4. Clinical Guidelines for Liver Transplantation (PDF) - British ...
4. Clinical Guidelines for Liver Transplantation (PDF) - British ...
4. Clinical Guidelines for Liver Transplantation (PDF) - British ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
______________________________<br />
4 <strong>Clinical</strong><br />
<strong>Guidelines</strong><br />
For <strong>Liver</strong><br />
<strong>Transplantation</strong><br />
Program<br />
______________________________<br />
REVISED July, 2010<br />
The <strong>Clinical</strong> <strong>Guidelines</strong> are a statement of consensus of BC Transplant professionals regarding their views of currently<br />
accepted approaches to treatment. Any clinician seeking to apply or consult the <strong>Guidelines</strong> is expected to use<br />
independent medical judgment in the context of individual clinical circumstances to determine any patient's care or<br />
treatment. Use of these guidelines and any in<strong>for</strong>mation on it is at your own risk, and is subject to our Terms of Use.<br />
AMB-GEN.08.005 Rev 01
<strong>4.</strong>1.1 INTRODUCTION<br />
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1 Transplant<br />
<strong>Clinical</strong> liver transplantation was first per<strong>for</strong>med in 1963 by Thomas Starzl and is now an<br />
established therapy <strong>for</strong> end-stage liver disease in selected patients. Since the introduction of<br />
Cyclosporine by Sir Roy Calne in 1978, outcomes have improved significantly so that the oneyear<br />
survival is approximately 80 to 90%. Most people return to a normally functioning life,<br />
although lifelong monitoring and immunosuppressive therapy is required. <strong>Liver</strong> transplantation<br />
was first per<strong>for</strong>med in <strong>British</strong> Columbia in 1989. At present, about 30 to 40 adults undergo<br />
liver transplantation annually in B.C.<br />
<strong>4.</strong>1.2 INDICATIONS AND REFERRAL GUIDELINES<br />
<strong>Liver</strong> transplantation should be considered <strong>for</strong> patients with decompensated chronic liver<br />
disease <strong>for</strong> which all other therapeutic options have been exhausted. Such patients generally<br />
have one or more of the following:<br />
<br />
<br />
<br />
<br />
<br />
<br />
Jaundice<br />
Decreased synthetic function (decreased albumin, increased INR)<br />
Encephalopathy<br />
Ascites<br />
Variceal bleeding<br />
Hepatocellular carcinoma (selected)<br />
Such patients will have an anticipated survival of less than three or four years due to liverrelated<br />
complications without liver replacement. <strong>Transplantation</strong> is also appropriate therapy <strong>for</strong><br />
some patients with fulminant acute liver failure.<br />
Special Considerations:<br />
Hepatitis C: Hepatitis C has become the most common indication <strong>for</strong> liver transplantation in<br />
most programs in North America. While results are fairly good, there is a high risk of recurrent<br />
hepatitis C in the new liver. The recurrence disease may be mild, but often leads to significant<br />
scarring in the liver after 5 years and many patients will have progressed to cirrhosis after 10<br />
years post-transplant. In about 10% of cases, the recurrent disease is rapidly progressive and<br />
may lead to graft failure within the first few years. Un<strong>for</strong>tunately there are few treatment<br />
options in this circumstance and the results of retransplantation <strong>for</strong> early graft loss from<br />
recurrent hepatitis C are too poor to make this a viable option. Antiviral therapy with Interferon<br />
and Ribavirin is offered to selected patients with recurrent hepatitis C, but the effectiveness in<br />
preventing graft failure is unknown and there is a theoretical risk that Interferon may trigger<br />
rejection.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 1<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.2 INDICATIONS AND REFERRAL GUIDELINES CONT.<br />
Hepatitis B: With the advent of effective strategies <strong>for</strong> preventing allograft reinfection with<br />
hepatitis B, patients with hepatitis B can now be considered <strong>for</strong> liver transplantation. The HBV<br />
DNA level must be at the lowest level possible in order to meet transplant criteria. Those who<br />
have high HBV-DNA levels will be treated with Lamivudine at 100 mg daily. This results in<br />
HBV-DNA becoming undetectable after approximately four to six weeks in about 90% of such<br />
patients. Patients who do not respond may be treated with Adefovir, Tenofovir or Entecavir.<br />
Those who remain HBV-DNA at a titer greater than 500,000 copies/mL cannot be activated <strong>for</strong><br />
transplantation. Patients with HBV who are identified, as possible transplant recipients should<br />
only be started on Lamivudine or Adefovir, after discussion with the transplant team. Although<br />
Lamivudine is well tolerated, there is a high rate of resistance by the development of mutant<br />
hepatitis B virus. This is approximately 50% per year <strong>for</strong> the first three years and the emergence<br />
of a mutant virus will render the patient HBV-DNA positive and makes transplantation more<br />
problematic as high-dose HBIG is then required to reduce the risk of allograft reinfection. Even<br />
HBV-DNA negative patients with hepatitis B are at risk of allograft reinfection. Fortunately,<br />
this can be prevented using a combination of antiviral drugs and immunoprophylaxis. We are<br />
currently using long-term prophylaxis with Lamivudine combined with low dose hepatitis B<br />
immune globulin (HBIG). Although patients can also develop HBV escape mutants that are<br />
resistant to the HBIG, at present the combination of Lamivudine and immune globulin appears<br />
to be very effective at preventing HBV recurrence.<br />
Alcoholic <strong>Liver</strong> Disease: Patients with liver failure due to or associated with alcohol abuse<br />
can be considered <strong>for</strong> transplantation provided that they have demonstrated full and sustained<br />
rehabilitation from alcohol and other substance abuse and that social supports and an abstinence<br />
maintenance program are in effect. The minimal criteria are at least 6 months verifiable<br />
abstinence, willingness to sign abstinence and monitoring contract, a satisfactory report from an<br />
independent alcohol and drug counsellor and favourable assessments from the transplant<br />
program staff members who have expertise in evaluation of patients with a history of substance<br />
abuse.<br />
Metabolic Diseases: <strong>Liver</strong> transplantation is occasionally offered as therapy <strong>for</strong> patients<br />
with genetic disorders that can be corrected by liver transplantation. Examples include familial<br />
