

Radiopharmaceutical Therapy Dose Documentation Form
Radiopharmaceutical Therapy Dose Documentation Form
Radiopharmaceutical Therapy Dose Documentation Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
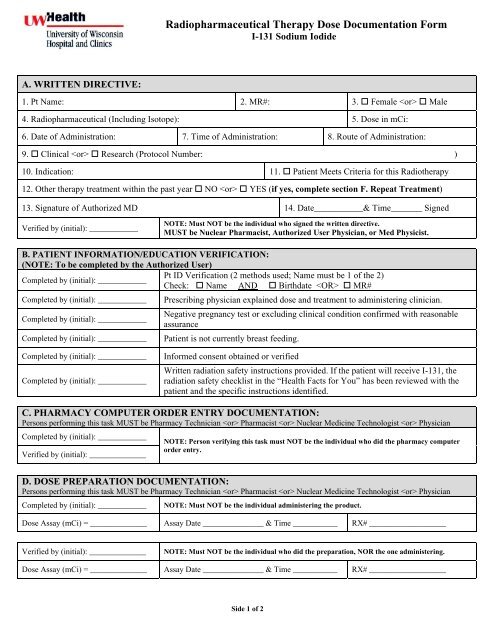
<strong>Radiopharmaceutical</strong> <strong>Therapy</strong> <strong>Dose</strong> <strong>Documentation</strong> <strong>Form</strong><br />
I-131 Sodium Iodide<br />
A. WRITTEN DIRECTIVE:<br />
1. Pt Name: 2. MR#: 3. Female Male<br />
4. <strong>Radiopharmaceutical</strong> (Including Isotope): 5. <strong>Dose</strong> in mCi:<br />
6. Date of Administration: 7. Time of Administration: 8. Route of Administration:<br />
9. Clinical Research (Protocol Number: )<br />
10. Indication: 11. Patient Meets Criteria for this Radiotherapy<br />
12. Other therapy treatment within the past year NO YES (if yes, complete section F. Repeat Treatment)<br />
13. Signature of Authorized MD 14. Date___________& Time_______ Signed<br />
Verified by (initial): ____________<br />
NOTE: Must NOT be the individual who signed the written directive.<br />
MUST be Nuclear Pharmacist, Authorized User Physician, or Med Physicist.<br />
B. PATIENT INFORMATION/EDUCATION VERIFICATION:<br />
(NOTE: To be completed by the Authorized User)<br />
Pt ID Verification (2 methods used; Name must be 1 of the 2)<br />
Completed by (initial): ____________<br />
Check: Name AND Birthdate MR#<br />
Completed by (initial): ____________<br />
Completed by (initial): ____________<br />
Completed by (initial): ____________<br />
Prescribing physician explained dose and treatment to administering clinician.<br />
Negative pregnancy test or excluding clinical condition confirmed with reasonable<br />
assurance<br />
Patient is not currently breast feeding.<br />
Completed by (initial): ____________<br />
Completed by (initial): ____________<br />
Informed consent obtained or verified<br />
Written radiation safety instructions provided. If the patient will receive I-131, the<br />
radiation safety checklist in the “Health Facts for You” has been reviewed with the<br />
patient and the specific instructions identified.<br />
C. PHARMACY COMPUTER ORDER ENTRY DOCUMENTATION:<br />
Persons performing this task MUST be Pharmacy Technician Pharmacist Nuclear Medicine Technologist Physician<br />
Completed by (initial): ____________<br />
Verified by (initial): ______________<br />
NOTE: Person verifying this task must NOT be the individual who did the pharmacy computer<br />
order entry.<br />
D. DOSE PREPARATION DOCUMENTATION:<br />
Persons performing this task MUST be Pharmacy Technician Pharmacist Nuclear Medicine Technologist Physician<br />
Completed by (initial): ____________<br />
NOTE: Must NOT be the individual administering the product.<br />
<strong>Dose</strong> Assay (mCi) = ______________ Assay Date _______________ & Time ___________ RX# ___________________<br />
Verified by (initial): ______________<br />
NOTE: Must NOT be the individual who did the preparation, NOR the one administering.<br />
<strong>Dose</strong> Assay (mCi) = ______________ Assay Date _______________ & Time ___________ RX# ___________________<br />
Side 1 of 2
E. I-131 THERAPY PATIENT RELEASE JUSTIFICATION RECORD for Exposure from the Patient<br />
RADIATION DOSE TO AN INDIVIDUAL EXPOSED TO PATIENT MUST BE < 500 mrem<br />
(Note: Complete either section 1, 2, 3, OR 4, as applicable.<br />
1. Patient with Thyroid (Assumes 100% whole body retention, dose MUST BE < 33 mCi for patient release):<br />
Estimated maximum dose to an individual exposed to patient.<br />
