Clinical anatomy in the context of portal hypertension.
Clinical anatomy in the context of portal hypertension.
Clinical anatomy in the context of portal hypertension.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
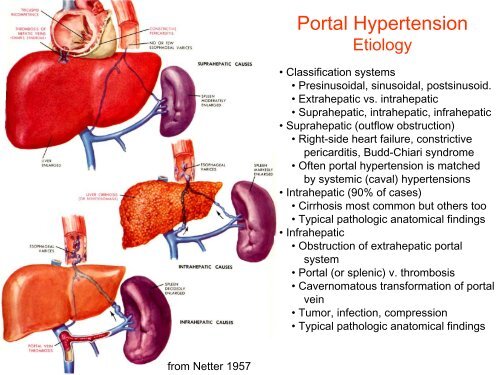
Portal Hypertension<br />
Etiology<br />
• Classification systems<br />
• Pres<strong>in</strong>usoidal, s<strong>in</strong>usoidal, posts<strong>in</strong>usoid.<br />
• Extrahepatic vs. <strong>in</strong>trahepatic<br />
• Suprahepatic, <strong>in</strong>trahepatic, <strong>in</strong>frahepatic<br />
• Suprahepatic (outflow obstruction)<br />
• Right-side heart failure, constrictive<br />
pericarditis, Budd-Chiari syndrome<br />
• Often <strong>portal</strong> <strong>hypertension</strong> is matched<br />
by systemic (caval) <strong>hypertension</strong>s<br />
• Intrahepatic (90% <strong>of</strong> cases)<br />
• Cirrhosis most common but o<strong>the</strong>rs too<br />
• Typical pathologic anatomical f<strong>in</strong>d<strong>in</strong>gs<br />
• Infrahepatic<br />
• Obstruction <strong>of</strong> extrahepatic <strong>portal</strong><br />
system<br />
• Portal (or splenic) v. thrombosis<br />
• Cavernomatous transformation <strong>of</strong> <strong>portal</strong><br />
ve<strong>in</strong><br />
• Tumor, <strong>in</strong>fection, compression<br />
• Typical pathologic anatomical f<strong>in</strong>d<strong>in</strong>gs<br />
from Netter 1957