amyloidosis, or metabolic conditions such as oxaluria, glycogen storage disease and urea cycle<br />
defects.<br />
Hepatocellular Carcinoma: Patients with hepatocellular carcinoma can be considered <strong>for</strong><br />
liver transplantation. However, they must be carefully selected to minimize the chance of<br />
recurrence of metastatic disease, because the progression of hepatoma is accelerated by<br />
immunosuppression. Patients with one lesion at 5 cm or up to 3 lesions, none greater than 3 cm.<br />
Patients with solitary tumors up to 6 cm could be considered if they showed a good response to<br />
pretransplant cytoreduction. All patients with single tumor should be offered pretransplant<br />
cytoreductive therapy. Smaller tumors will be treated with RFA or alcohol ablation and large<br />
ones with chemoembolization or combination therapy. Patients who have larger lesions are<br />
occasionally considered if they have a good response to chemoembolization. A “good response”<br />
is shrinkage of the tumour, with a needle biopsy of the area that is negative and a significant<br />
improvement in the alpha-fetoprotein. Chemoembolization is rarely used in patients who have a<br />
portal vein thrombosis or a previous shunt procedure.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 2<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.2 INDICATIONS AND REFERRAL GUIDELINES CONT.<br />
HIV <strong>Guidelines</strong>:<br />
Undectable HIV viral load.<br />
CD4 count ≥ 200 but in individual cases, may consider < 200.<br />
HAART medications on wait list (no minimum duration, HAART medications may be<br />
changed by HIV specialist at anytime, i.e. no specific duration “stable dose” required).<br />
Each case will be assessed on an individual basis. HIV guidelines are recognized to be on<br />
going, dynamic in nature and they are subject to change based on future research outcomes. The<br />
<strong>Liver</strong> Transplant Program has an on-going dialogue with the HIV Centre <strong>for</strong> Excellence on<br />
these issues.<br />
Age: Although there is no absolute age limitation, post-operative complications are more<br />
common in patients over 60 and long-term outcomes are often disappointing. Candidates older<br />
than 60 are screened carefully <strong>for</strong> concomitant disease and many will not be suitable <strong>for</strong><br />
transplantation due to comorbid conditions.<br />
General Health: Although secondary organ dysfunction may be present, it is not necessarily a<br />
contraindication if it can be expected to improve after transplantation.<br />
Compliance: Patients must be capable of following a complex medical regimen. Those with a<br />
history of noncompliance cannot be accepted.<br />
Emotional Stability and Motivation: Patients should be emotionally stable, have realistic<br />
attitudes towards their illness and have a strong will to live and return to productive lives.<br />
Support: Transplant candidates must identify a person or persons (usually a spouse or family<br />
member) who can provide comprehensive support be<strong>for</strong>e and after transplantation. The<br />
demands on support persons can be high and some patients may be unable to identify an<br />
individual who is able to meet the program’s requirement in that respect. Un<strong>for</strong>tunately, in such<br />
cases the program must defer activation <strong>for</strong> transplantation.<br />
Financial Resources: Patients should be prepared to stay in the Vancouver area <strong>for</strong> several<br />
months. Social services may be helpful in identifying sources of support.<br />
Expectations: Patients should have an understanding of what is involved in transplantation<br />
and should realize that they will be assessed by numerous members of the transplant team to<br />
determine if transplantation is a feasible treatment option. The decision on the appropriateness<br />
of transplantation is not made until after the assessment is completed.<br />
Physician Support: After consultation, patients are returned to the care of their referring<br />
specialist and family physician. The referring physician should be prepared to assist in<br />
arranging investigations required <strong>for</strong> the transplant assessment. Throughout the assessment<br />
process, the <strong>Clinical</strong> Coordinator will communicate with the referring physician, the patient and<br />
the transplant physicians regarding the assessment process and the patient’s clinical condition.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 3<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.2 INDICATIONS AND REFERRAL GUIDELINES CONT.<br />
After transplantation, patients will be seen by the transplant team through the Transplant<br />
Outpatient Clinic but are also expected to be followed by the referring physician and the family<br />
practitioner. The role of the transplant team is limited to monitoring graft function, prescribing<br />
immunosuppression and assisting with management of transplant-related complications. The<br />
family physician should be prepared to provide non-transplant care.<br />
Contraindications: The following are generally considered to be contraindications to liver<br />
transplantation:<br />
<br />
<br />
<br />
<br />
<br />
<br />
Active or chronic infection outside the biliary tree<br />
Extensive malignancy<br />
Systemic disease which significantly limits life expectancy or quality<br />
Refusal to accept blood transfusions or blood products<br />
Ongoing or recurrent alcohol or substance abuse<br />
Inability to follow a complex medical regimen<br />
Patients may be referred directly to the <strong>Clinical</strong> <strong>Liver</strong> Coordinator at BC Transplant (604-877-<br />
2240 or 1-800-663-6189).<br />
(See Appendix A: <strong>Liver</strong> Transplant Referral <strong>for</strong>m)<br />
<strong>4.</strong>1.3 ASSESSMENT<br />
Patients are usually seen on an outpatient basis at BC Transplant unless they are too ill and need<br />
to be hospitalized. Critically ill patients may be transferred to Vancouver General Hospital <strong>for</strong><br />
assessment. Following assessment, they are transferred back to their referring physician<br />
whenever possible <strong>for</strong> ongoing management. Patients should be referred when they are still<br />
relatively stable to minimize the likelihood of death or complications that preclude<br />
transplantation be<strong>for</strong>e the evaluation is completed or a suitable donor organ can be obtained.<br />
At the time of the initial assessment, patients will be seen by the <strong>Clinical</strong> Coordinator, a<br />
Transplant Hepatologist and Surgeon. All referred patients will be discussed at a weekly<br />
meeting of the liver transplant team. At that time, a recommendation will be made about the<br />
most appropriate management of the patient’s liver disease. Patients deemed to require<br />
