The Impact on Glaucoma from the OUTSIDE IN - New York Eye and ...
The Impact on Glaucoma from the OUTSIDE IN - New York Eye and ...
The Impact on Glaucoma from the OUTSIDE IN - New York Eye and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<str<strong>on</strong>g>The</str<strong>on</strong>g> <str<strong>on</strong>g>Impact</str<strong>on</strong>g><br />
<strong>on</strong> <strong>Glaucoma</strong><br />
<strong>from</strong> <strong>the</strong><br />
<strong>OUTSIDE</strong> <strong>IN</strong><br />
Highlights From an<br />
Experts Roundtable<br />
Discussi<strong>on</strong><br />
Sp<strong>on</strong>sored by <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary<br />
In joint sp<strong>on</strong>sorship with<br />
This c<strong>on</strong>tinuing medical educati<strong>on</strong> activity is supported through<br />
an unrestricted educati<strong>on</strong>al grant <strong>from</strong> Merck & Co, Inc.<br />
Richard K. Parrish II, MD—Chair<br />
Le<strong>on</strong> W. Hernd<strong>on</strong>, MD<br />
Richard A. Lewis, MD<br />
Marlene R. Moster, MD<br />
Stephen C. Pflugfelder, MD<br />
Distributed with<br />
Original Release: July 15, 2012 • Last Review: June 26, 2012 • Expirati<strong>on</strong>: July 30, 2013
How OSD Affects IOP<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> <str<strong>on</strong>g>Impact</str<strong>on</strong>g> <strong>on</strong> <strong>Glaucoma</strong><br />
<strong>OUTSIDE</strong> <strong>IN</strong><br />
FACULTY<br />
<strong>from</strong> <strong>the</strong><br />
Richard K. Parrish II, MD—Chair<br />
Associate Dean for Graduate Medical Educati<strong>on</strong><br />
Professor of Ophthalmology<br />
University of Miami Miller School of Medicine<br />
Bascom Palmer <strong>Eye</strong> Institute<br />
Miami, Florida<br />
Le<strong>on</strong> W. Hernd<strong>on</strong>, MD<br />
Associate Professor of Ophthalmology<br />
Duke University School of Medicine<br />
Durham, North Carolina<br />
Richard A. Lewis, MD<br />
Grutzmacher, Lewis & Sierra<br />
Sacramento, California<br />
Marlene R. Moster, MD<br />
Professor of Ophthalmology<br />
Thomas Jeffers<strong>on</strong> University School of Medicine<br />
Attending Surge<strong>on</strong><br />
<strong>Glaucoma</strong> Service<br />
Wills <strong>Eye</strong> Institute<br />
Philadelphia, Pennsylvania<br />
Stephen C. Pflugfelder, MD<br />
Professor of Ophthalmology<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> James <strong>and</strong> Margaret Elkins Chair<br />
Baylor College of Medicine<br />
Houst<strong>on</strong>, Texas<br />
LEARN<strong>IN</strong>G METHOD AND MEDIUM<br />
This educati<strong>on</strong>al activity c<strong>on</strong>sists of a supplement <strong>and</strong> ten (10) study questi<strong>on</strong>s.<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> participant should, in order, read <strong>the</strong> learning objectives c<strong>on</strong>tained at <strong>the</strong><br />
beginning of this supplement, read <strong>the</strong> supplement, answer all questi<strong>on</strong>s in <strong>the</strong><br />
post test, <strong>and</strong> complete <strong>the</strong> evaluati<strong>on</strong> form. To receive credit for this activity,<br />
please follow <strong>the</strong> instructi<strong>on</strong>s provided <strong>on</strong> <strong>the</strong> post test <strong>and</strong> evaluati<strong>on</strong> form.<br />
This educati<strong>on</strong>al activity should take a maximum of 1.5 hours to complete.<br />
CONTENT SOURCE<br />
This c<strong>on</strong>tinuing medical educati<strong>on</strong> (CME) activity captures c<strong>on</strong>tent <strong>from</strong> an experts<br />
roundtable discussi<strong>on</strong> held <strong>on</strong> April 17, 2012.<br />
ACTIVITY DESCRIPTION<br />
This activity will address <strong>the</strong> prevalence <strong>and</strong> clinical significance of ocular surface<br />
disease in patients with ocular hypertensi<strong>on</strong>/glaucoma, how to diagnose ocular<br />
surface disease in <strong>the</strong>se patients, <strong>the</strong> role of preservatives in ocular surface<br />
disease, current treatment opti<strong>on</strong>s <strong>and</strong> patient management.<br />
LEARN<strong>IN</strong>G OBJECTIVES<br />
Up<strong>on</strong> completi<strong>on</strong> of this activity, you will have improved your ability to:<br />
• State <strong>the</strong> prevalence of ocular surface disorders in patients with glaucoma or<br />
ocular hypertensi<strong>on</strong> • Describe <strong>the</strong> effects of preservatives in glaucoma<br />
medicati<strong>on</strong>s <strong>on</strong> <strong>the</strong> ocular surface • Identify <strong>the</strong>rapeutic approaches for patients<br />
with glaucoma or ocular hypertensi<strong>on</strong> that maintain or improve ocular surface<br />
health • Incorporate new strategies for improving <strong>the</strong>rapeutic adherence in<br />
patients with glaucoma or ocular hypertensi<strong>on</strong><br />
TARGET AUDIENCE<br />
This educati<strong>on</strong>al activity is intended for comprehensive ophthalmologists <strong>and</strong><br />
glaucoma specialists in <strong>the</strong> United States.<br />
ACCREDITATION STATEMENT<br />
This activity has been planned <strong>and</strong> implemented in accordance with <strong>the</strong> Essential<br />
Areas <strong>and</strong> Policies of <strong>the</strong> Accreditati<strong>on</strong> Council for C<strong>on</strong>tinuing Medical Educati<strong>on</strong><br />
through <strong>the</strong> joint sp<strong>on</strong>sorship of <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary <strong>and</strong><br />
MedEdicus LLC. <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary is accredited by <strong>the</strong> ACCME<br />
to provide c<strong>on</strong>tinuing medical educati<strong>on</strong> for physicians.<br />
AMA CREDIT DESIGNATION STATEMENT<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary designates this enduring material for a<br />
maximum of 1.5 AMA PRA Category 1 Credits. Physicians should claim <strong>on</strong>ly <strong>the</strong><br />
credit commensurate with <strong>the</strong> extent of <strong>the</strong>ir participati<strong>on</strong> in <strong>the</strong> activity.<br />
GRANTOR STATEMENT<br />
This c<strong>on</strong>tinuing medical educati<strong>on</strong> activity is supported through an unrestricted<br />
educati<strong>on</strong>al grant <strong>from</strong> Merck & Co, Inc.<br />
MISSION STATEMENT<br />
It is <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary Institute for C<strong>on</strong>tinuing Medical Educati<strong>on</strong>’s<br />
stated missi<strong>on</strong> to create medical educati<strong>on</strong> activities that will serve to increase <strong>the</strong><br />
knowledge, skills, professi<strong>on</strong>al performance, <strong>and</strong> relati<strong>on</strong>ships that a physician uses<br />
to provide services for patients, <strong>the</strong> public, or <strong>the</strong> chosen professi<strong>on</strong>.<br />
DISCLOSURE POLICY STATEMENT<br />
It is <strong>the</strong> policy of <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary that <strong>the</strong> faculty <strong>and</strong> any<strong>on</strong>e in<br />
a positi<strong>on</strong> to c<strong>on</strong>trol activity c<strong>on</strong>tent disclose any real or apparent c<strong>on</strong>flicts of interest<br />
relating to <strong>the</strong> topics of this educati<strong>on</strong>al activity, <strong>and</strong> also disclose discussi<strong>on</strong>s of<br />
unlabeled/unapproved uses of drugs or devices during <strong>the</strong>ir presentati<strong>on</strong>(s). <str<strong>on</strong>g>The</str<strong>on</strong>g><br />
<strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary has established policies in place that will identify<br />
<strong>and</strong> resolve all c<strong>on</strong>flicts of interest prior to this educati<strong>on</strong>al activity. Full disclosure of<br />
faculty/planner <strong>and</strong> <strong>the</strong>ir commercial relati<strong>on</strong>ships, if any, follows.<br />
FACULTY DISCLOSURES<br />
Le<strong>on</strong> W. Hernd<strong>on</strong>, MD, had a financial agreement or affiliati<strong>on</strong> during <strong>the</strong> past year<br />
with <strong>the</strong> following commercial interests in <strong>the</strong> form of H<strong>on</strong>oraria: Alc<strong>on</strong>, Inc; <strong>and</strong><br />
Reichert Technologies.<br />
Richard A. Lewis, MD, had a financial agreement or affiliati<strong>on</strong> during <strong>the</strong> past year<br />
with <strong>the</strong> following commercial interests in <strong>the</strong> form of H<strong>on</strong>oraria: Alc<strong>on</strong>, Inc;<br />
Allergan, Inc; <strong>and</strong> Merck & Co, Inc; C<strong>on</strong>sultant/Advisory Board: Aerie<br />
Pharmaceuticals, Inc; Alc<strong>on</strong>, Inc; Allergan, Inc; AqueSys Inc; iScience Interventi<strong>on</strong>al<br />
Corporati<strong>on</strong>; Ivantis; <strong>and</strong> Santen Pharmaceutical Co, Ltd.<br />
Marlene R. Moster, MD, had a financial agreement or affiliati<strong>on</strong> during <strong>the</strong> past<br />
year with <strong>the</strong> following commercial interests in <strong>the</strong> form of C<strong>on</strong>sultant/Advisory<br />
Board: Alc<strong>on</strong>, Inc; Allergan, Inc; <strong>and</strong> Merck & Co, Inc; H<strong>on</strong>oraria for Lectures: Alc<strong>on</strong>,<br />
Inc; Allergan, Inc; Bausch + Lomb Incorporated; ISTA Pharmaceuticals, Inc; <strong>and</strong><br />
Merck & Co, Inc; C<strong>on</strong>tracted Research: Ae<strong>on</strong> Optical Inc; Aerie Pharmaceuticals,<br />
Inc; Alc<strong>on</strong>, Inc; Allergan, Inc; Genentech, Inc; IOP Ophthalmics; <strong>and</strong> Solx, Inc.<br />
Richard K. Parrish II, MD, had a financial agreement or affiliati<strong>on</strong> during <strong>the</strong> past<br />
year with <strong>the</strong> following commercial interests in <strong>the</strong> form of C<strong>on</strong>sultant/Advisory<br />
Board: Aerie Pharmaceuticals, Inc; Alimera Sciences; Allergan, Inc; AqueSys Inc;<br />
Bausch + Lomb Incorporated; Glaukos Corporati<strong>on</strong>; InnFocus, Inc; Innovia LLC; <strong>and</strong><br />
Merck & Co, Inc.<br />
Stephen C. Pflugfelder, MD, had a financial agreement or affiliati<strong>on</strong> during <strong>the</strong> past<br />
year with <strong>the</strong> following commercial interests in <strong>the</strong> form of C<strong>on</strong>sultant/Advisory<br />
Board: Allergan, Inc; GlaxoSmithKline; Merck & Co, Inc; <strong>and</strong> Mimetogen<br />
Pharmaceuticals; C<strong>on</strong>tracted Research: Allergan, Inc; <strong>and</strong> GlaxoSmithKline.<br />
PEER REVIEW DISCLOSURES<br />
Ted M. Gerszberg, MD, has no relevant commercial relati<strong>on</strong>ships to disclose.<br />
EDITORIAL SUPPORT DISCLOSURES<br />
Derek Dore, PharmD; Cynthia Tornallyay, RD, MBA, CCMEP; Kimberly Corbin,<br />
CCMEP; <strong>and</strong> Barbara Ly<strong>on</strong> have no relevant commercial relati<strong>on</strong>ships to disclose.<br />
DISCLOSURE ATTESTATION<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> c<strong>on</strong>tributing physicians listed above have attested to <strong>the</strong> following:<br />
1) that <strong>the</strong> relati<strong>on</strong>ships/affiliati<strong>on</strong>s noted will not bias or o<strong>the</strong>rwise influence <strong>the</strong>ir<br />
involvement in this activity; 2) that practice recommendati<strong>on</strong>s given relevant to <strong>the</strong><br />
companies with whom <strong>the</strong>y have relati<strong>on</strong>ships/affiliati<strong>on</strong>s will be supported by <strong>the</strong><br />
best available evidence or, absent evidence, will be c<strong>on</strong>sistent with generally<br />
accepted medical practice; <strong>and</strong> 3) that all reas<strong>on</strong>able clinical alternatives will be<br />
discussed when making practice recommendati<strong>on</strong>s.<br />
OFF-LABEL DISCUSSION<br />
This activity does not include discussi<strong>on</strong> of any off-label use.<br />
SYSTEM REQUIREMENTS FOR DIGITAL EDITIONS<br />
If you are viewing this activity <strong>on</strong>line, please ensure <strong>the</strong> computer you plan to use<br />
meets <strong>the</strong> following requirements:<br />
• Operating System: Windows or Macintosh<br />
• Media Viewing Requirements: Flash Player or Adobe Reader<br />
• Supported Browsers: Microsoft Internet Explorer, Firefox, Google Chrome,<br />
Safari, <strong>and</strong> Opera<br />
• A good Internet c<strong>on</strong>necti<strong>on</strong><br />
TO OBTA<strong>IN</strong> AMA PRA CATEGORY 1 CREDIT<br />
To obtain AMA PRA Category 1 Credit for this activity, read <strong>the</strong> material in its<br />
