Respiratory Examination
Respiratory Examination
Respiratory Examination

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Respiratory</strong> <strong>Examination</strong><br />
Dr. Andrew Don-Wauchope<br />
Lecturer in Clinical Medicine<br />
© University of Dublin, 2005
© University of Dublin, 2005
General Inspection<br />
appearance<br />
− dyspnea, cyanosis, cough, sputum, stridor,<br />
hoarseness<br />
respiratory rate (normal < 14)<br />
depth of respiration (shallow, deep)<br />
accessory muscles (SCM, platysma, strap<br />
muscles of neck)<br />
© University of Dublin, 2005
Looking at the Patient with COPD<br />
Rennard, S. I. N Engl J Med 2004;350:965-966<br />
© University of Dublin, 2005
Hands<br />
clubbing (lung CA, bronchiectasis, , lung<br />
abscess, CF, asbestosis, idiopathic pulmonary<br />
fibrosis)<br />
cyanosis<br />
nicotine staining<br />
wasting/weakness<br />
− wasting of small muscles of hand<br />
− weakness of finger abduction<br />
− due to lung CA compressing/infiltrating brachial<br />
plexus<br />
anemia (palmer creases)<br />
© University of Dublin, 2005
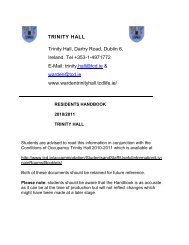
A 44-year-old man had had marked swelling of the terminal digits since early childhood<br />
Reynen, K. et al. N Engl J Med 2000;343:1235<br />
© University of Dublin, 2005
Hands<br />
clubbing (lung CA, bronchiectasis, , lung<br />
abscess, CF, asbestosis, idiopathic pulmonary<br />
fibrosis)<br />
cyanosis<br />
nicotine staining<br />
wasting/weakness<br />
− wasting of small muscles of hand<br />
− weakness of finger abduction<br />
− due to lung CA compressing/infiltrating brachial<br />
plexus<br />
anemia (palmer creases)<br />
© University of Dublin, 2005
© University of Dublin, 2005
Hands<br />
clubbing (lung CA, bronchiectasis, , lung<br />
abscess, CF, asbestosis, idiopathic pulmonary<br />
fibrosis)*<br />
cyanosis*<br />
nicotine staining<br />
wasting/weakness<br />
− wasting of small muscles of hand<br />
− weakness of finger abduction<br />
− due to lung CA compressing/infiltrating brachial<br />
plexus<br />
anemia (palmer creases)<br />
© University of Dublin, 2005
Hands contd.<br />
HPOA (swelling/tenderness at wrist)<br />
pulse<br />
− pulses paradoxus (severe asthma)<br />
− bounding (hypercapnia(<br />
hypercapnia)<br />
asterixis (hypercapnia) – flapping tremor<br />
dilated veins (hypercapnia(<br />
hypercapnia)<br />
© University of Dublin, 2005
Face<br />
eyes<br />
− anemia<br />
− Horner’s s Syndrome*<br />
nose*<br />
meiosis, ptosis, anhydrosis<br />
due to apical lung CA compressing sympathetic chain<br />
− polyps (asthma)<br />
− engorged turbinates (allergy)<br />
− deviated septum (obstruction)<br />
© University of Dublin, 2005
A 53-year-old man was evaluated because of a one-month history of anisocoria and left-sided<br />
ptosis of 1 mm (Panel A)<br />
Balcer, L. J. et al. N Engl J Med 1997;337:1359<br />
© University of Dublin, 2005
Face<br />
eyes<br />
− anemia<br />
− Horner’s s Syndrome*<br />
nose*<br />
meiosis, ptosis, anhydrosis<br />
due to apical lung CA compressing sympathetic chain<br />
− polyps (asthma)<br />
− engorged turbinates (allergy)<br />
− deviated septum (obstruction)<br />
© University of Dublin, 2005
Clinical Photograph of the Nose<br />
Weller, P. F. et al. N Engl J Med 2005;352:609-615<br />
© University of Dublin, 2005
Face<br />
eyes<br />
− anemia<br />
− Horner’s s Syndrome*<br />
nose*<br />
meiosis, ptosis, anhydrosis<br />