transplantation will then have further investigations, including a CT scan of the abdomen. They<br />
will be seen by an Anaesthetist and by the team’s Psychologist, Social Worker and Dietician. In<br />
some cases, consultation with other specialists may also be sought. During the assessment<br />
phase, the transplant team provides patients and families with in<strong>for</strong>mation about transplantation,<br />
including the risks and benefits of the procedure, medication regimens and the transplant<br />
process.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 4<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.3 ASSESSMENT CONT.<br />
Routine Investigations<br />
The following tests are typically done during the assessment phase:<br />
Complete blood count<br />
INR<br />
PTT<br />
Electrolytes<br />
Creatinine<br />
<strong>Liver</strong> function tests<br />
Glucose<br />
Protein<br />
Alpha fetoprotein<br />
CEA<br />
Urinalysis<br />
PSA to male patient<br />
Stool <strong>for</strong> occult blood<br />
TB skin test<br />
Virology markers <strong>for</strong> Hepatitis B, Hepatitis C, CMV, EBV, Hepatitis A, HSV, VSV,<br />
and HIV<br />
(Where indicated), ferritin, TIBC, Iron, Fraction Saturation, (ceruloplasmin, alphato1<br />
antitrypsin), ANA and antimitochondrial antibody and antismooth<br />
Blood group<br />
ECG<br />
Echocardiogram<br />
Chest X-Ray<br />
Ultrasound (Doppler)<br />
CT scan / MRI<br />
Mammogram (women)<br />
Selected patients may require gastroscopy, ERCP, colonoscopy<br />
Dental Examination<br />
Anaesthetic consult<br />
<strong>4.</strong>1.4 ACTIVATION<br />
Patients referred <strong>for</strong> liver transplant are assessed and, if necessary, appropriate consultation is<br />
made with specialists in the areas of Medicine, Surgery, Social Work, Psychiatry/Psychology<br />
and Drug and Alcohol Addiction. All candidates <strong>for</strong> liver transplantation who have been<br />
referred are then discussed at the weekly liver transplant activation rounds. This is a<br />
multidisciplinary rounds including representation from transplant hepatology, surgery, nursing,<br />
nutrition, pharmacy, psychology and social work. The decision to place a patient on the waiting<br />
list is made in accordance with current accepted Canadian <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong>.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 5<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.4 ACTIVATION CONT.<br />
Indication <strong>for</strong> liver transplantation shall be documented in the physician and surgeon consult<br />
notes and in the coordinator’s progress notes. Patients are supplied with educational material<br />
including Living with <strong>Liver</strong> Transplant Manual which includes risk factors relevant to<br />
successful transplantation.<br />
The date of activation is documented on the Recipients Activation Sheet and on the active list.<br />
Patients accepted <strong>for</strong> transplantation will be placed on the active list and will be given a pager<br />
and instructions to communicate any change in their location or health status to the transplant<br />
coordinator. A letter is also sent to the referring physicians by the coordinator. While on the<br />
active list, they will be followed closely by the transplant team. Patients living outside the<br />
Lower Mainland have urgent transportation to Vancouver arranged by the transplant<br />
coordinator when a donor organ is available. Air Ambulance costs are not covered by Medical<br />
Services Plan, however, they may be covered by extended health benefits.<br />
Patients in whom a contraindication <strong>for</strong> transplantation exists or those who are felt not to be<br />
candidates <strong>for</strong> other reasons are returned to their referring physicians <strong>for</strong> ongoing care. Some<br />
patients may not require transplantation at the time of assessment. These patients will be<br />
periodically reviewed by the transplant team, with follow-up clinical and laboratory<br />
investigations. These are done at three to twelve month intervals and will vary from individual<br />
to individual.<br />
When a patient is activated, the Program Assistant copies the following in<strong>for</strong>mation as well as<br />
any other pertinent in<strong>for</strong>mation and places it in a brown envelope in the patient's BCT chart.<br />
These copied reports are transported to the hospital by the <strong>Clinical</strong> Coordinator and the<br />
in<strong>for</strong>mation from the envelope becomes part of the in-hospital chart at the time of transplant.<br />
Copies of:<br />
Patient demographics<br />
Social work consult<br />
Psychologist consult<br />
Anaesthesia consult<br />
Initial and most recent Dietician consult<br />
All recent physician's consults<br />
Summary blood sheet<br />
Most recent virology results<br />
VGH ABO report<br />
Imaging Reports<br />
Alcohol and Drug Contract and Consult (See Appendix O: Contract For Abstinence)<br />
Original surgical consent <strong>for</strong>m signed by both surgeon and patient. (cc: BCT patient chart)<br />
(See Appendix M: Consent <strong>for</strong> Surgical care and Transfusion of Blood Products)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 6<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>1.4 ACTIVATION CONT.<br />
All preoperative investigations become a permanent part of the BCT Chart. A letter outlining<br />
the assessment and plan <strong>for</strong> follow up is written by the transplant hepatologist and the surgeon<br />
and sent to the referring specialist with copies to the family doctor and to the BCT chart after<br />
each visit to the BCT clinic. Nursing Assessment is charted on the progress notes of the BCT<br />
chart. When a patient is ready <strong>for</strong> activation a Recipient Activation <strong>for</strong>m is filled out (See<br />
Appendix N) and remains in the BCT chart. A letter is sent to the referring specialist, with<br />
copies to the family doctor and the patient in<strong>for</strong>ming them of the activation. When patient is<br />
placed on Active <strong>Liver</strong> Transplant list, the <strong>Clinical</strong> Coordinator reviews the updated active list<br />
to ensure accuracy.<br />
Critical recipient-specific listing items are documented in the BCT patient chart as well as on<br />
the Active <strong>Liver</strong> List. The Active List is updated as necessary to change status, weight, etc. The<br />
Active <strong>Liver</strong> List is discussed and reviewed at the weekly <strong>Liver</strong> Team rounds. Any changes to<br />
the Active List shall be made under the direction of the transplant physician and/or surgeon on<br />
call.<br />
A copy of the Active <strong>Liver</strong> List is kept in Recipient Coordinator’s On-Call Binder. Each<br />