entirety <strong>and</strong> c<strong>on</strong>sult referenced sources as necessary. We offer instant certificate<br />
processing <strong>and</strong> support Green CE. Please take this post test <strong>and</strong> evaluati<strong>on</strong> <strong>on</strong>line by<br />
going to www.MedEdicus.com <strong>and</strong> clicking <strong>the</strong> Educati<strong>on</strong>al Activities & Post Test<br />
Center box. Up<strong>on</strong> passing, you will receive your certificate immediately. You must<br />
score 70% or higher to receive credit for this activity, <strong>and</strong> may take <strong>the</strong> test up to two<br />
times. Up<strong>on</strong> registering <strong>and</strong> successfully completing <strong>the</strong> post test, your certificate will<br />
be made available <strong>on</strong>line <strong>and</strong> you can print it or file it. <str<strong>on</strong>g>The</str<strong>on</strong>g>re are no fees for<br />
participating <strong>and</strong> receiving CME credit for this activity.<br />
Alternatively, you may complete <strong>the</strong> evaluati<strong>on</strong> form al<strong>on</strong>g with <strong>the</strong> post test answer<br />
box within this supplement. Remove <strong>the</strong> Activity Evaluati<strong>on</strong> page <strong>from</strong> <strong>the</strong> printed<br />
supplement or print <strong>the</strong> Activity Evaluati<strong>on</strong> page <strong>from</strong> <strong>the</strong> Digital Editi<strong>on</strong>. Return via<br />
mail or fax to Kim Corbin, Director, ICME, <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary, 310<br />
East 14th Street, <strong>New</strong> <strong>York</strong>, NY 10003 or fax to (212) 353-5703. Your certificate<br />
will be mailed to <strong>the</strong> address that you provide <strong>on</strong> <strong>the</strong> evaluati<strong>on</strong> form. Please allow<br />
3 weeks for mailed/faxed forms to be processed.<br />
DISCLAIMER<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> views <strong>and</strong> opini<strong>on</strong>s expressed in this educati<strong>on</strong>al activity are those of <strong>the</strong><br />
faculty <strong>and</strong> do not necessarily represent <strong>the</strong> views of <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear<br />
Infirmary; MedEdicus LLC; Merck & Co, Inc; or Ophthalmology Times. Please refer<br />
to <strong>the</strong> official prescribing informati<strong>on</strong> for each product for discussi<strong>on</strong> of approved<br />
indicati<strong>on</strong>s, c<strong>on</strong>traindicati<strong>on</strong>s, <strong>and</strong> warnings.<br />
This CME activity is copyrighted to MedEdicus LLC ©2012. All rights reserved.<br />
2
Recently, 4 glaucoma specialists <strong>and</strong> 1 cornea specialist<br />
c<strong>on</strong>vened to discuss <strong>the</strong> evidence-based literature <strong>and</strong> <strong>the</strong>ir<br />
insights relevant to <strong>the</strong> intersecti<strong>on</strong> of ocular surface health<br />
<strong>and</strong> IOP management. This CME activity summarizes<br />
highlights <strong>from</strong> <strong>the</strong> discussi<strong>on</strong> <strong>and</strong> shares <strong>the</strong> faculty’s<br />
expertise regarding <strong>the</strong> prevalence of OSD in patients with<br />
glaucoma or ocular hypertensi<strong>on</strong>, <strong>the</strong> effects of preservatives<br />
in ocular antihypertensives <strong>on</strong> <strong>the</strong> ocular surface, <strong>and</strong><br />
<strong>the</strong>rapeutic approaches to improve patient outcomes.<br />
<strong>IN</strong>TRODUCTION<br />
Historically, <strong>the</strong> health of <strong>the</strong> ocular surface in patients with<br />
glaucoma or ocular hypertensi<strong>on</strong> has been overlooked <strong>and</strong><br />
underappreciated by both comprehensive ophthalmologists<br />
<strong>and</strong> glaucoma specialists. <strong>Eye</strong> care clinicians have focused<br />
<strong>on</strong> <strong>the</strong> reducti<strong>on</strong> of intraocular pressure (IOP), <strong>and</strong> often<br />
have not c<strong>on</strong>sidered <strong>the</strong> c<strong>on</strong>sequences of patients’ red,<br />
weepy, <strong>and</strong> uncomfortable eyes. Poor ocular surface health<br />
has been c<strong>on</strong>sidered <strong>the</strong> price to pay for c<strong>on</strong>trol of IOP.<br />
Recently, eye care clinicians have recognized <strong>the</strong> importance<br />
of maintaining ocular surface health when managing IOP.<br />
Studies show that approximately 50% of patients with<br />
glaucoma or ocular hypertensi<strong>on</strong> treated with ocular<br />
antihypertensives have symptoms c<strong>on</strong>sistent with ocular<br />
surface disease (OSD). 1,2,3 Moreover, <strong>the</strong> evidence indicates<br />
that <strong>the</strong>re is a direct correlati<strong>on</strong> between <strong>the</strong> number of<br />
instilled drops <strong>and</strong> <strong>the</strong> severity of OSD symptoms. 1,2,3<br />
Fortunately, <strong>the</strong> l<strong>and</strong>scape of IOP-lowering medicati<strong>on</strong>s has<br />
changed to include products that are kinder to <strong>and</strong> gentler <strong>on</strong><br />
<strong>the</strong> ocular surface. Patients may no l<strong>on</strong>ger need to trade a<br />
healthy ocular surface for c<strong>on</strong>trol of IOP.<br />
—Richard K. Parrish II, MD<br />
EYE CARE CL<strong>IN</strong>ICIANS’ OBSERVATIONS<br />
OF OCULAR SURFACE DISEASE<br />
<strong>IN</strong> PATIENTS WITH GLAUCOMA<br />
OR OCULAR HYPERTENSION<br />
Dr Parrish: Dr Pflugfelder, as a cornea <strong>and</strong> external eye disease<br />
specialist, what are typical findings of OSD in patients with<br />
glaucoma or ocular hypertensi<strong>on</strong>?<br />
Dr Pflugfelder: <str<strong>on</strong>g>The</str<strong>on</strong>g>re is no universal presentati<strong>on</strong>; however,<br />
patients often complain of ocular discomfort, particularly <strong>from</strong><br />
<strong>the</strong> administrati<strong>on</strong> of ocular medicati<strong>on</strong>s. Signs of OSD include<br />
redness of <strong>the</strong> eye, pathology of <strong>the</strong> corneal epi<strong>the</strong>lium, <strong>and</strong><br />
severe posterior lid margin disease.<br />
Dr Parrish: Dr. Moster, do you see OSD in a specific patient<br />
populati<strong>on</strong>?<br />
for cosmetic purposes <strong>and</strong> for successful treatment, including<br />
medical <strong>the</strong>rapy <strong>and</strong> surgical opti<strong>on</strong>s.<br />
Dr Parrish: Dr Lewis, with <strong>the</strong> patent expirati<strong>on</strong> of br<strong>and</strong>ed<br />
Xalatan ® , generic latanoprost is now available <strong>from</strong> many<br />
different manufacturers. In your practice, have you noted<br />
increased ocular surface complaints <strong>from</strong> patients who<br />
switched <strong>from</strong> <strong>the</strong> br<strong>and</strong>ed Xalatan ® to generic latanoprost?<br />
Dr Lewis: This is a bewildering issue. Each time a patient’s<br />
generic latanoprost prescripti<strong>on</strong> is refilled, he or she may<br />
receive <strong>the</strong> medicati<strong>on</strong> <strong>from</strong> a different manufacturer. In my<br />
experience, this variati<strong>on</strong> in manufacturers has been<br />
associated with inc<strong>on</strong>sistency in terms of both efficacy <strong>and</strong><br />
ocular redness.<br />
Dr Moster: I agree with Dr Lewis. Although all formulati<strong>on</strong>s of<br />
generic latanoprost should be equivalent, <strong>the</strong>re may be slight<br />
differences in <strong>the</strong> compositi<strong>on</strong> of <strong>the</strong> preservative or additi<strong>on</strong>al<br />
ingredients that may cause increased ocular surface changes.<br />
Dr Hernd<strong>on</strong>: Generic medicati<strong>on</strong>s provide an affordable<br />
<strong>the</strong>rapeutic opti<strong>on</strong> for my patients. In my practice, I have<br />
observed <strong>on</strong>ly a few circumstances in which a generic alternative<br />
has failed to uphold <strong>the</strong> efficacy of its br<strong>and</strong>-name equivalent.<br />
IMPLICATIONS OF POOR OCULAR<br />
SURFACE HEALTH <strong>IN</strong> PATIENTS WITH<br />
GLAUCOMA OR OCULAR HYPERTENSION<br />
Dr Parrish: Let us discuss <strong>the</strong> clinical implicati<strong>on</strong>s of poor<br />
ocular surface health in patients with glaucoma or ocular<br />
hypertensi<strong>on</strong>. <str<strong>on</strong>g>The</str<strong>on</strong>g> first c<strong>on</strong>siderati<strong>on</strong> relates to <strong>the</strong> practical<br />
c<strong>on</strong>sequence of patient n<strong>on</strong>adherence to a medical regimen<br />
that causes adverse effects. Our colleagues James C. Tsai,<br />
MD, <strong>and</strong> Gail F. Schwartz, MD, have reported <strong>on</strong> <strong>the</strong> obstacles<br />
to patient adherence to ocular medical <strong>the</strong>rapy caused by<br />
deleterious effects <strong>on</strong> <strong>the</strong> ocular surface. 5,6 Dr Pflugfelder, do<br />
you see suboptimal adherence to <strong>the</strong>rapy as a c<strong>on</strong>sequence of<br />
<strong>the</strong> deteriorating health of <strong>the</strong> ocular surface in patients <strong>on</strong><br />
ocular antihypertensives?<br />
Dr Pflugfelder: Yes, I receive complaints <strong>from</strong> patients who are<br />
intolerant of <strong>the</strong>ir ocular antihypertensives, <strong>and</strong> poor adherence<br />
is <strong>the</strong> outcome. Patients disc<strong>on</strong>tinue ocular agents because of<br />
blurred <strong>and</strong> fluctuating visi<strong>on</strong> due to unstable tear film <strong>and</strong><br />
corneal epi<strong>the</strong>liopathy.<br />
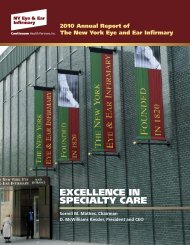
Dr Moster: Patients also disc<strong>on</strong>tinue <strong>the</strong>rapy because of <strong>the</strong><br />
unbearable symptoms <strong>the</strong>y experience. We have all seen<br />
patients who present with poorly c<strong>on</strong>trolled IOP, incredibly red<br />
irritated eyes, with superficial punctate keratitis, <strong>and</strong> poor<br />
corneal tear film. (Figure 1)<br />
Dr Moster: <str<strong>on</strong>g>The</str<strong>on</strong>g> prevalence of symptomatic OSD appears to be<br />
highest in adults aged 65 years <strong>and</strong> older. 4 Additi<strong>on</strong>ally, older<br />
adults are comm<strong>on</strong>ly bo<strong>the</strong>red by symptoms of OSD <strong>and</strong> often<br />
complain of difficulty using <strong>the</strong>ir medicati<strong>on</strong>s because of ocular<br />
irritati<strong>on</strong>.<br />
Dr Parrish: Dr Hernd<strong>on</strong>, you practice at a referral center <strong>and</strong><br />
see glaucoma patients who have OSD. What are your thoughts<br />
with respect to ocular surface health in patients with<br />
glaucoma?<br />
Dr Hernd<strong>on</strong>: I have become wiser to <strong>the</strong> importance of creating<br />
a kinder <strong>and</strong> gentler envir<strong>on</strong>ment for <strong>the</strong> ocular surface, both<br />
Figure 1. Red <strong>and</strong> inflamed eye with a cornea that has almost c<strong>on</strong>fluent<br />
superficial punctate staining. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient presented with an IOP of<br />
36 mm Hg <strong>and</strong> a failed bleb; she was put back <strong>on</strong> a topical ocular<br />
antihypertensive.<br />
Photo Courtesy of Marlene R. Moster, MD<br />
3
Dr Pflugfelder’s Top 5 Ocular Surface<br />
Assessments for <strong>the</strong> Comprehensive<br />
Ophthalmologist<br />
1. Lacrimal Puncta<br />
Are <strong>the</strong>re signs of ectropi<strong>on</strong> or stenosis of <strong>the</strong> puncta?<br />
Many older patients have ei<strong>the</strong>r a subtle ectropi<strong>on</strong> or<br />
some stenosis of <strong>the</strong>ir puncta, which will interfere with<br />
tear drainage.<br />
2. Posterior Lids (Meibomian Gl<strong>and</strong>s)<br />
Express <strong>the</strong> lids!<br />
Has gl<strong>and</strong> dropout occurred?<br />
What is <strong>the</strong> quality of <strong>the</strong> meibum?<br />
Is vascularizati<strong>on</strong> present?<br />
Many older patients also have lid margin changes due to<br />
posterior blepharitis/meibomian gl<strong>and</strong> dysfuncti<strong>on</strong>.<br />
Decreases in <strong>the</strong> quantity <strong>and</strong>/or quality of meibum lead to<br />
lipid deficiency that can destabilize <strong>the</strong> tears <strong>and</strong> potentiate<br />
<strong>the</strong> deleterious effects of ocular antihypertensives.<br />
3. Tear Film Layer<br />
What are <strong>the</strong> results of a fluorescein tear break-up time test?<br />
Fluorescein tear break-up time may be <strong>the</strong> easiest test that<br />
