Ascension® pyroCarbon Lunate
Ascension® pyroCarbon Lunate
Ascension® pyroCarbon Lunate

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
surgical<br />
technique<br />
Ascension Orthopedics does not recommend a particular<br />
surgical technique when using the implant. Proper surgical<br />
techniques are necessarily the responsibility of the medical<br />
profession. Each surgeon must evaluate the appropriateness<br />
of the surgical technique used based on personal medical<br />
training and experience. A description of the procedure<br />
used by Prof. John Stanley and Dr. Steven Moran follows.<br />
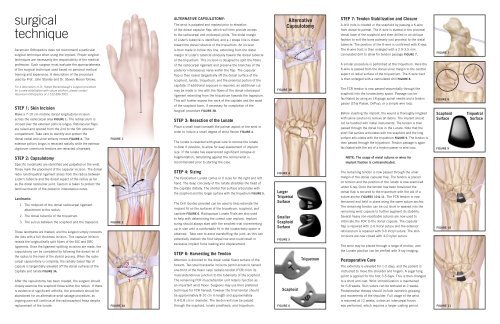
Alternative Capsulotomy:<br />
The wrist is palpated and marked prior to elevation<br />
of the dorsal capsular flap, which will then provide access<br />
to the radiocarpal and midcarpal joints. The distal margin<br />
of Lister’s tubercle is identified, and a J shape line is drawn<br />
toward the dorsal tubercle of the triquetrum. An incision<br />
is then made to follow this line, extending from the distal<br />
margin of Lister’s tubercle obliquely toward the dorsal tubercle<br />
of the triquetrum. This incision is designed to split the fibers<br />
of the radiocarpal ligament and preserve the branches of the<br />
posterior interosseous nerve within the flap. The capsular<br />
flap is then raised tangentially off the dorsal surface of the<br />
scaphoid, lunate, triquetrum, and the proximal portion of the<br />
Alternative<br />
Capsulotomy<br />
Step 7: Tendon Stabilization and Closure<br />
A drill hole is created in the scaphoid by passing a K-wire<br />
from dorsal to palmar. The K-wire is started in the proximal<br />
dorsal base of the scaphoid and then drilled in an oblique<br />
fashion to exit the bone palmarly just proximal to the distal<br />
tubercle. The position of the K-wire is confirmed with X-rays.<br />
The K-wire tract is then enlarged with a 2.9-3.5 mm<br />
cannulated drill to allow for tendon passage Figure 7.<br />
A similar procedure is performed at the triquetrum. Here the<br />
K-wire is passed from the dorsal ulnar margin to the central<br />
aspect of radial surface of the triquetrium. The K-wire tract<br />
is then enlarged with a cannulated drill Figure 8.<br />
Figure 7<br />
For a description of Dr. Robert Beckenbaugh's surgical procedure<br />
for <strong>Lunate</strong> stabilization with suture anchors, please contact<br />
Ascension Orthopedics at 1-512-836-5001.<br />
Step 1: Skin Incision<br />
Make a 7-10 cm midline dorsal longitudinal incision<br />
across the radiocarpal area Figure 1. The retinaculum is<br />
incised over the extensor pollicis longus. Retinacular flaps<br />
are raised and opened from the 2nd to the 5th extensor<br />
compartment. Take care to identify and protect the<br />
dorsal radial and ulnar sensory nerves Figure 2. The<br />
extensor pollicis longus is retracted radially while the extensor<br />
digitorum communis tendons are retracted ulnarward.<br />
Figure 1<br />
capitate. If additional exposure is required, an additional cut<br />
may be made in line with the fibers of the dorsal intercarpal<br />
ligament extending from the triquetrum towards the trapezium.<br />
This will further expose the neck of the capitate and the waist<br />
of the scaphoid bone, if necessary for completion of the<br />
surgical procedure Figure 3B.<br />
Step 3: Resection of the <strong>Lunate</strong><br />
Place a small towel beneath the palmar aspect of the wrist in<br />
order to induce a small degree of wrist flexion Figure 4.<br />
The lunate is resected with great care to remove the lunate<br />
in-total if possible, to allow for easy assessment of implant<br />
size. If the lunate has experienced significant collapse or<br />
Figure 3B<br />
The FCR tendon is now passed sequentially through the<br />
scaphoid into the lunatectomy space. Passage can be<br />
facilitated by using an 18 gauge spinal needle and a tendon<br />
passer (Chia Passer, DePuy), or a simple wire loop.<br />
Before inserting the implant, the wound is thoroughly irrigated<br />
with saline solution to remove all debris. The implant should<br />
not be handled with metal instruments. The tendon is then<br />
passed through the dorsal hole in the <strong>Lunate</strong>. Note that the<br />
short flat surface articulates with the scaphoid and the long<br />
surface articulates with the triquetrum Figure 9. The tendon is<br />
then passed through the triquetrum. Tendon passage is again<br />
facilitated with the aid of a tendon passer or wire loop.<br />
Figure 8<br />
Scaphoid<br />
Surface<br />
Figure 9<br />
Triquetral<br />
Surface<br />