member of the <strong>Liver</strong> Transplant team receives an updated list at weekly <strong>Liver</strong> Team meetings.<br />
An updated list shall be distributed to the on call transplant physician, transplant surgeon and<br />
<strong>Clinical</strong> Coordinator as changes occur.<br />
In addition to other in<strong>for</strong>mation, patient's home address, phone number, contact number,<br />
referring specialist and family doctor are found on the “Extra-Renal Transplant Waiting List<br />
Demographic” <strong>for</strong>m, which is located in the <strong>Clinical</strong> Coordinators on call book.<br />
(See Appendix Q: When a <strong>Liver</strong> Becomes Available)<br />
<strong>4.</strong>1.5 PATIENT DEEMED NOT TO BE TRANSPLANT CANDIDATE<br />
Patients who are considered unsuitable <strong>for</strong> transplantation and there<strong>for</strong>e discharged from BC<br />
Transplant's follow-up care are in<strong>for</strong>med of the decision by the <strong>Clinical</strong> Coordinator and<br />
offered the opportunity to meet with the liver transplant team members <strong>for</strong> a face to face<br />
meeting. The Medical and Surgical Director of the <strong>Liver</strong> Transplant Program writes a letter to<br />
the referring physician and the patient’s primary care physician in<strong>for</strong>ming them of the decision.<br />
Patients in whom a contraindication <strong>for</strong> transplantation exists or those who are felt not to be<br />
candidates <strong>for</strong> other reasons are returned to their referring physicians <strong>for</strong> ongoing care.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 7<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>2.1 DONOR COORDINATION<br />
<strong>4.</strong>2 Transplant<br />
When a donor liver becomes available, the transplant surgeon on call and hepatologist review<br />
the list of activated patients with compatible blood type to the donor and select the recipient<br />
based on medical urgency, size compatibility and waiting time on the list.<br />
Patients on the waiting list are discussed at the weekly activation rounds. Changes in status are<br />
in accordance with the accepted Canadian Society of <strong>Transplantation</strong> (CST) criteria (i.e., status<br />
1 to 4).<br />
Patients who are assigned a higher priority status are given preference <strong>for</strong> transplantation (if an<br />
organ becomes available) compared to patients who have lower CST priority status listing.<br />
<strong>4.</strong>2.2 RECIPIENT COORDINATION<br />
(See Appendix R: VGH Transplant Checklist)<br />
<strong>4.</strong>2.3 PRE-OPERATIVE PROTOCOL<br />
When a suitable donor organ has been identified, the recipient will be admitted to Vancouver<br />
General Hospital and assessed by the hepatologist on call. Pre-op blood work and a chest X-ray<br />
is done. If no contraindications to transplantation have arisen, the patient is prepared <strong>for</strong><br />
surgery.<br />
(See Appendix B: Pre-<strong>Liver</strong> Transplant - Adult)<br />
<strong>4.</strong>2.4 BACK-UP<br />
Occasionally a second potential recipient is prepared <strong>for</strong> transplant in the event the first<br />
recipient is found to be unsuitable.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 8<br />
See Page 1 <strong>for</strong> disclaimer
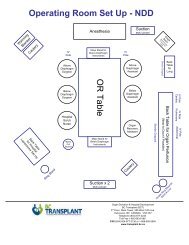
<strong>4.</strong>2.5 TRANSPLANT PROCEDURE<br />
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
The technical aspects of liver transplantation are complex. The procedure has been modified in<br />
many ways over the years to account <strong>for</strong> concerns regarding physiological stability during the<br />
transplant procedure and has been further modified to accommodate split liver, partial liver and<br />
living-related liver transplantation. The procedure is described as an orthotopic liver<br />
transplantation, which means replacing the liver in the same location in the body.<br />
The liver transplant actually requires four surgeries. These are listed as follows:<br />
i. Donor hepatectomy<br />
The liver is removed along with other organs, such as the heart, lung, pancreas and kidneys.<br />
Occasionally, the liver is split into two during this process and usually a portion of the organ<br />
goes to a child and the remaining liver goes to an adult. During this procedure, the anatomy of<br />
the donor is assessed and the liver is assessed <strong>for</strong> fat content, size and the presence of any<br />
tumors or abnormalities, which may affect the recipient operation. The organ can be kept in ice<br />
<strong>for</strong> up to 24 hours. However, the longer the storage time, the more likely there is going to be an<br />
ischemic reperfusion injury due to lack of nutrients and oxygen to the liver. There<strong>for</strong>e, it is<br />
desirable to keep the cold ischemic time, i.e., the time the liver is stored on ice, as short as<br />
possible, preferably under 12 hours.<br />
ii. Recipient hepatectomy<br />
The recipient surgery is divided into three procedures:<br />
a. On entering the abdomen, the surgeon per<strong>for</strong>ms a careful assessment of the liver and<br />
other intra-abdominal structures.<br />
b. Rarely, an unexpected abnormality such as an advanced malignancy is found that<br />
precludes transplantation. A back-up recipient may then be brought in.<br />
c. The diseased organ is removed in a way that preserves vessels and the bile duct to<br />
permit re-anastomosis to the graft.<br />
The anesthesia <strong>for</strong> this particular procedure is quite complex. The patient requires intensive<br />
monitoring during the procedure. This requires a catheter in the radial artery at the wrist, in the<br />
central vein near the heart <strong>for</strong> monitoring pressures and <strong>for</strong> rapid infusion of fluids. The patient<br />
generally has compression devices on the legs to prevent blood clots from <strong>for</strong>ming in the legs<br />
during the prolonged procedure. The entire chest and abdomen, armpit and groin are prepared<br />
should a venous bypass be required. Venous bypass allows flow of the blood from the inferior<br />
vena cava below the liver, which is normally clamped off during the operation, to leave the<br />
body, go through a pump and enter the body again above the liver. Patients who have heart<br />
disease or metabolic conditions, such as amyloidosis may not tolerate vena cava clamping<br />
during the procedure and may require a venous bypass. The venous bypass catheter takes blood<br />
from the saphenous vein in the groin and replaces it through the axillary vein in under the<br />
armpit. There<strong>for</strong>e, incisions may be necessary in the groin and armpit when this procedure is<br />
per<strong>for</strong>med.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 9<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>2.5 TRANSPLANT PROCEDURE CONT.<br />