an eye care clinician performs. When I c<strong>on</strong>duct <strong>the</strong> test,<br />
I first moisten <strong>the</strong> fluorescein strip (any br<strong>and</strong>) with<br />
preservative-free saline, touch <strong>the</strong> patient’s inferior tarsal<br />
c<strong>on</strong>junctiva, <strong>and</strong> ask <strong>the</strong> patient to blink to disperse <strong>the</strong><br />
fluorescein. Viewing under cobalt blue illuminati<strong>on</strong>, I ask <strong>the</strong><br />
patient to blink <strong>and</strong> keep his or her eye open until I begin to<br />
observe disc<strong>on</strong>tinuities in <strong>the</strong> tear film, which usually occur<br />
in <strong>the</strong> center or <strong>the</strong> inferior cornea. I count in sec<strong>on</strong>ds to<br />
determine <strong>the</strong> amount of time it takes for <strong>the</strong> tears to break<br />
up. <str<strong>on</strong>g>The</str<strong>on</strong>g>re is some debate about what <strong>the</strong> normal tear breakup<br />
time is. I c<strong>on</strong>sider 7 sec<strong>on</strong>ds or less to be abnormal. In<br />
many older patients, tear break-up is instantaneous.<br />
4. Cornea<br />
Is erosi<strong>on</strong> present?<br />
Once fluorescein is instilled, I examine <strong>the</strong> cornea to<br />
determine <strong>the</strong> presence of punctate fluorescein staining.<br />
Staining in <strong>the</strong> center of <strong>the</strong> cornea indicates greater<br />
severity of erosi<strong>on</strong>, which has <strong>the</strong> potential to reduce visi<strong>on</strong>.<br />
5. C<strong>on</strong>junctiva<br />
Is redness present?<br />
Is c<strong>on</strong>junctival chalasis present?<br />
Redness <strong>and</strong> fluorescein staining in <strong>the</strong> c<strong>on</strong>junctiva indicate<br />
epi<strong>the</strong>lial disease. C<strong>on</strong>junctival chalasis, or loosening of <strong>the</strong><br />
c<strong>on</strong>junctiva, can interfere with <strong>the</strong> spread of tears.<br />
C<strong>on</strong>junctival chalasis tends to compartmentalize <strong>the</strong> tears,<br />
typically in <strong>the</strong> center of <strong>the</strong> lower lid, because <strong>the</strong> c<strong>on</strong>diti<strong>on</strong><br />
blocks <strong>the</strong> flow of <strong>the</strong> tear meniscus both temporally <strong>and</strong><br />
sometimes nasally. C<strong>on</strong>junctival chalasis also interferes with<br />
tear clearance <strong>and</strong> increases <strong>the</strong> c<strong>on</strong>centrati<strong>on</strong> of ocular<br />
medicati<strong>on</strong>s over <strong>the</strong> cornea.<br />
Typically with ocular antihypertensive toxicity, most of <strong>the</strong><br />
redness occurs in <strong>the</strong> lower third of <strong>the</strong> eye, <strong>on</strong> <strong>the</strong> inferior<br />
bulbar c<strong>on</strong>junctiva <strong>and</strong> <strong>the</strong> inferior tarsus, particularly<br />
medially, where <strong>the</strong> tears are swept toward <strong>the</strong> lacrimal<br />
drainage system. When I observe redness <strong>on</strong> <strong>the</strong> inferior<br />
tarsus <strong>and</strong> <strong>the</strong> patient is using 1 or more ocular<br />
antihypertensives, I suspect toxicity. (Figure 2)<br />
Dr Parrish: It is hard to believe that any<strong>on</strong>e presenting with<br />
<strong>the</strong>se signs <strong>and</strong> symptoms would be willing to c<strong>on</strong>tinue to use<br />
<strong>the</strong> medicati<strong>on</strong>s that we prescribe.<br />
Dr Pflugfelder: Certainly, this presentati<strong>on</strong> can negatively affect<br />
patient quality of life (QOL). In fact, evidence suggests that dry<br />
eye adversely affects QOL at a magnitude similar to that<br />
caused by unstable angina. 7<br />
Dr Moster: A patient’s ability to be productive in <strong>the</strong> workforce<br />
also can be affected by symptoms of dry eye, which inhibit an<br />
individual’s ability to keep visually focused for an extended<br />
period of time. Given <strong>the</strong>se critical financial times, people must<br />
be able to work l<strong>on</strong>g hours. If <strong>the</strong>y are uncomfortable doing <strong>the</strong>ir<br />
job, <strong>the</strong> cause of <strong>the</strong> discomfort―ocular antihypertensives―will<br />
most likely be <strong>the</strong> first thing to be eliminated by <strong>the</strong> patients in<br />
an effort to reduce <strong>the</strong> discomfort. Such an acti<strong>on</strong> will likely<br />
lead to worsening of existing glaucoma.<br />
Dr Lewis: This is an important point, particularly with today’s<br />
computer-related occupati<strong>on</strong>s. Most workers spend many<br />
hours working in fr<strong>on</strong>t of a video display terminal, which leads<br />
to a decrease in blink rate <strong>and</strong>, c<strong>on</strong>sequently, a form of<br />
occupati<strong>on</strong>al stress that exacerbates an already unstable tear<br />
film brought <strong>on</strong> by <strong>the</strong> use of glaucoma medicati<strong>on</strong>s.<br />
Dr Moster: Older, retired glaucoma patients are spending<br />
significant amounts of time at <strong>the</strong> computer as well, reading<br />
e-mail messages <strong>and</strong> searching <strong>the</strong> Internet. <str<strong>on</strong>g>The</str<strong>on</strong>g> need to limit<br />
this time because of OSD symptoms may negatively affect<br />
<strong>the</strong>ir QOL.<br />
ASSESSMENT OF THE OCULAR SURFACE<br />
<strong>IN</strong> PATIENTS WITH GLAUCOMA OR<br />
OCULAR HYPERTENSION<br />
Dr Parrish: Dr Pflugfelder, what is your recommendati<strong>on</strong> to a<br />
comprehensive ophthalmologist without research tools <strong>and</strong><br />
advanced technologies for assessing <strong>the</strong> ocular surface?<br />
Dr Pflugfelder: Assessment of <strong>the</strong> ocular surface <strong>and</strong> <strong>the</strong> lids<br />
necessitates some effort <strong>on</strong> <strong>the</strong> part of <strong>the</strong> ophthalmologist;<br />
<strong>the</strong> clinician, however, can quickly become efficient at <strong>the</strong><br />
evaluati<strong>on</strong>. (see Sidebar)<br />
Dr Parrish: Regarding OSD, many eye care clinicians report that<br />
patient-reported symptoms <strong>and</strong> clinical signs do not always<br />
correlate. What is <strong>the</strong> rati<strong>on</strong>ale for this disc<strong>on</strong>nect?<br />
Dr Pflugfelder: This is certainly a paradox in <strong>the</strong> world of<br />
ophthalmology. It turns out that some patients with <strong>the</strong> most<br />
severe corneal epi<strong>the</strong>lial disease have <strong>the</strong> least troublesome<br />
symptoms. Patients with l<strong>on</strong>g-st<strong>and</strong>ing OSD may develop nerve<br />
Figure 2. Injecti<strong>on</strong> of<br />
c<strong>on</strong>junctival blood vessels in<br />
<strong>the</strong> inferior tarsal <strong>and</strong> bulbar<br />
c<strong>on</strong>junctiva of a patient<br />
chr<strong>on</strong>ically treated with<br />
latanoprost.<br />
Photo Courtesy of<br />
Stephen C. Pflugfelder, MD<br />
4
Typically with ocular antihypertensive toxicity, most of<br />
<strong>the</strong> redness occurs in <strong>the</strong> lower third of <strong>the</strong> eye, <strong>on</strong><br />
<strong>the</strong> inferior bulbar c<strong>on</strong>junctiva <strong>and</strong> <strong>the</strong> inferior tarsus,<br />
particularly medially, where <strong>the</strong> tears are swept<br />
toward <strong>the</strong> lacrimal drainage system. When I observe<br />
redness <strong>on</strong> <strong>the</strong> inferior tarsus <strong>and</strong> <strong>the</strong> patient is using<br />
1 or more ocular antihypertensives, I suspect toxicity.<br />
—Stephen C. Pflugfelder, MD<br />
degenerati<strong>on</strong>. C<strong>on</strong>sequently, <strong>the</strong>y develop relative corneal<br />
anes<strong>the</strong>sia, <strong>and</strong> stop complaining of symptoms. C<strong>on</strong>versely,<br />
some patients with early stages of OSD <strong>and</strong> minimal<br />
epi<strong>the</strong>liopathy complain bitterly. In early-stage OSD, <strong>the</strong>re may<br />
be an inflammatory-mediated hyperes<strong>the</strong>sia of <strong>the</strong> nerve,<br />
similar to that which occurs in a chr<strong>on</strong>ic pain syndrome.<br />
CAUSES OF OCULAR SURFACE DISEASE<br />
AND PATIENTS AT RISK<br />
Dr Parrish: What are some of <strong>the</strong> extrinsic <strong>and</strong> intrinsic causes<br />
of OSD?<br />
Dr Lewis: In terms of extrinsic causes, geography can play a<br />
part. In Sacramento, California, where I practice, <strong>the</strong> humidity<br />
is low compared with many o<strong>the</strong>r regi<strong>on</strong>s of <strong>the</strong> United States.<br />
C<strong>on</strong>sequently, we note a dry eye problem, particularly in <strong>the</strong><br />
spring <strong>and</strong> summer. In additi<strong>on</strong>, my practice is in a farming<br />
valley, where <strong>the</strong>re is exposure to many allergens. When<br />
<strong>the</strong>se envir<strong>on</strong>mental causes of OSD are combined with<br />
blepharoc<strong>on</strong>junctivitis, c<strong>on</strong>tact lens wear, or <strong>the</strong> toxic effects<br />
of preservatives in ocular medical <strong>the</strong>rapy, patients experience<br />
significant discomfort.<br />
Dr Parrish: Meibomian gl<strong>and</strong> dysfuncti<strong>on</strong> is an important<br />
intrinsic cause of OSD, particularly subclinical evaporative dry<br />
eye in older adults.<br />
Dr Hernd<strong>on</strong>: With older age, I certainly see eyelid issues as a<br />
c<strong>on</strong>tributor. Thus, I pay close attenti<strong>on</strong> to <strong>the</strong> impact of<br />
ectropi<strong>on</strong> or entropi<strong>on</strong> <strong>on</strong> <strong>the</strong> ocular surface.<br />
Dr Lewis: Although Sjögren syndrome is cited as an associated<br />
systemic finding with OSD, 8 I do not observe <strong>the</strong> syndrome as a<br />
comm<strong>on</strong> c<strong>on</strong>comitant c<strong>on</strong>diti<strong>on</strong>. I do, however, see c<strong>on</strong>nective<br />
tissue diseases as a comm<strong>on</strong> comorbidity. Interestingly, I find<br />
that female patients complain more about red eye <strong>and</strong> irritati<strong>on</strong>,<br />
even though I see <strong>the</strong> problem more often in male patients.<br />
Dr Pflugfelder: I agree with Dr Lewis: in my experience, male<br />
patients complain less often than female patients, which is<br />
counterintuitive, because women typically have a higher pain<br />
threshold than men.<br />
Dr Parrish: In my experience, male patients are more likely than<br />
female patients to develop severe rosacea <strong>and</strong> c<strong>on</strong>comitant<br />
keratitis or lid margin disease.<br />
Dr Pflugfelder: In additi<strong>on</strong> to <strong>the</strong> autoimmune c<strong>on</strong>diti<strong>on</strong>s, I often<br />
see 2 diseases in <strong>the</strong> elderly that affect <strong>the</strong> ocular surface:<br />
diabetes <strong>and</strong> Parkins<strong>on</strong> disease. When patients with diabetes<br />
develop neuropathy that affects <strong>the</strong> corneal nerves, <strong>the</strong> result is<br />
a decrease in blink rate, which diminishes <strong>the</strong> spread of tears.<br />
Likewise, patients with moderate-to-severe Parkins<strong>on</strong> disease<br />
do not blink often, which results in tear stagnati<strong>on</strong> al<strong>on</strong>g <strong>the</strong><br />
lower lid <strong>and</strong> <strong>the</strong> development of blepharitis. Also, certain<br />
antidepressants, urinary antispasmodics, <strong>and</strong> antihistamines<br />
should be c<strong>on</strong>sidered potential extrinsic causes of OSD.<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> anticholinergic effects of <strong>the</strong>se comm<strong>on</strong>ly prescribed<br />
medicati<strong>on</strong>s can reduce tear producti<strong>on</strong>. 9<br />
THE EFFECTS OF PRESERVATIVES<br />
ON OCULAR STRUCTURES<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> Effects of Preservatives <strong>on</strong><br />
<strong>the</strong> Ocular Surface<br />
Dr Parrish: Most commercially available ocular<br />
antihypertensives c<strong>on</strong>tain preservatives, <strong>and</strong> <strong>the</strong> most<br />
comm<strong>on</strong>ly employed preservative is benzalk<strong>on</strong>ium chloride<br />
(BAK). <str<strong>on</strong>g>The</str<strong>on</strong>g> deleterious effects of BAK <strong>on</strong> <strong>the</strong> ocular surface<br />
have received a great deal of attenti<strong>on</strong>. Dr Pflugfelder, can you<br />