Step 2: Capsulotomy<br />
Specific landmarks are identified and palpated on the wrist.<br />
These mark the placement of the capsular incision. The dorsal<br />
radio lunotriquetral ligament arises from the radius between<br />
Lister's tubercle and the dorsal aspect of the radius as far<br />
as the distal radioulnar joint. Caution is taken to protect the<br />
terminal branch of the posterior interosseous nerve.<br />
Landmarks:<br />
1. The midpoint of the dorsal radiocarpal ligament<br />
attachment to the radius.<br />
2. The dorsal tubercle of the triquetrum.<br />
3. The sulcus between the scaphoid and the trapezoid.<br />
These landmarks are marked, and the surgeon simply connects<br />
the dots with a full thickness incision. This capsular incision<br />
reveals the longitudinally split fibers of the DIC and DRC<br />
ligaments. Once the ligament-splitting incisions are made, the<br />
capsulotomy can be completed by following the dorsal rim of<br />
the radius to the level of the styloid process. When the radiocarpal<br />
capsulotomy is complete, the radially based flap of<br />
capsule is tangentially elevated off the dorsal surfaces of the<br />
capitate and lunate Figure 3A.<br />
After the capsulotomy has been created, the surgeon should<br />
closely examine the scaphoid fossa within the radius. If there<br />
is evidence of significant arthritis, the procedure should be<br />
abandoned for an alternative wrist salvage procedure, as<br />
ongoing pain will continue at the radioscaphoid fossa despite<br />
replacement of the lunate.<br />
Figure 2<br />
Figure 3A<br />
3<br />
1<br />
2<br />
fragmentation, templating against the normal wrist is<br />
recommended prior to starting the case.<br />
Step 4: Sizing<br />
The PyroCarbon <strong>Lunate</strong> comes in 5 sizes for the right and left<br />
hand. The deep concavity of the lunate straddles the head of<br />
the capitate distally. The shorter flat surface articulates with<br />
the scaphoid and the longer surface with the triquetrum Figure 5.<br />
The Drill Guides provided can be used to help estimate the<br />
implant fit on the surfaces of the triquetrum, scaphoid, and<br />
capitate Figure 6. Radiopaque <strong>Lunate</strong> Trials are also used<br />
to help with determining the correct size implant. Implant<br />
sizing should always start with the smallest trial incrementing<br />
up in size until a comfortable fit in the lunatectomy space is<br />
obtained. Take care to avoid overstuffing the joint, as this can<br />
potentially distract the first carpal row and could result in<br />
excessive implant force loading and displacement.<br />
Step 6: Harvesting the Tendon<br />
Attention is directed to the distal radial flexor surface of the<br />
forearm. Two small transverse incisions permit access to harvest<br />
one-third of the flexor carpi radialis tendon (FCR) from its<br />
musculotendinous junction to the tuberosity of the scaphoid.<br />
The remaining FCR muscle/tendon unit retains function as<br />
an important wrist flexor. Surgeons may use their preferred<br />
technique for FCR harvest; however the final tendon should<br />
be approximately 8-10 cm in length and approximately<br />
0.4-0.8 cm in diameter. The tendon will now be passed<br />
through the scaphoid, lunate prosthesis, and triquetrum.<br />
Figure 4<br />
Larger<br />
Triquetral<br />
Surface<br />
Smaller<br />
Scaphoid<br />
Surface<br />
Figure 5<br />
Scaphoid<br />
Figure 6<br />
Triquetrum<br />
NOTE: The usage of metal sutures or wires for<br />
implant fixation is contraindicated.<br />
The remaining tendon is now passed through the ulnar<br />
margin of the dorsal capsular flap. The tendon is placed<br />
on tension and the position of the lunate is now examined<br />
under X-ray. Once the tendon has been tensioned the<br />
dorsal flap is secured to the triquetrum with the aid of a<br />
suture anchor Figures 10 & 11. The FCR tendon is now<br />
tensioned and held in place using the same suture anchor.<br />
The remaining tendon can be cut short or weaved into the<br />
remaining wrist capsule to further augment its stability.<br />
Several heavy non-resorbable sutures are now used to<br />
imbricate the FCR to the dorsal capsule. The capsular<br />
flap is repaired with 2-0 Vicryl suture and the extensor<br />
retinaculum is repaired with 3-0 Vicryl suture. The skin<br />
incisions are now closed with 4-0 nylon suture.<br />
The wrist may be placed through a range of motion, and<br />
the <strong>Lunate</strong> position can be verified with X-ray imaging.<br />
Postoperative Care<br />
The extremity is elevated for 1-2 days, and the patient is<br />