iii. Back table preparation<br />
Be<strong>for</strong>e the liver is transplanted into the recipient, it is prepared in a separate location in the<br />
operating room. This is called the “back table preparation". The liver is inspected, perhaps<br />
biopsied, the anatomy is confirmed and any abnormalities, injuries or unusual findings detected<br />
and dealt with. The liver is modified to fit the recipient’s anatomy if necessary and the vessels<br />
and bile duct are optimized <strong>for</strong> transplant.<br />
iv. <strong>Transplantation</strong><br />
Once the liver has been prepared in the back table, the diseased liver is removed and the<br />
transplant itself begins. There are two commonly used recipient procedures. One is the<br />
standard orthotopic procedure, which is generally used <strong>for</strong> patients with tumors and whole<br />
organ transplants, where the vena cava, the large vein that goes to the heart, is removed with the<br />
diseased liver. A second technique, termed “piggyback” technique is when the recipient’s vena<br />
cava is left intact, the liver is removed from the cava and the hepatic veins are sewn to the<br />
hepatic veins of the donor liver, leaving the patient’s vena cava as well as the transplanted vena<br />
cava intact. The first step of the recipient procedure is the anastomosis, the suprahepatic vena<br />
cava first, followed by the infrahepatic vena cava.<br />
The liver can be either washed out with cold lactated Ringers solution or some IV solution that<br />
washes out the potassium and preservative solution, or the patient’s portal blood can be run<br />
through the liver and allowed to run out the vena cava from below through a vent until such<br />
time that the liver has been washed out with the patient’s own blood. This blood is usually<br />
saved in a cell saver system, which scavenges any blood that is allowed to leave the body and is<br />
re-transfused once the red cells have been washed. This cuts down the need <strong>for</strong> allogeneic blood<br />
transfusions.<br />
Once the vena cava has been reconstructed, the portal vein is reconstructed, which when<br />
completed allows <strong>for</strong> reperfusion of the liver. The next procedure is to reconstruct the hepatic<br />
artery, which is done is various ways, generally not leaving too short of an artery or too<br />
redundant an artery. Good flow through the portal vein and hepatic artery is mandatory <strong>for</strong><br />
survival of the organ. The quality of the storage can be assessed by the stiffness of the liver, the<br />
rapidity of preservation and the fact that the liver may make bile in the early reperfusion period.<br />
<strong>Liver</strong>s that contain a lot of fat or were in storage <strong>for</strong> a prolonged period of time may function<br />
poorly at first. In the third stage of the operation, the bile duct is reconnected. If the biliary<br />
system of the recipient is adequate an intraoperative cholangiogram may be done to assess <strong>for</strong><br />
major bile leaks or obstruction.<br />
The donor bile duct is sewn to the recipient bile duct so that the sphincter mechanism in the<br />
distal end is still intact. Sometimes a small stent is placed across the sphincter of Oddi to reduce<br />
the chance of a bile leak. The stent usually floats out on its own in the postoperative period but<br />
may have to be removed endoscopically.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 10<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>2.5 TRANSPLANT PROCEDURE CONT.<br />
iv. <strong>Transplantation</strong> cont.<br />
If the recipient’s bile duct is diseased or if a split liver is being transplanted Rouxtoentoy<br />
choledochojejunostomy may be per<strong>for</strong>med. In this case, a loop of bowel is sutured to the<br />
intrahepatic bile duct to serve as conduit <strong>for</strong> bile drainage. Once the bile duct is reconstructed,<br />
the gall bladder is removed and the liver is checked <strong>for</strong> any bleeding.<br />
If no bleeding is detected, up to three drains are placed into the abdominal cavity, usually one<br />
under each leaf of the diaphragm and one by the bile duct. The abdomen is then closed and the<br />
patient goes into the Intensive Care Unit <strong>for</strong> early postoperative management.<br />
Immunosuppressive treatment is started in the operating room to minimize the risk of rejection.<br />
The transplant surgeon is responsible <strong>for</strong> completing the BC Transplant Cooler sheet (Part B)<br />
and returning it to the BCT Organ Donation and Hospital Development (ODHD) Department.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 11<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>3.1 IN-HOSPITAL CARE<br />
<strong>4.</strong>3 Post-Transplant<br />
After the transplant operation, the patient is transferred to the Intensive Care Unit (ICU).<br />
Management in the ICU specifically relates to the identification of early post-transplant<br />
complications such as bleeding, metabolic abnormalities, perfusion abnormalities, ventilatory<br />
support and sepsis. The patient is carefully monitored with tests, hemodynamic monitoring and<br />
clinical examination. Most patients will spend 24 to 48 hours in the ICU be<strong>for</strong>e being<br />
transferred to the Transplant Unit. Occasionally, patients with serious complications or<br />
respiratory problems may have a more prolonged ICU stay.<br />
(See Appendix C: <strong>Liver</strong> Transplant Post-operative Orders in ICU)<br />
From the ICU, the patient will be transferred to the transplant unit. Postoperative care of the<br />
patient involves standard surgical nursing care, nutritional support, mobilization, medical and<br />
immunosuppressive therapy, monitoring <strong>for</strong> rejection, sepsis, or biliary tract complications and<br />
education <strong>for</strong> the patient and his/her family. Psychological interventions are available to assist<br />
the patient in coping with inevitable stresses and <strong>for</strong> anxiety, mood and pain management.<br />
The drains are removed in the early postoperative period except <strong>for</strong> the one by the bile duct,<br />
which is usually left <strong>for</strong> about a week or until the patient is on a regular diet and no bile leak is<br />
detected.<br />
<strong>4.</strong>3.2 EARLY COMPLICATIONS<br />
The early complications after a liver transplant fall into four major categories.<br />
The first includes surgical complications: which include intra-abdominal bleeding, vascular<br />
thromboses and bile leaks or bile strictures. A bile leak is an occasional but serious<br />
complication of transplant operations. Patients typically have abdominal pain, ongoing jaundice<br />
and sepsis. Diagnosis may be made by HIDA scan or cholangiogram. Sometimes patients can<br />