provide an evidence-based summary of <strong>the</strong> safety of BAK as a<br />
preservative in ocular preparati<strong>on</strong>s?<br />
Dr Pflugfelder: <str<strong>on</strong>g>The</str<strong>on</strong>g> literature is replete with various toxic<br />
effects of BAK in in vitro c<strong>on</strong>junctival <strong>and</strong> corneal epi<strong>the</strong>lial cell<br />
models, 10,11,12 in vivo animal models, 13,14,15 <strong>and</strong> clinical trials. 16<br />
BAK is a detergent, <strong>and</strong> as such, <strong>the</strong> chemical compound can<br />
have direct effects <strong>on</strong> <strong>the</strong> lipid layer in <strong>the</strong> cell membrane. BAK<br />
has been found to disrupt <strong>the</strong> corneal epi<strong>the</strong>lial tight juncti<strong>on</strong><br />
proteins, particularly occludin, which results in loss of <strong>the</strong><br />
barrier functi<strong>on</strong> in <strong>the</strong> apical epi<strong>the</strong>lium <strong>and</strong> in rapid loss of<br />
cells. This may account for <strong>the</strong> observed epi<strong>the</strong>liopathy with<br />
BAK. 11 And, in <strong>the</strong> c<strong>on</strong>centrati<strong>on</strong>s present in commercially<br />
available ocular preparati<strong>on</strong>s, BAK can also cause programmed<br />
cell death, apoptosis, <strong>and</strong> necrosis in epi<strong>the</strong>lial cells. 10-12,15,17<br />
BAK also has been found to incite various inflammatory<br />
mediators, including cytokines, chemotactic factors, <strong>and</strong><br />
metalloproteinases that fur<strong>the</strong>r cause loss of cells. 18-20<br />
Dr Parrish: Additi<strong>on</strong>ally, a recent study by Sarkar <strong>and</strong><br />
colleagues showed that <strong>the</strong> applicati<strong>on</strong> of BAK elicited corneal<br />
neurotoxicity <strong>and</strong> reduced aqueous tear producti<strong>on</strong> in vivo <strong>and</strong><br />
in vitro in mouse eyes. 21 Although mouse eyes may not be<br />
analogous to human eyes, <strong>the</strong> findings show <strong>the</strong> depth <strong>and</strong><br />
breadth of BAK’s deleterious effects. Clinical evidence has<br />
dem<strong>on</strong>strated BAK’s dose-dependent relati<strong>on</strong>ship with OSD <strong>and</strong><br />
its negative effect <strong>on</strong> patient QOL. 1-3,22<br />
Dr Moster: Patients using multiple topical agents are being<br />
overexposed to BAK. <str<strong>on</strong>g>The</str<strong>on</strong>g> negative effect BAK has <strong>on</strong> <strong>the</strong> ocular<br />
surface may be in part resp<strong>on</strong>sible for <strong>the</strong> symptomatology we<br />
so often observe in clinical practice. 1-3<br />
Dr Hernd<strong>on</strong>: BAK’s detergent-like properties became clear to<br />
me at, of all places, a local rib restaurant. Following my meal, I<br />
proceeded to open a wet nap package. I noticed <strong>the</strong> active<br />
ingredient of <strong>the</strong> cleanser was BAK. (Figure 3)<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> Effects of Preservatives<br />
<strong>on</strong> <strong>the</strong> Trabecular Meshwork<br />
Figure 3. Example of a wet nap<br />
product, with BAK as <strong>the</strong> cleanser,<br />
comm<strong>on</strong>ly provided in restaurant<br />
settings.<br />
Photo Courtesy of<br />
Le<strong>on</strong> W. Hernd<strong>on</strong>, MD<br />
Dr Parrish: It is difficult to accept <strong>the</strong> noti<strong>on</strong> that as clinicians,<br />
we may be harming <strong>the</strong> eye’s internal structures (ie, trabecular<br />
meshwork) with <strong>the</strong> medicine that we prescribe. However, <strong>the</strong><br />
5
work of Ammar <strong>and</strong> Kahook 18,23 <strong>and</strong> that of Zhang <strong>and</strong><br />
colleagues 17 suggest that <strong>the</strong> toxic effects of BAK may not be<br />
limited to <strong>the</strong> external surface of <strong>the</strong> eye, but that BAK may<br />
actually penetrate through corneal skeletal limbal tissue <strong>and</strong><br />
thus both trabecular endo<strong>the</strong>lial cells <strong>and</strong> n<strong>on</strong>-pigmented ciliary<br />
epi<strong>the</strong>lial lines are also affected. What is your belief regarding<br />
this evidence?<br />
Dr Moster: A single drop of a BAK-c<strong>on</strong>taining ocular medicati<strong>on</strong><br />
can persist in ocular tissues for an extended period of time 24 ;<br />
thus, I believe <strong>the</strong>re is a str<strong>on</strong>g possibility that BAK can enter<br />
into <strong>and</strong> persist within internal tissues.<br />
Dr Hernd<strong>on</strong>: Before forming a definitive opini<strong>on</strong> <strong>on</strong> this issue, I<br />
would like to see more evidence showing BAK’s toxicity <strong>on</strong> <strong>the</strong><br />
trabecular meshwork.<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> Effects of Preservatives<br />
<strong>on</strong> Surgical Outcomes<br />
Dr Parrish: Some evidence suggests that <strong>the</strong> l<strong>on</strong>g-term use of<br />
ocular antihypertensives is associated with failure of traditi<strong>on</strong>al<br />
trabeculectomy limbal filtrati<strong>on</strong> surgery or with complicati<strong>on</strong>s<br />
with postoperative healing. 25,26 Do you see poor surgical<br />
outcomes caused by ocular antihypertensives?<br />
Dr Hernd<strong>on</strong>: I believe that preservatives have a deleterious effect<br />
<strong>on</strong> <strong>the</strong> c<strong>on</strong>junctival surface, leading to poor surgical outcomes.<br />
This was dem<strong>on</strong>strated by <strong>the</strong> work of Broadway <strong>and</strong> colleagues<br />
approximately 20 years ago. <str<strong>on</strong>g>The</str<strong>on</strong>g>y found that <strong>the</strong> l<strong>on</strong>g-term use of<br />
multiple ocular antihypertensives induced preoperative subclinical<br />
c<strong>on</strong>junctival inflammati<strong>on</strong>, <strong>and</strong> that <strong>the</strong> l<strong>on</strong>g-term multidrug<br />
regimens were associated with lower surgical success rates<br />
compared with shorter-term m<strong>on</strong>o<strong>the</strong>rapy. Both exposure to<br />
preservatives <strong>and</strong> durati<strong>on</strong> of <strong>the</strong>rapy were cited by <strong>the</strong> authors<br />
as probable mechanisms that led to poor surgical outcomes. 25<br />
Dr Moster: I recommend a drop holiday prior to surgery, even if<br />
<strong>the</strong> patient’s IOP is high. Following a drop holiday, I often<br />
observe decreased bleeding, less irritati<strong>on</strong>, <strong>and</strong> improved<br />
surgical outcomes. An oral agent can be employed to lower <strong>the</strong><br />
IOP until <strong>the</strong> time when <strong>the</strong> patient can be brought comfortably<br />
to <strong>the</strong> operating room.<br />
Dr Parrish: Do ocular antihypertensives negatively affect<br />
outcomes of arg<strong>on</strong> laser trabeculoplasty (ALT) or selective laser<br />
trabeculoplasty (SLT)?<br />
Dr Pflugfelder: It is a possibility. Ocular antihypertensive use,<br />
specifically in terms of <strong>the</strong> inflammatory effects of BAK, has<br />
been found to be a risk factor for failure or rejecti<strong>on</strong> of corneal<br />
transplant, suggesting that <strong>the</strong> drops can gain access to <strong>the</strong><br />
anterior chamber. 27<br />
Prostagl<strong>and</strong>in-Associated Periorbitopathy<br />
Dr Parrish: Recently, prostagl<strong>and</strong>in-associated periorbitopathy<br />
(PAP), or deepening of <strong>the</strong> superior lid sulcus, has received<br />
increasing attenti<strong>on</strong> as a potential adverse effect of ocular<br />
prostagl<strong>and</strong>in ag<strong>on</strong>ists. Do you observe this phenomen<strong>on</strong> in<br />
your practice, <strong>and</strong> if so, what do you do about it?<br />
Dr Hernd<strong>on</strong>: I have clearly seen patients in my practice who<br />
have presented with deeper orbits related to <strong>the</strong> use of ocular<br />
prostagl<strong>and</strong>in analogs, particularly those who are treated in<br />
<strong>on</strong>ly 1 eye. We should give credit to both Louis R. Pasquale,<br />
MD, <strong>and</strong> Stanley J. Berke, MD, for bringing this adverse effect<br />
to <strong>the</strong> attenti<strong>on</strong> of <strong>the</strong> ocular community. In this situati<strong>on</strong>, <strong>the</strong><br />
eyelids become tighter <strong>and</strong> it can be difficult for <strong>the</strong> clinician to<br />
lift up <strong>the</strong> patient’s eyelid.<br />
Dr Moster: <str<strong>on</strong>g>The</str<strong>on</strong>g> c<strong>on</strong>diti<strong>on</strong> is sometimes referred to as<br />
pharmacologic blepharoplasty.<br />
Dr Parrish: With limited literature <strong>on</strong> this subject, it is difficult<br />
to ascertain if PAP is an effect of preservatives or of <strong>the</strong><br />
prostagl<strong>and</strong>in analog moiety. Could it be that BAK is enhancing<br />
<strong>the</strong> penetrati<strong>on</strong> of <strong>the</strong> prostagl<strong>and</strong>in analog into <strong>the</strong> periorbital<br />
tissue? Based <strong>on</strong> this hypo<strong>the</strong>sis, perhaps a preservative-free<br />
prostagl<strong>and</strong>in analog would have less extensive orbital<br />
penetrati<strong>on</strong>? For <strong>the</strong> present, <strong>the</strong>se scientific questi<strong>on</strong>s are<br />
simply speculati<strong>on</strong>.<br />
MANAG<strong>IN</strong>G PATIENTS WITH GLAUCOMA<br />
OR OCULAR HYPERTENSION AND<br />
OCULAR SURFACE ISSUES<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g>rapeutic Strategies for C<strong>on</strong>trolling IOP<br />
<strong>and</strong> Maintaining Ocular Surface Health<br />
Dr Parrish: What are <strong>the</strong> best practices for maintaining ocular<br />
surface health while managing IOP? What do you do for <strong>the</strong><br />
patient who uses ocular antihypertensives <strong>and</strong> presents with a<br />
myriad of ocular surface findings <strong>and</strong> complaints?<br />
Dr Pflugfelder: <str<strong>on</strong>g>The</str<strong>on</strong>g> best method to determine if ocular<br />
antihypertensive agents are <strong>the</strong> cause of ocular surface toxicity<br />
is to initiate a drop holiday. Thus, in patients with ocular surface<br />
toxicity, I disc<strong>on</strong>tinue all ocular antihypertensives <strong>and</strong> begin IOPlowering<br />
<strong>the</strong>rapy with an oral carb<strong>on</strong>ic anhydrase inhibitor. In<br />
severe cases, during <strong>the</strong> drop holiday, I will prescribe a low-dose,<br />
preservative-free ocular steroid to reduce inflammati<strong>on</strong> of <strong>the</strong><br />
ocular surface. <str<strong>on</strong>g>The</str<strong>on</strong>g> steroid typically accelerates improvement of<br />
<strong>the</strong> ocular surface, <strong>and</strong> interestingly, usually does not increase<br />
IOP. I typically use dexamethas<strong>on</strong>e, 0.01%, which is compounded<br />
by a specialty pharmacy. In close collaborati<strong>on</strong> with <strong>the</strong> patient’s<br />
glaucoma specialist, <strong>and</strong> with careful m<strong>on</strong>itoring of IOP, I typically<br />
c<strong>on</strong>tinue <strong>the</strong> drop holiday for a few weeks. <str<strong>on</strong>g>The</str<strong>on</strong>g>n, if <strong>the</strong> patient’s<br />
ocular surface improves, which it usually does, I resume ocular<br />
antihypertensive <strong>the</strong>rapy, but with n<strong>on</strong>-BAK preserved or<br />
preservative-free ocular antihypertensives. In some cases, I<br />
prescribe <strong>the</strong> combinati<strong>on</strong> of a low-dose oral carb<strong>on</strong>ic anhydrase<br />
inhibitor <strong>and</strong> an ocular antihypertensive.<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> best method to determine if ocular<br />
antihypertensive agents are <strong>the</strong> cause of ocular<br />
surface toxicity is to initiate a drop holiday. Thus, in<br />
patients with ocular surface toxicity, I disc<strong>on</strong>tinue<br />
all ocular antihypertensives <strong>and</strong> begin IOP-lowering<br />
<strong>the</strong>rapy with an oral carb<strong>on</strong>ic anhydrase inhibitor.<br />
—Stephen C. Pflugfelder, MD<br />
Dr Moster: Because glaucoma is a lifel<strong>on</strong>g disease, a drop<br />
holiday makes sense. As does Dr Pflugfelder, I prescribe a lowdose,<br />
preservative-free ocular steroid during <strong>the</strong> drop holiday,<br />
followed by re-initiati<strong>on</strong> of ocular antihypertensive <strong>the</strong>rapy, but<br />
with a preservative-free formulati<strong>on</strong>.<br />
Dr Parrish: Has any<strong>on</strong>e used <strong>the</strong> 1-eye trial to determine which<br />
