full-time student dependent certification - United Concordia
full-time student dependent certification - United Concordia
full-time student dependent certification - United Concordia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
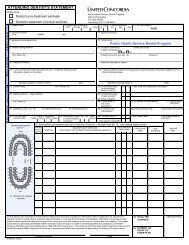
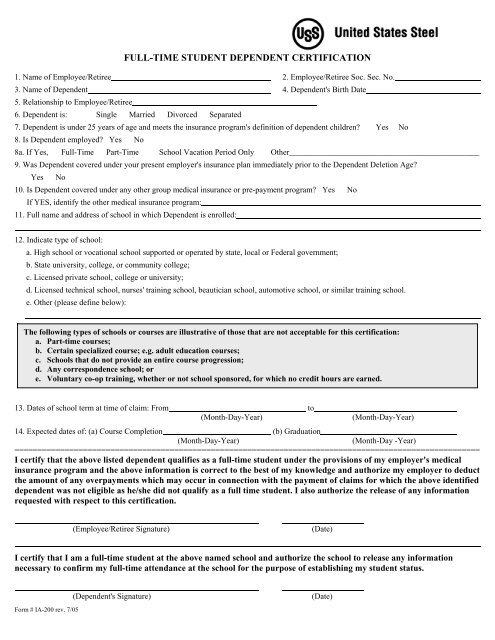
FULL-TIME STUDENT DEPENDENT CERTIFICATION<br />
1. Name of Employee/Retiree 2. Employee/Retiree Soc. Sec. No.<br />
3. Name of Dependent 4. Dependent's Birth Date<br />
5. Relationship to Employee/Retiree<br />
6. Dependent is: Single Married Divorced Separated<br />
7. Dependent is under 25 years of age and meets the insurance program's definition of <strong>dependent</strong> children? Yes No<br />
8. Is Dependent employed? Yes No<br />
8a. If Yes, Full-Time Part-Time School Vacation Period Only Other_______________________________________________<br />
9. Was Dependent covered under your present employer's insurance plan immediately prior to the Dependent Deletion Age?<br />
Yes No<br />
10. Is Dependent covered under any other group medical insurance or pre-payment program? Yes No<br />
If YES, identify the other medical insurance program:<br />
11. Full name and address of school in which Dependent is enrolled:<br />
12. Indicate type of school:<br />
a. High school or vocational school supported or operated by state, local or Federal government;<br />
b. State university, college, or community college;<br />
c. Licensed private school, college or university;<br />
d. Licensed technical school, nurses' training school, beautician school, automotive school, or similar training school.<br />
e. Other (please define below):<br />
The following types of schools or courses are illustrative of those that are not acceptable for this <strong>certification</strong>:<br />
a. Part-<strong>time</strong> courses;<br />
b. Certain specialized course; e.g. adult education courses;<br />
c. Schools that do not provide an entire course progression;<br />
d. Any correspondence school; or<br />
e. Voluntary co-op training, whether or not school sponsored, for which no credit hours are earned.<br />
13. Dates of school term at <strong>time</strong> of claim: From to<br />
(Month-Day-Year)<br />
(Month-Day-Year)<br />
14. Expected dates of: (a) Course Completion (b) Graduation<br />
(Month-Day-Year)<br />
(Month-Day -Year)<br />
======================================================================================================<br />
I certify that the above listed <strong>dependent</strong> qualifies as a <strong>full</strong>-<strong>time</strong> <strong>student</strong> under the provisions of my employer's medical<br />
insurance program and the above information is correct to the best of my knowledge and authorize my employer to deduct<br />
the amount of any overpayments which may occur in connection with the payment of claims for which the above identified<br />
<strong>dependent</strong> was not eligible as he/she did not qualify as a <strong>full</strong> <strong>time</strong> <strong>student</strong>. I also authorize the release of any information<br />
requested with respect to this <strong>certification</strong>.<br />
(Employee/Retiree Signature)<br />
(Date)<br />
I certify that I am a <strong>full</strong>-<strong>time</strong> <strong>student</strong> at the above named school and authorize the school to release any information<br />
necessary to confirm my <strong>full</strong>-<strong>time</strong> attendance at the school for the purpose of establishing my <strong>student</strong> status.<br />
Form # IA-200 rev. 7/05<br />
(Dependent's Signature)<br />
(Date)
INSTRUCTIONS FOR USS STUDENT CERTIFICATION FORM<br />
Please complete all necessary information on the Full-Time Student Dependent Certification form including signing and dating the form in the<br />