due to apical lung CA compressing sympathetic chain<br />
− polyps (asthma)<br />
− engorged turbinates (allergy)<br />
− deviated septum (obstruction)<br />
© University of Dublin, 2005
Face cont.<br />
mouth*<br />
− central cyanosis<br />
− pharynx (erythema(<br />
erythema, , purulent tonsils)<br />
− dentition (lung abscess, pneumonia)<br />
sinuses<br />
− tenderness (sinusitis)<br />
plethora<br />
− SVO<br />
− Pemberton’s s sign (arms raised over head causes<br />
plethora, stridor, , non-pulsatile<br />
elevation of JVP)<br />
© University of Dublin, 2005
Clinical Findings in Epstein-Barr Virus (EBV) Infection<br />
Cohen, J. I. N Engl J Med 2000;343:481-492<br />
© University of Dublin, 2005
© University of Dublin, 2005
Face cont.<br />
mouth*<br />
− central cyanosis<br />
− pharynx (erythema(<br />
erythema, , purulent tonsils)<br />
− dentition (lung abscess, pneumonia)<br />
sinuses<br />
− tenderness (sinusitis)<br />
plethora<br />
− SVO*<br />
− Pemberton’s s sign (arms raised over head causes<br />
plethora, stridor, , non-pulsatile<br />
elevation of JVP)*<br />
© University of Dublin, 2005
A 79-Year-Old Woman with Facial Swelling<br />
Betjes, M. G.H. N Engl J Med 2000;342:740<br />
© University of Dublin, 2005
Face cont.<br />
mouth*<br />
− central cyanosis<br />
− pharynx (erythema(<br />
erythema, , purulent tonsils)<br />
− dentition (lung abscess, pneumonia)<br />
sinuses<br />
− tenderness (sinusitis)<br />
plethora<br />
− SVO*<br />
− Pemberton’s s sign (arms raised over head causes<br />
plethora, stridor, , non-pulsatile<br />
elevation of JVP)*<br />
© University of Dublin, 2005
A 58-year-old woman with a 20-year history of goiter presented with a two-month history of<br />
progressive dyspnea on exertion, occasional stridor, and a choking sensation while supine<br />
Basaria, S. et al. N Engl J Med 2004;350:1338<br />
© University of Dublin, 2005
Neck<br />
lymph nodes*<br />
− submental, submandibular, , pre-auricular, post-<br />
auricular, occipital, cervical chain<br />
thyroid/goitre<br />
(airway obstruction)<br />
trachea<br />
− displacement (suggests disease of upper lobes)<br />
towards side of lesion<br />
• upper lobe collapse/fibrosis, pneumonectomy<br />
away from side of lesion<br />
• pleural effusion, tension pneumothorax<br />
upper mediastinal masses (retrosternal(<br />
goitre)<br />
© University of Dublin, 2005
© University of Dublin, 2005
© University of Dublin, 2005
Posteroanterior Film of the Chest Showing Left Inferior Hilar Lymphadenopathy (Arrow) and<br />
Right Paratracheal Lymphadenopathy (Arrowhead)<br />
Levitz, S. M. et al. N Engl J Med 1998;339:1835-1843<br />
© University of Dublin, 2005
Frontal Radiograph of the Chest Showing Bilateral Hilar Lymphadenopathy, Which Is More<br />
Prominent on the Left Side, and Mediastinal Lymphadenopathy<br />
Querfurth, H. W. et al. N Engl J Med 1998;338:747-754<br />
© University of Dublin, 2005
Neck<br />
lymph nodes*<br />
− submental, submandibular, , pre-auricular, post-<br />
auricular, occipital, cervical chain<br />
thyroid/goitre<br />
(airway obstruction)<br />
trachea<br />
− displacement (suggests disease of upper lobes)<br />
towards side of lesion<br />
• upper lobe collapse/fibrosis, pneumonectomy<br />
away from side of lesion<br />
• pleural effusion, tension pneumothorax<br />
upper mediastinal masses (retrosternal(<br />
goitre)<br />
© University of Dublin, 2005
Neck cont.<br />
−<br />
tug inferiorly with inspiration<br />