ocular antihypertensive in a regimen is causing ocular surface<br />
distress? That is, has any<strong>on</strong>e disc<strong>on</strong>tinued 1 medicati<strong>on</strong> at a<br />
time, in 1 eye, <strong>and</strong> followed <strong>the</strong> patient to observe for<br />
improvement of ocular surface symptoms in <strong>the</strong> trial eye<br />
compared with <strong>the</strong> eye that c<strong>on</strong>tinues to be treated with <strong>the</strong><br />
original medical regimen.<br />
6
Dr Hernd<strong>on</strong>: Yes, for patients <strong>on</strong> multiple ocular antihypertensives,<br />
I use <strong>the</strong> m<strong>on</strong>ocular approach to back down <strong>on</strong> <strong>the</strong> <strong>the</strong>rapy,<br />
1 medicati<strong>on</strong> at a time.<br />
Medical <str<strong>on</strong>g>The</str<strong>on</strong>g>rapy<br />
N<strong>on</strong>-BAK Preservatives<br />
Dr Parrish: <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>on</strong>ly prostagl<strong>and</strong>in ag<strong>on</strong>ist with a n<strong>on</strong>-BAK<br />
preservative currently <strong>on</strong> <strong>the</strong> market is travoprost with SofZia.<br />
Some studies suggest that SofZia is relatively n<strong>on</strong>toxic to<br />
ocular structures. 20,28,29 What is your impressi<strong>on</strong> of <strong>the</strong> safety<br />
<strong>and</strong> tolerability of travoprost with SofZia?<br />
Dr Moster: I believe that replacing BAK with SofZia is a move in<br />
<strong>the</strong> right directi<strong>on</strong>. My patients complain less of ocular<br />
symptoms with <strong>the</strong> use of travoprost with SofZia compared with<br />
BAK-preserved ocular antihypertensives.<br />
Dr Hernd<strong>on</strong>: I have seen situati<strong>on</strong>s in which patients have<br />
experienced red eye irritati<strong>on</strong> with <strong>the</strong> use of BAK-preserved<br />
ocular antihypertensives; when switched to travoprost with<br />
SofZia, <strong>the</strong>ir ocular symptoms subsided.<br />
Dr Moster: It is important to note that <strong>the</strong> prostagl<strong>and</strong>in<br />
analog molecule itself causes hyperemia <strong>and</strong> some level of<br />
discomfort. <str<strong>on</strong>g>The</str<strong>on</strong>g>refore, eliminati<strong>on</strong> of <strong>the</strong> BAK preservative may<br />
not completely obliterate red eye in some patients. 30,31<br />
Dr Parrish: I am curious about your thoughts <strong>on</strong> Purite as a<br />
preservative. Although Purite may not be toxic, 19 I have noted<br />
frequent toxic effects with <strong>the</strong> formulati<strong>on</strong> of <strong>the</strong> alpha-2<br />
adrenergic receptor ag<strong>on</strong>ist, brim<strong>on</strong>idine, preserved with Purite.<br />
Dr Moster: <str<strong>on</strong>g>The</str<strong>on</strong>g> brim<strong>on</strong>idine moiety itself can be an allergen. 32<br />
In my experience, <strong>the</strong> <strong>on</strong>ly factor that appears to limit<br />
brim<strong>on</strong>idine’s ocular toxicity is when it is formulated in<br />
combinati<strong>on</strong> with timolol.<br />
Dr Pflugfelder: I believe that SofZia <strong>and</strong> Purite are gentler <strong>on</strong><br />
<strong>the</strong> ocular surface compared with BAK. Some studies suggest<br />
that SofZia <strong>and</strong> Purite are less toxic to <strong>the</strong> epi<strong>the</strong>lium 19,20,28,29 ;<br />
<strong>the</strong>se findings have not, however, been clearly or c<strong>on</strong>sistently<br />
c<strong>on</strong>firmed in clinical trials. 33-36<br />
Dr Lewis: <str<strong>on</strong>g>The</str<strong>on</strong>g> early clinical trial comparing travoprost with<br />
SofZia to travoprost with BAK showed no difference in terms<br />
of efficacy <strong>and</strong> adverse events, 35 which was surprising.<br />
N<strong>on</strong>e<strong>the</strong>less, <strong>the</strong> more recent studies show that replacing<br />
BAK with an alternative preservative is more protective to <strong>the</strong><br />
ocular surface. 20,29<br />
Preservative-Free Formulati<strong>on</strong>s<br />
Dr Parrish: Recently, <strong>the</strong> much anticipated first preservativefree<br />
prostagl<strong>and</strong>in analog, preservative-free tafluprost, became<br />
available in <strong>the</strong> United States. Results <strong>from</strong> peer-reviewed<br />
clinical trials dem<strong>on</strong>strate preservative-free tafluprost’s 26% to<br />
30% IOP-lowering effect (Figure 4) <strong>and</strong> <strong>the</strong> medicati<strong>on</strong>’s<br />
equivalent IOP lowering when compared with latanoprost<br />
preserved with BAK. 30,31,37,38 In additi<strong>on</strong>, clinical studies show<br />
that preservative-free tafluprost is better tolerated than<br />
latanoprost with BAK―improving ocular comfort <strong>and</strong> quality of<br />
life in patients who experience signs <strong>and</strong> symptoms of OSD<br />
with latanoprost with BAK. 37,38 What is your perspective <strong>on</strong> <strong>and</strong><br />
clinical experience with preservative-free tafluprost?<br />
Figure 4. Mean (± 95% c<strong>on</strong>fidence interval) IOP at baseline <strong>and</strong> at 2, 6,<br />
<strong>and</strong> 12 weeks in patients with open-angle glaucoma or ocular hypertensi<strong>on</strong><br />
receiving preservative-free tafluprost or preservative-free timolol.<br />
Reprinted with permissi<strong>on</strong> <strong>from</strong> Elsevier.<br />
Dr Lewis: It is nice that we now have a preservative-free<br />
prostagl<strong>and</strong>in analog opti<strong>on</strong> to complement <strong>the</strong> preservativefree<br />
beta-blocker timolol.* In <strong>the</strong> past, we did not have<br />
preservative-free ocular antihypertensive opti<strong>on</strong>s <strong>and</strong> it was<br />
difficult to c<strong>on</strong>trol <strong>the</strong> cumulative effect of <strong>the</strong> preservatives <strong>on</strong><br />
<strong>the</strong> patient’s ocular surface, particularly when IOP c<strong>on</strong>trol<br />
required a multidrug regimen. <str<strong>on</strong>g>The</str<strong>on</strong>g> glaucoma community has<br />
been struggling with <strong>the</strong> preservative-free effort for years,<br />
searching for a safe <strong>and</strong> effective breakthrough. It is refreshing<br />
that <strong>the</strong> preservative-free effort has not been ab<strong>and</strong><strong>on</strong>ed by<br />
glaucoma specialists.<br />
Dr Moster: I have used preservative-free tafluprost in patients<br />
who are sensitive to o<strong>the</strong>r prostagl<strong>and</strong>in analog preparati<strong>on</strong>s<br />
<strong>and</strong> who have a history of dry eye. It is well tolerated <strong>and</strong><br />
efficacious in terms of lowering IOP <strong>and</strong> is a viable alternative,<br />
particularly for patients who are plagued by BAK-induced ocular<br />
adverse effects <strong>from</strong> o<strong>the</strong>r ocular antihypertensives. <str<strong>on</strong>g>The</str<strong>on</strong>g>re is a<br />
commitment needed <strong>from</strong> patients to use <strong>the</strong> single-dose<br />
c<strong>on</strong>tainers, which are recommended to be stored refrigerated<br />
when in unopened foil pouches. Once pouches are opened, <strong>the</strong><br />
single-use c<strong>on</strong>tainers may be stored at room temperature for<br />
up to 28 days. 39<br />
Dr Lewis: Early clinical trials in Europe dem<strong>on</strong>strated that<br />
preservative-free tafluprost is both safe <strong>and</strong> effective. 30,38<br />
I believe preservative-free tafluprost is used in Europe because<br />
Europeans have been very c<strong>on</strong>scious of <strong>the</strong> problems with<br />
BAK for many years now, largely because of <strong>the</strong> work of Dr<br />
Christophe Baudouin. 40 Having preservative-free opti<strong>on</strong>s<br />
available to patients in <strong>the</strong> United States is important. In my<br />
opini<strong>on</strong>, <strong>the</strong> future of drug delivery will lie in <strong>the</strong> preservativefree<br />
formulati<strong>on</strong>s, <strong>and</strong> <strong>the</strong> issue of OSD caused by ocular<br />
antihypertensives will become a moot point. In <strong>the</strong> future, we<br />
will look back <strong>and</strong> find it hard to believe that, for decades, we<br />
ophthalmologists applied BAK to our patients’ eyes.<br />
Dr Parrish: As anticipated, clinical evidence has dem<strong>on</strong>strated<br />
improvement of <strong>the</strong> ocular surface of patients when <strong>the</strong>y are<br />
* In additi<strong>on</strong>, preservative-free dorzolamide-timolol has recently been approved in <strong>the</strong> United States.<br />
7
switched <strong>from</strong> preserved ocular antihypertensives to<br />
preservative-free formulati<strong>on</strong>s. Janulevičienė <strong>and</strong> colleagues<br />
evaluated patients who were switched <strong>from</strong> BAK-preserved<br />
latanoprost to preservative-free tafluprost. In <strong>the</strong> study,<br />
patients who complained of ocular surface discomfort, who<br />
also had abnormal tear film break-up <strong>and</strong> abnormal corneal<br />
fluorescein staining with latanoprost with BAK, were switched<br />
to preservative-free tafluprost, resulting in significant<br />
improvements in <strong>the</strong>se subjective <strong>and</strong> objective measures. 37<br />
(Table) <str<strong>on</strong>g>The</str<strong>on</strong>g> o<strong>the</strong>r preservative-free ocular antihypertensive<br />
available in <strong>the</strong> United States is timolol, supplied in a sterile<br />
unit-dose dispenser. What is your experience with this<br />
preservative-free opti<strong>on</strong>?<br />
Dr Moster: I have a fair amount of patients <strong>on</strong> preservative-free<br />
timolol; <strong>the</strong>y are using <strong>the</strong> product twice daily as indicated. In<br />
my experience, preservative-free timolol is very well tolerated<br />
<strong>and</strong> is well suited for patients with dry eye who have been<br />
unable to tolerate preserved ocular antihypertensives, but who<br />
still require IOP-lowering <strong>the</strong>rapy following ALT or SLT.<br />
Dr Parrish: I have <strong>on</strong>ly a few patients <strong>on</strong> preservative-free<br />
timolol. In my experience, I have not found preservative-free<br />
timolol to make a l<strong>on</strong>g-term difference in <strong>the</strong> management of<br />
many of <strong>the</strong>se patients.<br />
Dr Pflugfelder: I have been impressed with patient outcomes<br />
when <strong>the</strong> ocular surface is no l<strong>on</strong>ger exposed to BAK. I<br />
prescribe preservative-free timolol for all my severe dry eye<br />
patients <strong>and</strong> for nearly every corneal transplant patient, <strong>and</strong><br />
c<strong>on</strong>sequently have hundreds of patients <strong>on</strong> this product.<br />
Indeed, before <strong>the</strong> availability of preservative-free tafluprost,<br />
preservative-free timolol was my go-to ocular antihypertensive<br />
for re-initiating topical <strong>the</strong>rapy following a drop holiday.<br />
Dr Parrish: If equally effective, comparably priced products were<br />
available, would you prescribe preservative-free ocular agents<br />
for your patients with glaucoma or ocular hypertensi<strong>on</strong>?<br />
Dr Pflugfelder: I certainly would choose a preservative-free<br />
ocular antihypertensive in patients at risk of ocular surface<br />
issues, in those with any corneal fluorescein staining, <strong>and</strong> in<br />
any o<strong>the</strong>r eye c<strong>on</strong>diti<strong>on</strong> in which ocular antihypertensives have<br />
been implicated in making <strong>the</strong> c<strong>on</strong>diti<strong>on</strong> worse, such as corneal<br />
transplantati<strong>on</strong> in a high-risk patient.<br />
Dr Hernd<strong>on</strong>: If efficacy is equivalent, prescribing preservativefree<br />
ocular antihypertensives for patients makes perfect sense.<br />
Dr Parrish: As an additi<strong>on</strong>al note, it is often thought that BAK<br />
allows greater penentrati<strong>on</strong> of <strong>the</strong> active ingredients through<br />
<strong>the</strong> cornea. If we compare bimatoprost, 0.3% with .05 mg/mL<br />
of BAK to bimatoprost, 0.01% with a 4-fold higher amount of<br />
BAK (0.2%) it may be that additi<strong>on</strong>al BAK was added to <strong>the</strong><br />
.01% soluti<strong>on</strong> for better penetrati<strong>on</strong>. 41 However, this is not<br />
known. It is important to keep in mind that <strong>the</strong> o<strong>the</strong>r<br />
prostagl<strong>and</strong>in analogs we just discussed, travoprost with SofZia<br />