spaces provided. Please note that the form requires the signatures of both the employee/retiree and the <strong>student</strong>.<br />
Company Blue Cross/Blue Shield Medical Program:<br />
• A <strong>student</strong>’s eligibility for coverage is usually determined at the <strong>time</strong> a claim for benefits is received by Highmark Blue Cross/Blue Shield.<br />
When a claim is filed for a potential <strong>student</strong> <strong>dependent</strong> and a current Full-Time Student Dependent Certification form is not on file, a Full-<br />
Time Student Dependent Certification form is mailed to your home. The claim is held for 30 days pending the receipt of the completed<br />
form.<br />
• Your child’s “<strong>full</strong>-<strong>time</strong> <strong>student</strong>” status will be certified from January through September and/or from September through January.<br />
However, you will not receive another mailing when the <strong>certification</strong> period has expired.<br />
• You will need to:<br />
- Proactively request, complete and return a completed Full-Time Student Dependent Certification form prior to each of the two periods<br />
described above, or<br />
- Re-certify your child once it’s apparent that their claims are being denied for lack of coverage (Highmark will hold the claim and send<br />
you a blank Full-Time Student Dependent Certification form. If the form is not returned within thirty (30) days, you will be notified<br />
that the claim has been denied. The claim will be reprocessed for payment only upon receipt of the properly completed Full-Time<br />
Student Dependent Certification form.), or<br />
- Pre-certify your <strong>student</strong> <strong>dependent</strong> before any claim is filed by sending Highmark a completed form each January and September.<br />
• When a <strong>dependent</strong> of yours is no longer a <strong>full</strong>-<strong>time</strong> <strong>student</strong>, you must call Highmark at 1-800-245-6642.<br />
For a medical claim return Full-Time Student Dependent Certification form to:<br />
Highmark BCBS<br />
USS Dedicated Unit<br />
120 Fifth Avenue<br />
Suite P3503<br />
Pittsburgh, PA 15222<br />
Prescription Drug Program:<br />
• Certification of your <strong>student</strong> <strong>dependent</strong> is required before prescription drug benefits are paid.<br />
• If the form is not returned within thirty (30) days, you will be notified that the claim has been denied. The claim will be reprocessed for<br />
payment only upon receipt of the properly completed Full-Time Student Dependent Certification form.<br />
• When a <strong>dependent</strong> of yours is no longer a <strong>full</strong>-<strong>time</strong> <strong>student</strong>, you must call Medco Health at 1-800-662-8269.<br />
For a prescription claim return Full-Time Student Dependent Certification form to:<br />
Medco Health Solutions of North Versailles, L.L.C.<br />
Attn: Eligibility Department<br />
1810 Lincoln Highway<br />
North Versailles, PA 15137<br />
Fax Number: 412-829-3245<br />
Dental Benefits Program:<br />
Dependent Certification is a service that <strong>United</strong> <strong>Concordia</strong> provides to its members. Prior to when your <strong>dependent</strong> child attains the limiting age<br />
of coverage, <strong>United</strong> <strong>Concordia</strong> will send you a Dependent Certification Form to determine if your child is eligible for <strong>student</strong> <strong>dependent</strong><br />
status.<br />
The Dependent Certification Form you receive must be returned within thirty (30) days in order to ensure <strong>time</strong>ly processing. Completed forms<br />
should be sent to: Dependent Certification, <strong>United</strong> <strong>Concordia</strong> Companies, P.O. Box 69417, Harrisburg, PA 17106-9417.<br />
Form # IA-200 rev. 7/05