Impaction 75<br />
7240 Complete Bony Impaction 89<br />
7241 Removal of Impacted Tooth - Completely<br />
Bony with Unusual Surgical 90<br />
7250 Surgical Removal Residual Roots 45<br />
7280 Surgical Exposure, for Orthodontics 108<br />
7281 Surgical Exposure, Aid Eruption 75<br />
7310 Alveoloplasty in Conj with Extraction-Quadrant 46<br />
7320 Alveoloplasty without Extraction-Quadrant 59<br />
7450 Removal of odontogenic cyst - up to 1.25 cm 75<br />
7960 Frenulectomy 68<br />
Limited Orthodontic Treatment<br />
8010 Limited Orthodontic Treatment of the primary<br />
Dentition 750<br />
8020 Limited Orthodontic Treatment of the<br />
transitional Dentition 750<br />
8030 Limited Orthodontic Treatment of the<br />
adolescent Dentition 750<br />
8040 Limited Orthodontic Treatment of the<br />
adult Dentition 750<br />
Interceptive Orthodontic Treatment<br />
8050 Interceptive Orthodontic Treatment<br />
of the primary Dentition 900<br />
8060 Interceptive Orthodontic Treatment<br />
of the transitional Dentition 900<br />
Comprehensive Orthodontic Treatment<br />
8070 Comprehensive Orthodontic Treatment<br />
of the Transitional Dentition 1900<br />
8080 Comprehensive Orthodontic Treatment<br />
of the Adolescent Dentition 2100<br />
8090 Comprehensive Orthodontic Treatment<br />
of the Adult Dentition 2300<br />
Minor Treatment to Control Harmful Habits<br />
8210 Removable Appliance Therapy 212<br />
8220 Fixed Appliance Therapy 222<br />
Other Orthodontic Services<br />
8680 Orthodontic retention 400<br />
8999 Orthodontic Records Fee 350<br />
General Services<br />
9110 Palliative Treatment 0<br />
9220 General Anesthesia - First 30 Minutes 200<br />
9221 General Anesthesia - Each Additional 15 Minutes 40<br />
9241 Intravenous Sedation/Analgesia - First 30 Minutes 200<br />
9242 Intravenous Sedation/Analgesia - Each<br />
Additional 15 Minutes 40<br />
9310 Consultation, Other than Treating Dentist 30<br />
9400 Broken Appointment charge per 15 minutes<br />
(w/o 24 hours notice) 10<br />
9440 Office Visit, After Hours 43