<strong>and</strong> preservative-free tafluprost, achieve 25% to 30% pressure<br />
lowering, comparable to prostagl<strong>and</strong>in analogs with BAK.<br />
Surgical Strategies for C<strong>on</strong>trolling IOP <strong>and</strong><br />
Maintaining Ocular Surface Health<br />
Dr Parrish: According to <strong>the</strong> American Academy of<br />
Ophthalmology’s <strong>Glaucoma</strong> Preferred Practice Pattern ®<br />
Guidelines <strong>on</strong> Primary Open-Angle <strong>Glaucoma</strong>, medical <strong>the</strong>rapy,<br />
laser trabeculoplasty, <strong>and</strong> st<strong>and</strong>ard limbal filtrati<strong>on</strong> surgery are<br />
all viewed as acceptable modalities for <strong>the</strong> management of<br />
open-angle glaucoma. 42 In my practice, most patients prefer<br />
medical <strong>the</strong>rapy as <strong>the</strong> first-line approach to manage IOP.<br />
Generally, patients are not too eager to undergo surgery <strong>and</strong><br />
most patients are still c<strong>on</strong>cerned about laser procedures. Laser<br />
trabeculoplasty is a viable first-line <strong>the</strong>rapy, however, <strong>and</strong><br />
patients with poor ocular surface health or those who are<br />
experiencing intolerable adverse events <strong>from</strong> ocular<br />
antihypertensives occasi<strong>on</strong>ally opt for surgical management.<br />
Dr Hernd<strong>on</strong>: I offer laser trabeculoplasty as a first-line<br />
treatment for some of my glaucoma patients. I counsel <strong>the</strong><br />
patients regarding <strong>the</strong> efficacy, safety, <strong>and</strong> cost-effectiveness of<br />
laser opti<strong>on</strong>s, particularly SLT. Approximately 8 out of 10 of my<br />
patients choose SLT as <strong>the</strong> first-line <strong>the</strong>rapy; in most cases,<br />
after <strong>the</strong> procedure, medical <strong>the</strong>rapy use is postp<strong>on</strong>ed.<br />
Dr Moster: I discuss laser trabeculoplasty; however, most of my<br />
patients expect to begin with medical <strong>the</strong>rapy. <str<strong>on</strong>g>The</str<strong>on</strong>g>y will often<br />
c<strong>on</strong>sider laser as an opti<strong>on</strong> if ocular antihypertensives are<br />
causing symptoms or are not effectively c<strong>on</strong>trolling <strong>the</strong>ir IOP.<br />
Dr Hernd<strong>on</strong>: In patients with severe OSD, a trial of a preservativefree<br />
ocular antihypertensive is a reas<strong>on</strong>able <strong>the</strong>rapeutic approach<br />
to potentially delay or avoid surgical opti<strong>on</strong>s.<br />
Table. Patients’ Dry <strong>Eye</strong> Complaints, Mean Tear Film Break-up Time (± SD), <strong>and</strong> Abnormal Corneal Fluorescein Staining at<br />
Baseline (latanoprost with BAK), <strong>and</strong> at 2, 6, <strong>and</strong> 12 Weeks After Switching to Preservative-free Tafluprost 37<br />
Baseline Week 2 Week 6 Week 12<br />
P-value<br />
(12 weeks<br />
vs baseline)<br />
Dry eye complaints<br />
(n=30, patients)<br />
Tear film break-up time<br />
(sec<strong>on</strong>ds) (n=60, eyes)<br />
Abnormal fluorescein<br />
staining of <strong>the</strong> cornea<br />
(n=60, eyes)<br />
30 (100%) 19 (63.3%) 11 (36.7%) 11 (36.7%)
CASE VIGNETTES<br />
Vignette 1<br />
Dr Parrish: A 62-year-old white male is referred to <strong>the</strong><br />
ophthalmology clinic. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient does not have a family history<br />
of glaucoma. His IOP is 27 mm Hg. Examinati<strong>on</strong> shows an<br />
open angle, moderate pigmentati<strong>on</strong>, pseudoexfoliati<strong>on</strong> following<br />
dilati<strong>on</strong> of <strong>the</strong> pupil, <strong>and</strong> obvious disc <strong>and</strong> field change that fit<br />
with a diagnosis of early glaucoma with a paracentral scotoma.<br />
Which additi<strong>on</strong>al assessments would you c<strong>on</strong>duct, <strong>and</strong> what do<br />
you c<strong>on</strong>sider best practice management for this patient, taking<br />
into c<strong>on</strong>siderati<strong>on</strong> <strong>the</strong> potential intersecti<strong>on</strong> of glaucoma <strong>and</strong><br />
ocular surface health?<br />
Dr Moster: I would assess <strong>the</strong> patient’s visual field, nerve fiber<br />
layer, <strong>and</strong> Tmax IOP. Additi<strong>on</strong>ally, I would examine <strong>the</strong> patient’s<br />
ocular surface <strong>and</strong> anterior chamber, looking for signs of dry<br />
eye, such as superficial punctate epi<strong>the</strong>liopathy <strong>and</strong> abnormal<br />
tear break-up time. If <strong>the</strong> diagnosis is glaucoma with<br />
c<strong>on</strong>comitant ocular surface pathology, I would attempt to attain<br />
a 30% decrease in IOP with an ocular prostagl<strong>and</strong>in analog<br />
without BAK as a preservative.<br />
Dr Hernd<strong>on</strong>: I would determine <strong>the</strong> optimal IOP range for this<br />
patient after evaluating <strong>the</strong> visual field <strong>and</strong> nerve fiber layer<br />
studies. I would discuss treatment opti<strong>on</strong>s (medical, laser,<br />
surgical) with <strong>the</strong> patient, involving him in <strong>the</strong> decisi<strong>on</strong>. If he<br />
chose to pursue topical <strong>the</strong>rapeutic opti<strong>on</strong>s, I would recommend<br />
a prostagl<strong>and</strong>in analog without BAK as a preservative. SLT as a<br />
first-line opti<strong>on</strong> would be reas<strong>on</strong>able as well.<br />
Dr Parrish: Is Schirmer testing useful in this patient to evaluate<br />
<strong>the</strong> presence of OSD?<br />
Dr Pflugfelder: I believe that <strong>the</strong> Schirmer test is <strong>the</strong> least<br />
valuable of <strong>the</strong> ocular surface evaluati<strong>on</strong>s because of <strong>the</strong><br />
variable ways in which <strong>the</strong> test can be d<strong>on</strong>e <strong>and</strong> <strong>the</strong> limited<br />
amounted of informati<strong>on</strong> that <strong>the</strong> test provides.<br />
Dr Parrish: I would evaluate <strong>the</strong> health of <strong>the</strong> patient’s<br />
meibomian gl<strong>and</strong>s, assess <strong>the</strong> quality <strong>and</strong> quantity of meibum,<br />
<strong>and</strong> look for signs of vascularizati<strong>on</strong> or loss of lashes.<br />
Vignette 2<br />
Dr Parrish: A 70-year-old African American female returns to <strong>the</strong><br />
ophthalmology clinic 6 m<strong>on</strong>ths after starting generic latanoprost<br />
with BAK for a newly diagnosed case of glaucoma. Her IOP is<br />
well c<strong>on</strong>trolled; she is complaining, however, of ocular irritati<strong>on</strong><br />
<strong>and</strong> foreign body sensati<strong>on</strong>, <strong>and</strong> she is c<strong>on</strong>cerned about <strong>the</strong><br />
ocular redness she is experiencing. Ocular examinati<strong>on</strong> shows<br />
signs of OSD, including increased tear osmolarity <strong>and</strong> corneal<br />
fluorescein staining. What would you do?<br />
Dr Hernd<strong>on</strong>: I have had experience with similar cases. I would<br />
switch <strong>the</strong> patient’s <strong>the</strong>rapy to travoprost with SofZia. I am<br />
encouraged by <strong>the</strong> clinical evidence dem<strong>on</strong>strating <strong>the</strong><br />
tolerability <strong>and</strong> efficacy of preservative-free tafluprost, <strong>and</strong> so<br />
would c<strong>on</strong>sider prescribing that product for this patient.<br />
Dr Moster: I would also switch <strong>the</strong> patient’s <strong>the</strong>rapy to a BAKfree<br />
preparati<strong>on</strong> or to preservative-free tafluprost. Both patient<br />
adherence <strong>and</strong> <strong>the</strong> patient-clinician relati<strong>on</strong>ship improve when<br />
patients realize <strong>the</strong> clinician is making a change not <strong>on</strong>ly to<br />
effectively manage IOP, but also to enhance patient comfort.<br />
Dr Lewis: I would first investigate whe<strong>the</strong>r <strong>the</strong> irritati<strong>on</strong> is <strong>from</strong><br />
<strong>the</strong> active ingredient, <strong>from</strong> <strong>the</strong> latanoprost, or <strong>from</strong> <strong>the</strong><br />
preservatives in <strong>the</strong> formulati<strong>on</strong>. Perhaps <strong>the</strong> easiest way to<br />
determine that is to switch to a n<strong>on</strong>prostagl<strong>and</strong>in agent, such<br />
as timolol.<br />
CONCLUSION<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> deleterious effects caused by <strong>the</strong> preservative BAK in<br />
ocular antihypertensive agents can lead to poor ocular surface<br />
health in patients with glaucoma or ocular hypertensi<strong>on</strong>. 1-3 Poor<br />
ocular surface health, in turn, can negatively affect patient<br />
adherence to glaucoma <strong>the</strong>rapy 5,6 <strong>and</strong> thus adversely affect<br />
patient QOL. 7 It is <strong>the</strong>refore important for ophthalmologists to<br />
assess <strong>the</strong> glaucoma patient’s ocular surface: effectively,<br />
frequently, <strong>and</strong> efficiently. A drop holiday can be a safe <strong>and</strong><br />
effective strategy to reduce ocular surface distress without<br />
adversely affecting IOP management. Fortunately, ocular health<br />
researchers <strong>and</strong> clinicians have been working diligently to<br />
develop glaucoma <strong>the</strong>rapies that are both effective <strong>and</strong> gentler<br />
<strong>on</strong> <strong>the</strong> ocular surface. Presently, ocular antihypertensives<br />
without BAK—eg, travoprost with SofZia <strong>and</strong> brim<strong>on</strong>idine with<br />
Purite—<strong>and</strong> ocular antihypertensives without preservatives—<br />
am<strong>on</strong>g <strong>the</strong>m, preservative-free timolol, preservative-free<br />
dorzolamide-timolol, <strong>and</strong> preservative-free tafluprost—are<br />
safely <strong>and</strong> effectively c<strong>on</strong>trolling IOP. 20,29,30-32,37,38,43 In some<br />
patients, laser <strong>the</strong>rapy is an opti<strong>on</strong> for IOP c<strong>on</strong>trol. Today, eye<br />
care clinicians no l<strong>on</strong>ger need to accept deteriorati<strong>on</strong> of ocular<br />
surface health as <strong>the</strong> price to pay for <strong>the</strong> c<strong>on</strong>trol of IOP: it is<br />
encumbent up<strong>on</strong> <strong>the</strong>m to be proactive in <strong>the</strong> management of<br />
OSD in patients with glaucoma or ocular hypertensi<strong>on</strong>.<br />
9
REFERENCES<br />
1. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface<br />
disease in glaucoma patients. J <strong>Glaucoma</strong>. 2008;17(5):350-355.<br />
2. Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC,<br />
Jasek MC. Prevalence of ocular surface complaints in patients with<br />
glaucoma using topical intraocular pressure-lowering medicati<strong>on</strong>s.<br />
Cornea. 2010;29(6):618-621.<br />
3. Rossi GC, Tinelli C, Pasinetti GM, Milano G, Bianchi PE. Dry eye<br />
syndrome-related quality of life in glaucoma patients. Eur J<br />
Ophthalmol. 2009;19(4):572-579.<br />
4. Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry<br />
eye syndrome am<strong>on</strong>g US women. Am J Ophthalmol. 2003;136(2):<br />
318-326.<br />
5. Tsai JC, McClure CA, Ramos SE, Schlundt DG, Pichert JW.<br />
Compliance barriers in glaucoma: a systematic classificati<strong>on</strong>.<br />
J <strong>Glaucoma</strong>. 2003;12(5):393-398.<br />
6. Schwartz GF, Quigley HA. Adherence <strong>and</strong> persistence with glaucoma<br />
<strong>the</strong>rapy. Surv Ophthalmol. 2008;53 suppl 1:S57-S68.<br />
7. Schiffman RM, Walt JG, Jacobsen G, Doyle JJ, Lebovics G, Sumner W.<br />
Utility assessment am<strong>on</strong>g patients with dry eye disease.<br />
Ophthalmology. 2003;110(7):1412-1419.<br />
8. Erb C, Gast U, Schremmer D. German register for glaucoma patients<br />
with dry eye. I. Basic outcome with respect to dry eye. Graefes Arch<br />
Clin Exp Ophthalmol. 2008;246(11):1593-1601.<br />
9. Management <strong>and</strong> <strong>the</strong>rapy of dry eye disease: report of <strong>the</strong><br />
Management <strong>and</strong> <str<strong>on</strong>g>The</str<strong>on</strong>g>rapy Subcommittee of <strong>the</strong> Internati<strong>on</strong>al Dry<br />
<strong>Eye</strong> WorkShop (2007). Ocul Surf. 2007;5(2):163-178.<br />
10. Brasnu E, Brignole-Baudouin F, Riancho L, Guenoun JM, Warnet JM,<br />
Baudouin C. In vitro effects of preservative-free tafluprost <strong>and</strong><br />
preserved latanoprost, travoprost, <strong>and</strong> bimatoprost in a c<strong>on</strong>junctival<br />
epi<strong>the</strong>lial cell line. Curr <strong>Eye</strong> Res. 2008;33(4):303-312.<br />