instructed to move the shoulder and fingers. A sugar tong<br />
splint is applied for the first 3-5 days. This is then changed<br />
to a short arm cast. Wrist immobilization is maintained<br />
for 6-8 weeks. Skin suture can be removed at 2 weeks.<br />
Postoperative therapy should include isometric gripping<br />
and movements of the shoulder. Full usage of the wrist<br />
is resumed at 12 weeks, unless an intercarpal fusion<br />
was performed, which requires a longer casting period.<br />
Figure 10<br />
Figure 11
Cyclic<br />
Wear test<br />
Against<br />
Bone<br />
penetration rate<br />
(nanometer/cycle)<br />
0.2<br />
<strong>pyroCarbon</strong><br />
elastic<br />
Modulus<br />
(Gpa)<br />
23<br />
Cortical Bone<br />
4.3<br />
CoCr Alloy<br />
29.4<br />
<strong>pyroCarbon</strong><br />
30.4<br />
Titanium<br />
105<br />
Titanium<br />
34.7<br />
Zirconia<br />
Wear testing shows<br />
that PyroCarbon-on-bone<br />
articulation wear is<br />
significantly less than<br />
that of medical grade<br />
metals and ceramics.<br />
210<br />
Zirconia<br />
The elastic modulus<br />
of PyroCarbon closely<br />
matches that of cortical<br />
bone.<br />
design<br />
interpositional<br />
➤ maintains mobility<br />
➤ preserves the scaphoid<br />
and triquetrum<br />
➤ bone-friendly material<br />
➤ open pathway for revision<br />
system overview<br />
Design Description<br />
The Ascension ® PyroCarbon<br />
<strong>Lunate</strong> is an anatomically<br />
designed lunate replacement<br />
with essentially the same<br />
shape as the native lunate<br />
bone. The <strong>Lunate</strong> implant<br />
acts as an articulating<br />
spacer to maintain the relationship of adjacent carpal<br />
bones after excision and to maintain mobility of the wrist.<br />
The articular concavity that captures the capitate is more<br />
exaggerated to enhance stability. The <strong>Lunate</strong> implant has<br />
two holes which allow fixation of the implant by tendon or<br />
suture to the adjacent scaphoid and triquetrum bones to<br />
provide temporary postoperative stability while a capsular<br />
fibrosis system forms around the implant providing additional<br />
stability. The Ascension PyroCarbon <strong>Lunate</strong> is constructed<br />
of a high strength On-X ® PyroCarbon layer deposited on a<br />
graphite substrate. The graphite is impregnated with tungsten<br />
making the <strong>Lunate</strong> radiopaque. The implant is available in<br />
5 sizes for use in left or right applications.<br />
Indications<br />
Ascension ®<br />
At Ascension Orthopedics,<br />
we are dedicated to transforming<br />
the surgical experience.<br />
PyroCarbon <strong>Lunate</strong><br />
Implants<br />
Catalog number<br />
LUN-710-01<br />
LUN-710-02<br />
LUN-710-03<br />
LUN-710-04<br />
LUN-710-05<br />
Instrumentation<br />
Catalog number<br />
INS-710-00<br />
Set includes:<br />
Radiopaque Trials<br />
Sizing Guides<br />
Additional solutions<br />
for the hand:<br />
Ascension ®<br />
MCP/PIP<br />
PyroCarbon<br />
Total Joints<br />
Ascension ®<br />
MCP/PIP<br />
Pre-flexed<br />
Silicone Joints<br />
Ascension ®<br />
PyroCarbon<br />
CMC<br />
Arthroplasty<br />
First Choice ®<br />
DRUJ: Partial<br />
& Modular<br />
Ulnar Head<br />
description<br />
Size 01 <strong>Lunate</strong><br />
Size 02 <strong>Lunate</strong><br />
Size 03 <strong>Lunate</strong><br />
Size 04 <strong>Lunate</strong><br />
Size 05 <strong>Lunate</strong><br />
description<br />
Instrument Set<br />
Ascension ®<br />
PyroCarbon <strong>Lunate</strong><br />
tendon stabilization<br />
surgical technique<br />
Transforming Extremities <br />
Histological examination<br />
after 7 mos. of articulation<br />
with PyroCarbon PHS<br />
showed a layer of healthy<br />
fibrous pseudocartilage.<br />
Sample had no evidence<br />
of particulate synovitis. 2<br />
The PyroCarbon <strong>Lunate</strong> may be considered for use<br />
in the following situations:<br />
• Presence of avascular necrosis – Kienböck’s disease<br />
• Localized osteoarthritic changes of the radiolunate<br />
fossa or capitellar head<br />
• Long-standing lunate dislocations<br />
Contraindications<br />
• Acute or chronic infection<br />
• Radial scaphoid arthritis<br />
• Gross carpal instability<br />
Ascension Orthopedics, Inc.<br />
8700 Cameron Road<br />
Austin, Texas 78754<br />
512.836.5001 Ph<br />
877.370.5001 TFP<br />
512.836.6933 Fax<br />
888.508.8081 TFF<br />
customerservice@ascensionortho.com<br />
www.ascensionortho.com<br />
Caution: U.S. federal law restricts this device<br />
to sale by or on the order of a physician.<br />
LC-04-717-003 rev A<br />
©2009