be managed by the placement of a stent at the time of an ERCP. Patients may require reoperation<br />
<strong>for</strong> bile duct reconstruction.<br />
The second category is primary non-function: which is another complication that the liver<br />
itself may not work adequately postoperatively. This is termed primary non-function and may<br />
be due to multiple factors, both patient and graft. Complete primary non-function is life<br />
threatening and occurs in only 2% of transplants. The only option is retransplantation on an<br />
urgent basis.<br />
The third category is infection: Bacterial, fungal or viral. These are treated with appropriate<br />
antimicrobial agents (See Appendix I & J <strong>for</strong> treatment guidelines).<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 12<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>3.2 EARLY COMPLICATIONS CONT.<br />
The fourth category is rejection: Acute rejection occurs in approximately 30 to 40% of the<br />
patients. This is usually suspected by an increase in liver enzymes. A liver biopsy is per<strong>for</strong>med<br />
to confirm the diagnosis. Treatment is with Methylprednisolone (SoluMedrol ® ) 10mg/kg per<br />
day <strong>for</strong> three days. Patients with steroid resistant rejection may require antibody treatment<br />
(ATG) and/or alternate immunosuppressive regimens.<br />
Anti-rejection Protocols and Target Levels:<br />
Anti-rejection: medications <strong>for</strong> liver transplant recipients include:<br />
1. Tacrolimus: Initial oral dose is 0.03 mg/kg/ dose given every 12 hours <strong>for</strong> the first few<br />
days post-transplant. Once liver function has been established increase dose to 0.12 to<br />
0.15 mg/kg/day divided every 12 hours to achieve therapeutic concentrations<br />
(See Appendix D: Table - Target Cyclosporine/Tacrolimus Blood Concentrations)<br />
2. Azathioprine: 1 mg/kg PO daily<br />
3. Methylprednisolone: IV daily<br />
a. Day 0 – 500 mg<br />
b. Day 1 – 200 mg<br />
c. Day 2 – 160 mg<br />
d. Day 3 – 120 mg<br />
e. Day 4 – 80 mg<br />
f. Day 5 – 40 mg followed by<br />
<strong>4.</strong> Prednisone: 20 mg (or 0.3 mg/kg) PO daily. Dose is tapered over 6 months so patient is<br />
steroid free by 6 months<br />
<strong>Guidelines</strong> <strong>for</strong> Use of Other Immunosuppressive Agents:<br />
1. IL-2 Receptor Blockers: Basiliximab (Simulect )<br />
The use of Basiliximab is restricted to patients who are heading into a liver transplant with<br />
renal impairment. For patients with renal impairment the use of a calcineurin inhibitor <strong>for</strong><br />
induction may aggravate renal impairment and hinder post-transplant renal recovery. Under<br />
these circumstances, our program prefers to use an induction with an IL2 receptor<br />
antagonist, followed by either delayed low-dose Tacrolimus or, if renal recovery does not<br />
occur, continued avoidance of Tacrolimus with the use of Mycophenolate Mofetil<br />
plus/minus Sirolimus.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 13<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>3.2 EARLY COMPLICATIONS CONT.<br />
2. Mycophenolate Mofetil (CellCept )<br />
In the maintenance phase, Mycophenolate Mofetil (MMF) use is restricted to the following<br />
indications:<br />
a. Renal dysfunction: Under these circumstances, in order to allow the use of low-dose<br />
calcineurin inhibitors or, in some cases, no calcineurin inhibitor. Mycophenolate<br />
Mofetil is used.<br />
b. Graft rejection: In circumstances in which graft rejection occurs despite the use of<br />
Tacrolimus at therapeutic levels, Mycophenolate Mofetil will be used. Once graft<br />
function has stabilized, Mycophenolate Mofetil use may be discontinued after three<br />
to six months.<br />
c. Calcineurin neurotoxicity: In circumstances where neurotoxicity has occurred to a<br />
calcineurin inhibiting agent, Mycophenolate Mofetil use will be indicated on an<br />
indefinite basis.<br />
d. Mycophenolate Mofetil use as a steroid-sparing agent: There may be circumstances<br />
in which patient’s should be weaned off maintenance Prednisone, i.e. osteoporosis,<br />
osteopenia, diabetic mellitus, etc. and <strong>for</strong> which patients are either intolerant of<br />
Azathioprine or the continued use of Azathioprine is inadequate to maintain a<br />
rejection-free allograft. Under these circumstances, Mycophenolate Mofetil may<br />
have to be used on an indefinite basis.<br />
The goal is <strong>for</strong> all patients that are clinically stable and have reached one year on initial<br />
immunosuppression with Mycophenolate to switch to Azathioprine 1 mg/kg/day PO except<br />
patients with the following:<br />
<br />
<br />
<br />
Calcineurin inhibitor nephrotoxicity or neurotoxicity despite therapeutic<br />
calcineurin inhibitor concentrations<br />
Calcineurin inhibitor hypersensitivity reactions or microangiopathy<br />
Multiple rejection episodes (≥ 2 rejections within the first year post transplant),<br />
despite adequate maintenance immunosuppression, including the inability to<br />
discontinue steroids<br />
3. Sirolimus (Rapamune ® )<br />
The use of Sirolimus by the <strong>Liver</strong> Transplant Program is on a case by case individualized<br />
basis. Due to an increased risk of hepatic artery thrombosis (HAT) in de novo transplant<br />
recipients, Sirolimus should not be used within the first 3 months of transplantation. The<br />
risk/benefit ratio of Sirolimus use in any liver transplant recipients must be discussed with<br />
the liver transplant team and the patient. Sirolimus has a long half-life (around 72 hours)<br />
and takes about 7 to 10 days to reach therapeutic level. There<strong>for</strong>e it should be used with<br />
another agent until therapeutic level is reached. (See Appendix E: Target Sirolimus<br />
Therapeutic Blood Concentrations)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 14<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>3.2 EARLY COMPLICATIONS CONT.<br />
To date, Sirolimus has been used when immunosuppression is required with low-dose<br />
Tacrolimus levels. The circumstances in which this drug may be used would be in patients<br />
who are suffering from ongoing renal dysfunction or calcineurin inhibitor toxicity and<br />
Mycophenolate Mofetil use alone is inadequate either because the patient cannot tolerate<br />
MMF or because of the risk of ongoing rejection<br />
(See Appendix F: Application <strong>for</strong> Sirolimus) (Also in Chapter 7, Section 7.9)<br />
<strong>4.</strong>3.3 Exceptional Distribution - Follow-up of Recipients<br />
It is recognized that in exceptional circumstances and compassionate reasons, a liver may be<br />
transplanted even when there may be a contraindication during donor assessment (e.g.,<br />
incomplete donor screening). If these conditions exist, an organ may be released <strong>for</strong> transplant<br />