___________ mrem<br />
(15.15 x administered mCi) Using Appendix U, Table 14, WisReg 1556, Vol 9.<br />
2. Hyperthyroid Thyroid <strong>Therapy</strong> (Thyroid uptake < 40% or lower (E*), dose MUST BE < 56 mCi for patient release):<br />
* Assumes 0.125 Occupancy Factor (E), patient lives alone and few visits by family & friends for at least the first 2 days.<br />
Estimated maximum dose to an individual exposed to patient.<br />
___________ mrem<br />
(8.84 x administered mCi) Using Appendix U, Equation B-5, WisReg 1556, Vol 9.<br />
3. Patient Post-Thyroidectomy (dose MUST BE < 220 mCi for patient release):<br />
___________ mrem<br />
Estimated maximum dose to an individual exposed to patient.<br />
(2.27 x administered mCi) Using Appendix U, Equation B-5, WisReg 1556, Vol 9.<br />
4. Patient Specific Calculations (Calculations MUST BE APPROVED by Authorized Physician<br />
___________ mrem<br />
Estimated maximum dose to an individual exposed to patient. (Must be < 500 mrem for patient release)<br />
Using patient specific calculations, Using Appendix U, Equation B-5, WisReg 1556, Vol 9.<br />
(Attach spreadsheet used to aid in the calculation: J:/Nuclear/NuclearPharmacy/NRC & Safety & Dosimetry/I131<br />
Exposure/I-131 Thyroid Cancer Exposure Calculation.xls)<br />
F. Repeat Treatments (Refer to Section A. WRITTEN DIRECTIVE, Item No. 12)<br />
Is this repeat therapy<br />
treatment within a<br />
year?<br />
___________ mrem<br />
NO (SKIP this section, if NO is checked)<br />
YES (Estimated dose to an individual exposed to patient due to other treatment ____ mrem)<br />
TOTAL Estimated dose to an individual exposed to patient from other therapy treatments. (The sum of mrems<br />
from 1, 2, 3, or 4 to dose from other treatments within one year MUST be < 500 mrem for patient release)<br />
G. ADMINISTRATION VERIFICATION (NOTE: To be completed at the time of treatment)<br />
Persons performing this task MUST be Pharmacy Technician Pharmacist Nuclear Medicine Technologist Physician<br />
Authorized User Physician<br />
Clinician<br />
#1<br />
<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Initial<br />
_______<br />
Clinician<br />
#2<br />
<br />
Initial<br />
_______<br />
Clinician #1 is the Administering Clinician who is giving the dose.<br />
Clinician #2 is NOT administering the dose.<br />
Clinician #1 reads aloud the patient name, radiopharmaceutical and dose from the product label.<br />
Clinician #2 reviews the written directive and verifies that the following match (check as done):<br />
Patient Name <strong>Radiopharmaceutical</strong> <strong>Dose</strong><br />
Clinician #1 Clinician #2 assays the dose in the dose calibrator. NOTE: Must NOT be the individual<br />
who did the preparation, NOR the one who verified the product.<br />
<strong>Dose</strong> Assay (mCi) = ___________________ Date _________________ Time ______________<br />
(also document assay, time, date, initials on the computer generated prescription)<br />
Pt ID Verification (2 methods used; Name must be 1 of the 2) Check: Name AND Birthdate MR#<br />
Negative pregnancy test or excluding clinical condition confirmed with reasonable assurance.<br />
Patient is not currently breast feeding.<br />
<strong>Dose</strong> administered to patient.<br />
Patient released at the time of administration. YES NO<br />
Clinician #1 Signature ______________________________________ Date________________ Time___________________<br />
Side 2 of 2<br />
Initials on file in Nuclear Medicine Procedure Manual Version date 11/11/08; Updated 12/14/09