11. Liang H, Pauly A, Riancho L, Baudouin C, Brignole-Baudouin F.<br />
Toxicological evaluati<strong>on</strong> of preservative-c<strong>on</strong>taining <strong>and</strong> preservativefree<br />
topical prostagl<strong>and</strong>in analogues <strong>on</strong> a three-dimensi<strong>on</strong>alrec<strong>on</strong>stituted<br />
corneal epi<strong>the</strong>lium system. Br J Ophthalmol.<br />
2011;95(6):869-875.<br />
12. Baudouin C, Riancho L, Warnet JM, Brignole F. In vitro studies of<br />
antiglaucomatous prostagl<strong>and</strong>in analogues: travoprost with <strong>and</strong><br />
without benzalk<strong>on</strong>ium chloride <strong>and</strong> preserved latanoprost. Invest<br />
Ophthalmol Vis Sci. 2007;48(9):4123-4128.<br />
13. Whits<strong>on</strong> JT, Cavanagh HD, Lakshman N, Petroll WM. Assessment of<br />
corneal epi<strong>the</strong>lial integrity after acute exposure to ocular<br />
hypotensive agents preserved with <strong>and</strong> without benzalk<strong>on</strong>ium<br />
chloride. Adv <str<strong>on</strong>g>The</str<strong>on</strong>g>r. 2006;23(5):663-671.<br />
14. Kahook MY, Noecker RJ. Comparis<strong>on</strong> of corneal <strong>and</strong> c<strong>on</strong>junctival<br />
changes after dosing of travoprost preserved with sofZia,<br />
latanoprost with 0.02% benzalk<strong>on</strong>ium chloride, <strong>and</strong> preservativefree<br />
artificial tears. Cornea. 2008;27(3):339-343.<br />
15. Denoyer A, Ossant F, Arbeille B, et al. Very-high-frequency ultrasound<br />
corneal imaging as a new tool for early diagnosis of ocular surface<br />
toxicity in rabbits treated with a preserved glaucoma drug.<br />
Ophthalmic Res. 2008;40(6):298-308.<br />
16. Br<strong>and</strong>t JD, Wittpenn JR, Katz LJ, Steinmann WN, Spaeth GL.<br />
C<strong>on</strong>junctival impressi<strong>on</strong> cytology in patients with glaucoma using l<strong>on</strong>gterm<br />
topical medicati<strong>on</strong>. Am J Ophthalmol. 1991;112(3):297-301.<br />
17. Zhang AQ, Liu H, Byrne C, Hutnik C. Mechanisms of benzalk<strong>on</strong>ium<br />
chloride toxicity in a human trabecular meshwork cell line. Poster<br />
presented at: 2012 Annual Meeting of <str<strong>on</strong>g>The</str<strong>on</strong>g> Associati<strong>on</strong> for<br />
Research in Visi<strong>on</strong> <strong>and</strong> Ophthalmology; May 6-10, 2012; Fort<br />
Lauderdale, FL.<br />
18. Ammar DA, Kahook MY. Effects of benzalk<strong>on</strong>ium chloride- or<br />
polyquad-preserved fixed combinati<strong>on</strong> glaucoma medicati<strong>on</strong>s <strong>on</strong><br />
human trabecular meshwork cells. Mol Vis. 2011;17:1806-1813.<br />
19. Noecker RJ, Herrygers LA, Anwaruddin R. Corneal <strong>and</strong> c<strong>on</strong>junctival<br />
changes caused by comm<strong>on</strong>ly used glaucoma medicati<strong>on</strong>s. Cornea.<br />
2004;23(5):490-496.<br />
20. Horsley MB, Kahook MY. Effects of prostagl<strong>and</strong>in analog <strong>the</strong>rapy <strong>on</strong><br />
<strong>the</strong> ocular surface of glaucoma patients. Clin Ophthalmol. 2009; 3:<br />
291-295.<br />
21. Sarkar J, Chaudhary S, Namavari A, et al. Corneal neurotoxicity due<br />
to topical benzalk<strong>on</strong>ium chloride. Invest Ophthalmol Vis Sci. 2012;<br />
53(4):1792-1802.<br />
22. Skalicky SE, Goldberg I, McCluskey P. Ocular surface disease <strong>and</strong><br />
quality of life in patients with glaucoma. Am J Ophthalmol. 2012;<br />
153(1):1-9.e2.<br />
23. Ammar DA, Kahook MY. Effects of glaucoma medicati<strong>on</strong>s <strong>and</strong><br />
preservatives <strong>on</strong> cultured human trabecular meshwork <strong>and</strong> n<strong>on</strong>pigmented<br />
ciliary epi<strong>the</strong>lial cell lines. Br J Ophthalmol.<br />
2011;95(10):1466-1469.<br />
24. Pflugfelder SC, Baudouin C. Challenges in <strong>the</strong> clinical measurement<br />
of ocular surface disease in glaucoma patients. Clin Ophthalmol.<br />
2011;5:1575-1583.<br />
25. Broadway DC, Griers<strong>on</strong> I, O'Brien C, Hitchings RA. Adverse effects of<br />
topical antiglaucoma medicati<strong>on</strong>. II. <str<strong>on</strong>g>The</str<strong>on</strong>g> outcome of filtrati<strong>on</strong><br />
surgery. Arch Ophthalmol. 1994;112(11):1446-1454.<br />
26. L<strong>and</strong>ers J, Martin K, Sarkies N, Bourne R, Wats<strong>on</strong> P. A twenty-year<br />
follow-up study of trabeculectomy: risk factors <strong>and</strong> outcomes.<br />
Ophthalmology. 2012;119(4):694-702.<br />
27. Price MO, Thomps<strong>on</strong> RW Jr, Price FW Jr. Risk factors for various<br />
causes of failure in initial corneal grafts. Arch Ophthalmol. 2003;<br />
121(8):1087-1092.<br />
28. Kahook MY, Ammar DA. In vitro toxicity of topical ocular<br />
prostagl<strong>and</strong>in analogs <strong>and</strong> preservatives <strong>on</strong> corneal epi<strong>the</strong>lial cells.<br />
J Ocul Pharmacol <str<strong>on</strong>g>The</str<strong>on</strong>g>r. 2010;26(3):259-263.<br />
29. Henry JC, Peace JH, Stewart JA, Stewart WC. Efficacy, safety, <strong>and</strong><br />
improved tolerability of travoprost BAK-free ophthalmic soluti<strong>on</strong><br />
compared with prior prostagl<strong>and</strong>in <strong>the</strong>rapy. Clin Ophthalmol.<br />
2008;2(3):613-621.<br />
30. Hamacher T, Airaksinen J, Saarela V, Liinamaa MJ, Richter U,<br />
Ropo A. Efficacy <strong>and</strong> safety levels of preserved <strong>and</strong> preservativefree<br />
tafluprost are equivalent in patients with glaucoma or ocular<br />
hypertensi<strong>on</strong>: results <strong>from</strong> a pharmacodynamics analysis. Acta<br />
Ophthalmol Suppl (Oxf). 2008;242:14-19.<br />
31. Chabi A, Varma R, Tsai JC, et al. R<strong>and</strong>omized clinical trial of <strong>the</strong><br />
efficacy <strong>and</strong> safety of preservative-free tafluprost <strong>and</strong> timolol in<br />
patients with open-angle glaucoma or ocular hypertensi<strong>on</strong>. Am J<br />
Ophthalmol. 2012;153(6):1187-1196.<br />
32. Katz LJ. Twelve-m<strong>on</strong>th evaluati<strong>on</strong> of brim<strong>on</strong>idine-purite versus<br />
brim<strong>on</strong>idine in patients with glaucoma or ocular hypertensi<strong>on</strong>.<br />
J <strong>Glaucoma</strong>. 2002;11(2):119-126.<br />
33. Schwartz GF, Kotak S, Mardekian J, Fain JM. Incidence of new<br />
coding for dry eye <strong>and</strong> ocular infecti<strong>on</strong> in open-angle glaucoma <strong>and</strong><br />
ocular hypertensi<strong>on</strong> patients treated with prostagl<strong>and</strong>in analogs:<br />
retrospective analysis of three medical/pharmacy claims<br />
databases. BMC Ophthalmol. 2011;11:14.<br />
34. Fain JM, Kotak S, Mardekian J, et al. A multicenter, retrospective<br />
chart review study comparing index <strong>the</strong>rapy change rates in openangle<br />
glaucoma or ocular hypertensi<strong>on</strong> patients newly treated with<br />
latanoprost or travoprost-Z m<strong>on</strong>o<strong>the</strong>rapy. BMC Ophthalmol. 2011;<br />
11(1):13.<br />
35. Lewis RA, Katz GJ, Weiss MJ, et al; Travoprost BAC-free Study Group.<br />
Travoprost 0.004% with <strong>and</strong> without benzalk<strong>on</strong>ium chloride: a<br />
comparis<strong>on</strong> of safety <strong>and</strong> efficacy. J <strong>Glaucoma</strong>. 2007;16(1):98-103.<br />
36. Mundorf T, Williams R, Whitcup S, Felix C, Batoosingh A. A 3-m<strong>on</strong>th<br />
comparis<strong>on</strong> of efficacy <strong>and</strong> safety of brim<strong>on</strong>idine-purite 0.15% <strong>and</strong><br />
brim<strong>on</strong>idine 0.2% in patients with glaucoma or ocular hypertensi<strong>on</strong>.<br />
J Ocul Pharmacol <str<strong>on</strong>g>The</str<strong>on</strong>g>r. 2003;19(1):37-44.<br />
37. Janulevičienė I, Derkač I, Grybauskiene L, Paulauskaitė R,<br />
Gromnickaite R, Kuzmienė L. Effects of preservative-free tafluprost<br />
<strong>on</strong> tear film osmolarity, tolerability, <strong>and</strong> intraocular pressure in<br />
previously treated patients with open-angle glaucoma. Clin<br />
Ophthalmol. 2012;6:103-109.<br />
38. Uusitalo H, Chen E, Pfeiffer N, et al. Switching <strong>from</strong> a preserved to a<br />
preservative-free prostagl<strong>and</strong>in preparati<strong>on</strong> in topical glaucoma<br />
medicati<strong>on</strong>. Acta Ophthalmol. 2010;88(3):329-336.<br />
39. Zioptan [package insert]. Whitehouse Stati<strong>on</strong>, NJ: Merck & Co, Inc;<br />
2012.<br />
40. R. Hitchings reported in Ophthalmology Times Europe October 1,<br />
2008. Accessed June 26, 2012.<br />
41. Lumigan [package insert]. Irvine, CA: Allergan, Inc; 2012.<br />
42. American Academy of Ophthalmology <strong>Glaucoma</strong> Panel. Preferred<br />
Practice Pattern ® Guidelines. Primary Open-Angle <strong>Glaucoma</strong>. San<br />
Francisco, CA: American Academy of Ophthalmology; 2010.<br />
www.aao.org/ppp. Accessed June 6, 2012.<br />
43. Shedden A, Adams<strong>on</strong>s IA, Gets<strong>on</strong> AJ, et al. Comparis<strong>on</strong> of <strong>the</strong><br />
efficacy <strong>and</strong> tolerability of preservative-free <strong>and</strong> preservativec<strong>on</strong>taining<br />
formulati<strong>on</strong>s of <strong>the</strong> dorzolamide/timolol fixed<br />
combinati<strong>on</strong> (COSOPT) in patients with elevated intraocular<br />
pressure in a r<strong>and</strong>omized clinical trial. Graefes Arch Clin Exp<br />
Ophthalmol. 2010;248(12):1757-1764.<br />
10
CME POST TEST<br />
How OSD Affects IOP<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> <str<strong>on</strong>g>Impact</str<strong>on</strong>g> <strong>on</strong> <strong>Glaucoma</strong> <strong>from</strong> <strong>the</strong> <strong>OUTSIDE</strong> <strong>IN</strong><br />
To obtain AMA PRA Category 1 Credit for this activity, you<br />
must complete <strong>the</strong> CME Post Test by writing <strong>the</strong> best answer to<br />
each questi<strong>on</strong> in <strong>the</strong> Answer Box located <strong>on</strong> <strong>the</strong> Activity<br />
Evaluati<strong>on</strong>/Credit Request form <strong>on</strong> <strong>the</strong> following page.<br />
To take this post test/evaluati<strong>on</strong> <strong>on</strong>line, please see<br />
"To Obtain AMA PRA Category 1 Credit" <strong>on</strong> page 2.<br />
1. In what percentage of patients with glaucoma or ocular<br />
hypertensi<strong>on</strong> treated with ocular antihypertensives are<br />
symptoms of ocular surface disease (OSD) present?<br />
a. 25<br />
b. 50<br />
c. 75<br />
d. 100<br />
2. Which of <strong>the</strong> following is directly correlated to <strong>the</strong> prevalence<br />
of OSD?<br />
a. Age 65 years or younger<br />
b. <str<strong>on</strong>g>The</str<strong>on</strong>g> number of years in which eyeglasses are worn<br />
c. <str<strong>on</strong>g>The</str<strong>on</strong>g> number of instilled ocular antihypertensive drops<br />
d. A humid climate<br />
3. Which of <strong>the</strong> following is/are a typical finding of OSD?<br />
a. Patient-reported ocular discomfort<br />
b. Redness of <strong>the</strong> eye<br />
c. Pathology of <strong>the</strong> corneal epi<strong>the</strong>lium<br />
d. All <strong>the</strong> above are typical findings of OSD<br />
4. A 67-year-old male patient presents to <strong>the</strong> ophthalmology clinic<br />
for a follow-up appointment for glaucoma management. <str<strong>on</strong>g>The</str<strong>on</strong>g><br />
patient has been treated with latanoprost with benzalk<strong>on</strong>ium<br />
chloride (BAK) for 1 year. He complains of eye irritati<strong>on</strong>, blurred<br />
<strong>and</strong> fluctuating visi<strong>on</strong>, <strong>and</strong> difficulty working <strong>on</strong> <strong>the</strong> computer for<br />
an extended period of time. He has been using preservativefree<br />
tear supplements for his symptoms. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient’s<br />
intraocular pressure (IOP) is 24 mm Hg (it was 16 mm Hg at<br />
<strong>the</strong> 6-m<strong>on</strong>th follow-up appointment). On examinati<strong>on</strong>, <strong>the</strong><br />
patient has c<strong>on</strong>junctival redness, superficial punctate keratitis,<br />
<strong>and</strong> poor corneal tear film. Which of <strong>the</strong> following is <strong>the</strong> most<br />
likely cause of <strong>the</strong> patient’s poorly c<strong>on</strong>trolled IOP?<br />
a. Patient tolerance to <strong>the</strong> pharmacological effects of<br />
latanoprost with BAK <strong>the</strong>rapy<br />
b. Worsening of glaucoma<br />
c. Drug interacti<strong>on</strong> with preservative-free tear<br />
supplements<br />
d. Suboptimal adherence to latanoprost with BAK <strong>the</strong>rapy<br />
5. Dry eye affects patient quality of life in a similar magnitude<br />
to that experienced in _____________.<br />