only under exceptional distribution as per Health Canada requirements. The process is<br />
documented on an Exceptional Distribution Form by the BCT Organ Donation Coordinator.<br />
The transplanting physician must authorize the exceptional distribution including obtaining<br />
in<strong>for</strong>med consent of the recipient. Copies of the exceptional distribution <strong>for</strong>m are to be<br />
included in the Recipient chart.<br />
It is important that in all cases, appropriate follow-up of recipients is per<strong>for</strong>med by the posttransplant<br />
medical care team. Each exceptional distribution is to be reviewed and assessed by<br />
the team <strong>for</strong> any follow-up treatment and diagnosis.<br />
Risk <strong>for</strong> Viral Mediated Disease Transmission<br />
In Exceptional Distribution cases involving risk <strong>for</strong> viral mediated disease transmission, the<br />
following will be faxed from BCT Quality Assurance to the transplant hospital or outpatient<br />
location:<br />
1) Fax Coversheet - Required Medical Follow-up <strong>for</strong> Transplant Recipient(s)<br />
(See Appendix S)<br />
2) Copy of the Exceptional Distribution Form<br />
3) Reference - Recommended Follow-up Testing <strong>for</strong> Recipients Transplanted under<br />
Risk <strong>for</strong> Viral Mediated Disease Transmission (See Appendix S)<br />
The post transplant Coordinator at VGH will ensure the above documents are reviewed by the<br />
post-transplant medical care team and the recommended follow-up is per<strong>for</strong>med at the required<br />
intervals.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 15<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>4 Outpatient Follow-up<br />
<strong>4.</strong><strong>4.</strong>1 AMBULATORY CARE PHASE<br />
Patients typically remain in the hospital <strong>for</strong> less than two weeks. After discharge from hospital,<br />
they are usually seen in the Post Transplant Clinic on a daily basis until their wounds are well<br />
healed and the staples and drains have been removed. The physician sees them twice weekly <strong>for</strong><br />
the first four weeks and weekly <strong>for</strong> the next few months. For patients with no major<br />
complications, frequency of visits is gradually reduced to monthly <strong>for</strong> the remaining part of the<br />
first year and approximately every two to three months <strong>for</strong> the next two years. Psychological<br />
services are available to assist patients with their emotional adjustment issues.<br />
Blood tests are done twice weekly <strong>for</strong> the first few months and if stable, biweekly and then<br />
monthly by the end of the first year. The blood tests are to monitor liver and renal function,<br />
blood counts, blood levels of immunosuppressive medication and screening <strong>for</strong> common<br />
complications of immunosuppression such as CMV disease. Patients who had a hepatoma are<br />
also followed with alpha-fetoprotein levels and chest X-rays every four months <strong>for</strong> the first<br />
three years.<br />
At six months, twelve months and every year thereafter, patients have more extensive<br />
investigations, which include hepatitis serology, cholesterol, hemoglobin A1C and ultrasound<br />
of the abdomen. The purpose of these tests is to monitor possible side effects of<br />
immunosuppressive medications and screen <strong>for</strong> new or recurrent viral infection.<br />
Patients develop a close relationship with the transplant team and have an understandable<br />
tendency to call on the transplant team <strong>for</strong> all their health concerns. However, the transplant<br />
physicians and nurses are neither able to nor necessarily the best qualified to advise on general<br />
health concerns or routine follow-up and it is expected that the family physician and referring<br />
specialist will continue to take primary responsibility <strong>for</strong> their general medical care. The<br />
laboratory investigations that are done prior to each clinical visit and also the “mini” blood<br />
work per<strong>for</strong>med <strong>for</strong> routine interval monitoring.<br />
(See Appendix G: VHHSC Standing Lab Orders)<br />
Hepatitis B protocol:<br />
(See Appendix H: Protocol <strong>for</strong> Hepatitis B)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 16<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>2 IMMUNIZATION<br />
Immunization in Immunocompromised Hosts:<br />
General Principles:<br />
<br />
<br />
<br />
<br />
<br />
<br />
Maximize benefit while minimizing harm<br />
Make no assumptions about susceptibility or protection<br />
A history of childhood infection or previous immunization may be irrelevant<br />
Immunize at the time when maximum immune response can be anticipated<br />
Immunize early, when immunologic decline is predictable<br />
Delay immunization if the immunodeficiency is transient (if this can be done<br />
safely)<br />
Stop or reduce immunosuppression to permit better vaccine response<br />
Consider the immunization environment broadly<br />
Spread of vaccine strain varicella to family members of the vaccine<br />
Avoid live vaccines, unless<br />
Data are available to support their use<br />
The risk of natural infection is greater than the risk of immunization<br />
Monitor vaccines carefully and boost aggressively<br />
The magnitude and duration of vaccine-induced immunity are often reduced<br />
Some vaccine strain organisms can persist <strong>for</strong> years in compromised hosts<br />
Source: Canadian Immunization Guide, 6 th Edition<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 17<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>2 Immunization Cont.<br />
Solid Organ Transplant Candidate<br />
The number of immunocompromised people in Canadian society is steadily increasing <strong>for</strong> a variety of reasons,<br />
including the accumulation of long-term survivors after organ transplantation. Apart from the importance of<br />
providing protection to the individuals, the increasing number of susceptible immunocompromised persons may also<br />
be of public health importance. One general principle of immunization of immunocompromised individuals is to<br />
immunize at a time when maximum immune response can be anticipated. Our goal is to have every Solid Organ<br />
Transplant Candidate within <strong>British</strong> Columbia complete all of their recommended vaccine series BEFORE they<br />
have their transplant. This will maximize benefit while minimizing harm.<br />
Organ<br />
Tdap/<br />
Td<br />
IPV<br />
Hepatitis A<br />
Hepatitis<br />
B<br />
Meningococcal<br />
Quadrivalent<br />
Conjugate<br />
Pneumococcal<br />
(polysaccharide<br />
only)<br />
Hib Influenza MMR Varicella<br />
Kidney<br />
<br />
<strong>Liver</strong> <br />
Pancreas<br />
<br />
Lung <br />