gross overexpansion of chest due to airflow<br />
obstruction<br />
© University of Dublin, 2005
Chest<br />
examine both anteriorly and posteriorly,<br />
comparing R and L*<br />
inspection<br />
− shape<br />
AP and lateral diameter<br />
• AP > lateral (barrel-shaped chest)<br />
• increased AP diameter due to hyperinflation (severe asthma,<br />
emphysema)<br />
pigeon chest/pectus carinatum<br />
• outward bowing of sternum<br />
• chronic childhood respiratory illness, rickets<br />
© University of Dublin, 2005
© University of Dublin, 2005
© University of Dublin, 2005
© University of Dublin, 2005
© University of Dublin, 2005
Chest<br />
examine both anteriorly and posteriorly,<br />
comparing R and L*<br />
inspection<br />
− Shape*<br />
AP and lateral diameter<br />
• AP > lateral (barrel-shaped chest)<br />
• increased AP diameter due to hyperinflation (severe asthma,<br />
emphysema)<br />
pigeon chest/pectus carinatum<br />
• outward bowing of sternum<br />
• chronic childhood respiratory illness, rickets<br />
© University of Dublin, 2005
An 18-year-old man with no clinically significant medical history presented with a six-month<br />
history of an increasing mass on the left side of his back (Panel A)<br />
Chaiyasate, K. et al. N Engl J Med 2005;352:e8<br />
© University of Dublin, 2005
A 13-year-old boy presented with increasing kyphotic deformity, back pain, and progressive<br />
paraparesis seven years after a one-year course of medical therapy for tuberculosis<br />
Shaw , B. A. N Engl J Med 1996;334:958-959<br />
© University of Dublin, 2005
© University of Dublin, 2005
Chest<br />
examine both anteriorly and posteriorly,<br />
comparing R and L*<br />
inspection<br />
− Shape*<br />
AP and lateral diameter<br />
• AP > lateral (barrel-shaped chest)<br />
• increased AP diameter due to hyperinflation (severe asthma,<br />
emphysema)<br />
pigeon chest/pectus<br />
carinatum<br />
• outward bowing of sternum<br />
• chronic childhood respiratory illness, rickets<br />
© University of Dublin, 2005
funnel chest/pectus<br />
excavatum<br />
• depression at lower sternum<br />
• developmental defect<br />
• may restrict lung capacity<br />
Harrison’s sulcus<br />
• linear depression of lower ribs along costal margin where<br />
diaphragm attached<br />
• severe childhood asthma, rickets<br />
kyphoscoliosis<br />
• decreases lung capacity, increases work of breathing<br />
• idiopathic (80%), poliomyelitis, Marfan’s<br />
© University of Dublin, 2005
− symmetry of chest wall movement<br />
reduced or delayed (underlying lung disease)<br />
• pulmonary fibrosis, consolidation, collapse, pleural effusion,<br />
pneumothorax<br />
bilateral reduction<br />
• chronic airflow limitation, diffuse pulmonary fibrosis<br />
− scars (previous thoracic surgery, chest drain)<br />
− erythema/thickened skin (previous RTx)<br />
© University of Dublin, 2005
palpation<br />
− chest expansion<br />
thumbs > 5cm apart with inspiration<br />
decreased on side of lesion<br />
− apex beat<br />
displacement toward side of lesion (lower lobe collapse,<br />
localized pulmonary fibrosis)<br />
displacement away from side of lesion (pleural effusion,<br />
tension pneumothorax)<br />
impalpable (emphysema)<br />
© University of Dublin, 2005
− vocal fremitus (99)<br />
increased vibration (consolidation)<br />
no vibration (fluid)<br />
unreliable sign<br />
− ribs (pain, fracture)<br />
− subcutaneous emphysema*<br />