a. Unstable angina<br />
b. Diabetes mellitus<br />
c. Osteoporosis<br />
d. Hypertensi<strong>on</strong><br />
6. Which is NOT a deleterious effect of BAK?<br />
a. Disrupti<strong>on</strong> of tight juncti<strong>on</strong> proteins<br />
b. Programmed cell death, apoptosis, <strong>and</strong> necrosis in<br />
epi<strong>the</strong>lial cells<br />
c. IOP elevati<strong>on</strong><br />
d. Incitati<strong>on</strong> of cytokines, chemotactic factors, <strong>and</strong><br />
metalloproteinases<br />
7. A 68-year-old white female presents to <strong>the</strong> ophthalmology<br />
clinic with complaints of red, irritated eyes. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient is<br />
treated with latanoprost with BAK for IOP lowering. On<br />
examinati<strong>on</strong>, <strong>the</strong> patient has marked hyperemia of both<br />
eyes. Which of <strong>the</strong> following <strong>the</strong>rapeutic strategies would be<br />
most likely to completely eliminate <strong>the</strong> patient’s red eyes?<br />
a. Change <strong>the</strong>rapy to preservative-free tafluprost<br />
b. Add preservative-free dexamethas<strong>on</strong>e, 0.01%<br />
c. Change <strong>the</strong>rapy to travoprost with SofZia<br />
d. Initiate a drop holiday<br />
8. Which statement regarding n<strong>on</strong>-BAK preserved prostagl<strong>and</strong>in<br />
analog ocular antihypertensives is true?<br />
a. Preservative-free ocular antihypertensives are not as<br />
effective as BAK-preserved ocular antihypertensives in<br />
terms of lowering IOP<br />
b. Travoprost with SofZia has been found to be ineffective<br />
<strong>and</strong> not well tolerated<br />
c. Preservative-free ocular antihypertensives are more<br />
effective than BAK-preserved ocular antihypertensives<br />
in terms of lowering IOP.<br />
d. Preservative-free tafluprost has been found to have an<br />
IOP-lowering effect of up to 30%<br />
9. Which of <strong>the</strong> following treatment strategies is/are <strong>the</strong> most<br />
reas<strong>on</strong>able opti<strong>on</strong>(s) for addressing <strong>the</strong>rapeutic<br />
n<strong>on</strong>adherence due to ocular surface complaints in a patient<br />
currently <strong>on</strong> a prostagl<strong>and</strong>in analog with BAK?<br />
a. Laser trabeculoplasty<br />
b. Switch to a n<strong>on</strong>-BAK preserved or preservative-free<br />
ocular antihypertensive <strong>the</strong>rapy<br />
c. Add artificial tears to <strong>the</strong> current regimen<br />
d. A <strong>and</strong> B are <strong>the</strong> most reas<strong>on</strong>able opti<strong>on</strong>s<br />
10. A 73-year-old African American female patient presents to<br />
<strong>the</strong> ophthalmology clinic. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient has been <strong>on</strong> an IOPlowering<br />
regimen of brim<strong>on</strong>idine with Purite <strong>and</strong> latanoprost<br />
with BAK. She is complaining of ocular irritati<strong>on</strong> <strong>and</strong> foreign<br />
body sensati<strong>on</strong>. Ocular examinati<strong>on</strong> shows c<strong>on</strong>junctival<br />
redness, rapid tear film break-up, <strong>and</strong> corneal fluorescein<br />
staining. <str<strong>on</strong>g>The</str<strong>on</strong>g> patient’s IOP is 24 mm Hg <strong>and</strong> she reports<br />
being adherent to her ocular antihypertensive <strong>the</strong>rapy.<br />
Which of <strong>the</strong> following is likely <strong>the</strong> most appropriate<br />
<strong>the</strong>rapeutic strategy for this patient?<br />
a. Initiate a drop holiday <strong>and</strong> begin preservative-free<br />
dexamethas<strong>on</strong>e, 0.01%, followed by re-initiati<strong>on</strong> of<br />
ocular antihypertensive <strong>the</strong>rapy with a preservative-free<br />
formulati<strong>on</strong><br />
b. Initiate a drop holiday <strong>and</strong> begin IOP-lowering <strong>the</strong>rapy<br />
with an oral carb<strong>on</strong>ic anhydrase inhibitor, followed by<br />
re-initiati<strong>on</strong> of ocular antihypertensive <strong>the</strong>rapy with a<br />
preservative-free formulati<strong>on</strong><br />
c. Initiate a drop holiday <strong>and</strong> begin preservative-free<br />
dexamethas<strong>on</strong>e, 0.01%, followed by re-initiati<strong>on</strong> of<br />
ocular antihypertensive <strong>the</strong>rapy with brim<strong>on</strong>idine with<br />
Purite <strong>and</strong> travoprost with SofZia<br />
d. Initiate a drop holiday <strong>and</strong> begin preservative-free<br />
dexamethas<strong>on</strong>e, 0.01%; recommend laser<br />
trabeculoplasty within 1 week<br />
11
ACTIVITY EVALUATION/CREDIT REQUEST<br />
How OSD Affects IOP<br />
<str<strong>on</strong>g>The</str<strong>on</strong>g> <str<strong>on</strong>g>Impact</str<strong>on</strong>g> <strong>on</strong> <strong>Glaucoma</strong> <strong>from</strong> <strong>the</strong> <strong>OUTSIDE</strong> <strong>IN</strong><br />
Original Release: July 15, 2012<br />
Last Review: June 26, 2012<br />
Expirati<strong>on</strong>: July 30, 2013<br />
To receive AMA PRA Category 1 Credit, you must complete this Evaluati<strong>on</strong> form <strong>and</strong> <strong>the</strong> Post Test. Record your answers to <strong>the</strong> Post Test in <strong>the</strong> Answer Box<br />
located below. Mail or Fax this completed page to <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary–ICME, 310 East 14th Street, <strong>New</strong> <strong>York</strong>, NY 10003 (Fax: 212-353-5703).<br />
Your comments help us to determine <strong>the</strong> extent to which this educati<strong>on</strong>al activity has met its stated objectives, assess future educati<strong>on</strong>al needs, <strong>and</strong> create timely<br />
<strong>and</strong> pertinent future activities. Please provide all <strong>the</strong> requested informati<strong>on</strong> below. This ensures that your certificate is filled out correctly <strong>and</strong> is mailed to <strong>the</strong> proper<br />
address. It also enables us to c<strong>on</strong>tact you about future CME activities. Please print clearly or type. Illegible submissi<strong>on</strong>s cannot be processed.<br />
PARTICIPANT <strong>IN</strong>FORMATION (Please Print) ❏ Home ❏ Office<br />
Last Name _____________________________________________________________________ First Name ________________________________________<br />
Specialty ____________________________________________ Degree ❏ MD ❏ DO ❏ PharmD ❏ RPh ❏ NP ❏ RN ❏ PA ❏ O<strong>the</strong>r ____________<br />
Instituti<strong>on</strong> _________________________________________________________________________________________________________________________<br />
Street Address ____________________________________________________________________________________________________________________<br />
City ________________________________________ State _____________________ ZIP Code ____________________ Country ______________________<br />
Email ______________________________________ Ph<strong>on</strong>e ______________________________________ Fax _____________________________________<br />
Please note: We do not sell or share e-mail addresses. <str<strong>on</strong>g>The</str<strong>on</strong>g>y are used strictly for c<strong>on</strong>ducting post-activity follow-up surveys that are required by <strong>the</strong><br />
Accreditati<strong>on</strong> Council for C<strong>on</strong>tinuing Medical Educati<strong>on</strong> (ACCME).<br />
Learner Disclosure: To ensure compliance with <strong>the</strong> US Centers for Medicare <strong>and</strong> Medicaid Services regarding gifts to physicians, <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear<br />
Infirmary Institute for CME requires that you disclose whe<strong>the</strong>r or not you have any financial, referral <strong>and</strong>/or o<strong>the</strong>r relati<strong>on</strong>ship with our instituti<strong>on</strong>. CME certificates<br />
cannot be awarded unless you answer this questi<strong>on</strong>. For additi<strong>on</strong>al informati<strong>on</strong>, please call NYEE ICME at 212-979-4383. Thank you.<br />
❏ Yes ❏ No I <strong>and</strong>/or my family member have a financial relati<strong>on</strong>ship with <str<strong>on</strong>g>The</str<strong>on</strong>g> <strong>New</strong> <strong>York</strong> <strong>Eye</strong> <strong>and</strong> Ear Infirmary <strong>and</strong>/or refer Medicare/Medicaid patients to it.<br />
❏ I certify that I have participated in <strong>the</strong> entire activity <strong>and</strong> claim 1.5 AMA PRA Category 1 Credits.<br />
Signature Required __________________________________________________________________ Date Completed ______________________________<br />
OUTCOMES MEASUREMENT<br />
❏ Yes ❏ No Did you perceive any commercial bias in any part of this activity? IMPORTANT! If you answered “Yes,” we urge you to be specific<br />
about where <strong>the</strong> bias occurred so we can address <strong>the</strong> perceived bias with <strong>the</strong> c<strong>on</strong>tributor <strong>and</strong>/or in <strong>the</strong> subject matter in future activities.<br />
_________________________________________________________________________________________________________________________________<br />
Circle <strong>the</strong> number that best reflects your opini<strong>on</strong> <strong>on</strong> <strong>the</strong> degree to which <strong>the</strong> following learning objectives were met:<br />
5 = Str<strong>on</strong>gly Agree 4 = Agree 3 = Neutral 2 = Disagree 1 = Str<strong>on</strong>gly Disagree<br />
Up<strong>on</strong> completi<strong>on</strong> of this activity, I have improved my ability to:<br />
• State <strong>the</strong> prevalence of ocular surface disorders in patients with glaucoma or ocular hypertensi<strong>on</strong> 5 4 3 2 1<br />
• Describe <strong>the</strong> effects of preservatives in glaucoma medicati<strong>on</strong>s <strong>on</strong> <strong>the</strong> ocular surface 5 4 3 2 1<br />
• Identify <strong>the</strong>rapeutic approaches for patients with glaucoma or ocular hypertensi<strong>on</strong> that 5 4 3 2 1<br />
maintain or improve ocular surface health<br />
• Incorporate new strategies for improving <strong>the</strong>rapeutic adherence in patients with glaucoma or ocular hypertensi<strong>on</strong> 5 4 3 2 1<br />
PERSONAL OBJECTIVES<br />
1. Please list <strong>on</strong>e or more things, if any, you learned <strong>from</strong> participating in this educati<strong>on</strong>al activity that you did not already know. ____________________________<br />
_________________________________________________________________________________________________________________________________<br />
2. As a result of <strong>the</strong> knowledge gained in this educati<strong>on</strong>al activity, how likely are you to implement changes in your practice?<br />
4=definitely will implement changes 3=likely will implement changes 2=likely will not implement any changes 1=definitely will not make any changes<br />
5 4 3 2 1<br />
Please describe <strong>the</strong> change(s) you plan to make: __________________________________________________________________________________________<br />
_________________________________________________________________________________________________________________________________<br />
3. Related to what you learned in this activity, what barriers to implementing <strong>the</strong>se changes or achieving better patient outcomes do you face?<br />
_________________________________________________________________________________________________________________________________<br />
_________________________________________________________________________________________________________________________________<br />
4. Please check <strong>the</strong> Core Competencies (as defined by <strong>the</strong> Accreditati<strong>on</strong> Council for Graduate Medical Educati<strong>on</strong>) that were enhanced for you through participati<strong>on</strong><br />
in this activity. ❏ Patient Care ❏ Practice-Based Learning <strong>and</strong> Improvement ❏ Professi<strong>on</strong>alism<br />
❏ Medical Knowledge ❏ Interpers<strong>on</strong>al <strong>and</strong> Communicati<strong>on</strong> Skills ❏ Systems-Based Practice<br />
5. What o<strong>the</strong>r topics would you like to see covered in future CME programs? ___________________________________________________________________________<br />
_________________________________________________________________________________________________________________________________<br />
ADDITIONAL COMMENTS __________________________________________________________________________________________________________<br />
_________________________________________________________________________________________________________________________________<br />
POST TEST ANSWER BOX<br />
1 2 3 4 5 6 7 8 9 10