crackling on palpation of skin<br />
air tracking from pneumothorax, , ruptured esophagus<br />
© University of Dublin, 2005
A 76-year-old man with chronic obstructive pulmonary disease was admitted after a car accident<br />
van der Kleij, F. G.H. et al. N Engl J Med 2000;342:1333<br />
© University of Dublin, 2005
− vocal fremitus (99)<br />
increased vibration (consolidation)<br />
no vibration (fluid)<br />
unreliable sign<br />
− ribs (pain, fracture)<br />
− subcutaneous emphysema*<br />
crackling on palpation of skin<br />
air tracking from pneumothorax, , ruptured esophagus<br />
© University of Dublin, 2005
percussion<br />
− anteriorly, posteriorly, supraclavicular fossa<br />
− resonant (normal)<br />
− hyper-resonant (bowel, pneumothorax)<br />
− dull (consolidation)<br />
− stony dull (fluid)<br />
© University of Dublin, 2005
auscultation<br />
− quality of breath sounds<br />
vesicular (normal)<br />
• transmission of air turbulence in large airways filtered through<br />
normal lung to chest wall<br />
• sound of “wind rustling in leaves”<br />
• louder and longer on inspiration than expiration<br />
• no gap<br />
bronchial<br />
• turbulence in large airways is heard without being filtered by<br />
alveoli<br />
• hollow, blowing quality (cf. stethoscope over trachea)<br />
• inspiration = expiration, gap<br />
• consolidation, pulmonary fibrosis, above pleural effusion,<br />
collapsed lung<br />
© University of Dublin, 2005
− intensity of breath sounds<br />
normal<br />
reduced (COPD, pleural effusion, pneumothorax, tumour,<br />
collapse, consolidation)<br />
− added sounds<br />
wheeze<br />
• inspiration/expiration (louder due to narrower airway)<br />
• pitch (high – small bronchi, low – larger bronchi)<br />
crackles<br />
• early inspiration (disease of small airways)<br />
• late or pan-inspiration (disease confined to alveoli)<br />
<br />
<br />
<br />
fine (pulmonary fibrosis)<br />
medium (LVF)<br />
coarse (pools of retained secretion – bronchiectasis)<br />
© University of Dublin, 2005
pleural friction rub<br />
• pleurisy (inflammation of pleura)<br />
• PE, pneumonia<br />
− vocal resonance (99)<br />
muffled (normal)<br />
clearly audible (consolidation)<br />
no sound (fluid)<br />
© University of Dublin, 2005
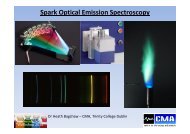
Soon after returning from Hong Kong, a previously healthy 48-year-old man began to have fever,<br />
malaise, dyspnea, and a nonproductive cough<br />
Nicolaou, S. et al. N Engl J Med 2003;348:2006<br />
© University of Dublin, 2005
Heart<br />
raised JVP, peripheral edema<br />
− cor pulmonale (RVF due to COPD, pulmonary<br />
fibrosis, PE, obesity, sleep apnea, kyphoscoliosis)<br />
loud P2 (pulmonary hypertension)<br />
© University of Dublin, 2005
Abdomen<br />
liver ptosis (emphysema)<br />
hepatomegaly due to metastases from lung CA<br />
© University of Dublin, 2005
Legs<br />
DVT as cause of PE<br />
© University of Dublin, 2005
A 67-year-old man presented to the emergency department with a five-day history of<br />
nonproductive cough and progressive dyspnea and a one-day history of right-sided pleuritic<br />
chest pain<br />
Sokolove, P. E. et al. N Engl J Med 2001;345:1311<br />
© University of Dublin, 2005
A 47-year-old man was admitted to the intensive care unit with respiratory failure complicating<br />
pneumonia due to legionella infection<br />
van Steijn, J. H.M. et al. N Engl J Med 2004;350:e16<br />
© University of Dublin, 2005