Heart<br />
<br />
<br />
Live Vaccines:<br />
MMR Vaccine <strong>for</strong> susceptible adults born after 1956 - 2 doses minimum 1 month apart<br />
Varicella Vaccine <strong>for</strong> any susceptible (test <strong>for</strong> VZIgG) adult - 2 doses minimum 1 month apart<br />
Live Vaccines must be given at least 4 weeks BEFORE transplantation<br />
Booster Doses:<br />
Td every 10 years <strong>for</strong> life<br />
Influenza every year <strong>for</strong> life<br />
Pneumococcal - a once only revaccination after 5 years<br />
References: Canadian Immunization Guide 7th Edition, BC Centre <strong>for</strong> Disease Control Immunization Program Manual,<br />
Loutan, L. Vaccination of the Immunocompromised Patient. Biologicals, 1997,25, 231-236., Avery Rk and<br />
Ljungman, P. Prophylactic Measures in the Solid-Organ Recipient be<strong>for</strong>e <strong>Transplantation</strong>: CID 2001;33:S15-<br />
S21.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 18<br />
See Page 1 <strong>for</strong> disclaimer
<strong>4.</strong><strong>4.</strong>2 Immunization Cont.<br />
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Solid Organ Transplant Recipients<br />
There is potential <strong>for</strong> serious illness and death in both the under immunization and over immunization of<br />
these people. Immunization of those with significant immunodeficiency should be per<strong>for</strong>med only in<br />
consultation with experts.<br />
Organ<br />
Tdap<br />
/Td<br />
IPV<br />
Hepatitis<br />
A<br />
Hepatitis<br />
B<br />
Meningococcal<br />
Quadrivalent<br />
Conjugate<br />
Pneumococcal<br />
(polysaccharide<br />
only)<br />
Hib<br />
Influenza<br />
Kidney <br />
<strong>Liver</strong> <br />
Pancreas <br />
Lung <br />
Heart <br />
<br />
Booster Doses<br />
Td every 10 years <strong>for</strong> life<br />
Influenza every year <strong>for</strong> life<br />
Pneumococcal - a once only revaccination after 5 years<br />
ALL Live Vaccines (such as MMR and Varicella) are Contraindicated after transplantation<br />
References: Canadian Immunization Guide 7th Edition, BC Centre <strong>for</strong> Disease Control Immunization Program<br />
Manual.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 19<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
BCCDC - Communicable Disease Control Immunization Program - Immunization of Special Populations<br />
January 2010 VACCINES RECOMMENDED FOR IMMUNOSUPPRESSED CLIENTS<br />
IMMUNE-<br />
SUPPRESSING<br />
CONDITIONS<br />
Asplenia (anatomic or<br />
functional), including<br />
sickle cell disease<br />
Congenital<br />
immunodeficiency<br />
(e.g., Complement,<br />
properdin, or factor D<br />
deficiency)<br />
Hematopoietic Stem<br />
Cell Transplant<br />
(HSCT)recipient<br />
Meningo<br />
<br />
Pneumo<br />
<br />
VACCINES<br />
Special Indications<br />
Hib<br />
Hep A Hep B Influenza<br />
<br />
Routine<br />
Inactivated<br />
x x x x x <br />
x x x x x C <br />
x x x x x x x <br />
HIV + adult x x x x x x <br />
Immunosuppressive<br />
therapy<br />
x x x x C <br />
Islet cell transplant<br />
candidate or recipient<br />
x x x x x <br />
Kidney<br />
disease(chronic) (predialysis<br />
and dialysis<br />
clients)<br />
x x x x <br />
<strong>Liver</strong> disease<br />
(chronic)<br />
x x x x x x<br />
Hepatitis B (chronic) x x x x x<br />
Hepatitis C (chronic) x x x x x x<br />
Malignant neoplasm x x x x C<br />
Solid organ (liver,<br />
heart, lung, kidney)<br />
transplant candidate<br />
or recipient<br />
x x x liver liver kidney x x <br />
Meningo = Meningococcal conjugate vaccines<br />
Pneumo = Pneumococcal conjugate and/or polysaccharide vaccine<br />
Yearly influenza immunization is indicated <strong>for</strong> all immunosuppressed individuals ≥ 6 months of age.<br />
Special considerations exist.<br />
C = Contraindicated<br />
This table is intended as a guideline only. For more in<strong>for</strong>mation, refer to the appropriate health condition<br />
in this Section or BC Communicable Disease Control Manual, Chapter 2, Section VII Biological Products<br />
Live<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 20<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>3 PROPHYLACTIC ANTIBIOTIC DENTAL COVERAGE<br />
As a general rule, we believe that all teeth should be preserved if at all possible. If this includes<br />
root canal or periodontal work, this should be done when the patient is well and ideally after<br />
transplantation.<br />
Pre-Transplant Patients<br />
These patients differ fundamentally from heart valve patients in two ways. The first is that it’s<br />
very easy to develop spontaneous bacterial peritonitis with dental procedures. Most of these<br />
patients will have ascites and there<strong>for</strong>e are at risk of this. The second problem is that because of<br />
their blood clotting abnormalities, things as simple as teeth cleaning can lead to progressive<br />
bleeding. Our major concern with cleaning and dental extractions, is that the patient will<br />
develop discom<strong>for</strong>t related to this and there<strong>for</strong>e will require some analgesia which could<br />
precipitate encephalopathy. Secondly, they can bleed from this and the swallowed blood and<br />
protein can also precipitate encephalopathy. Thirdly, they can become infected and not only<br />
can this also cause spontaneous bacterial peritonitis (SBP) but can also lead to encephalopathy.<br />
There<strong>for</strong>e, as a general rule, patients and dental staff should follow these general guidelines.<br />
1. Pre-transplant patients should generally not undergo either cleaning or any periodontal<br />
work unless they are very early in the course of their disease. The patient usually will be<br />
in<strong>for</strong>med as to whether or not he/she could proceed with aggressive dental work.<br />
2. Fillings above the gum line should be treated only with Amoxicillin 2 grams PO one hour<br />
prior to the dental procedure.<br />
3. Fillings below the gum line, including root canals, should be per<strong>for</strong>med in pre-transplant<br />
patients only when necessary. These patients should receive Amoxicillin 2 grams PO one<br />
hour be<strong>for</strong>e their dental procedure and Penicillin V 300 mg PO four times daily <strong>for</strong> four<br />
days.<br />
<strong>4.</strong> Patients requiring standard extractions should receive Amoxicillin 2 grams PO one hour<br />
prior to dental procedures and Penicillin V 300 mg PO four times daily <strong>for</strong> ten days<br />
thereafter.<br />
5. As mentioned above, we try to preserve every tooth. In the event that extraction is required<br />
of teeth 36, 37, 38, 46, 47 and 48, the addition of Decadron is usually of benefit. This helps<br />
to reduce swelling and there<strong>for</strong>e decreases analgesia requirement. The dosage is 4 mg on<br />
the morning of their procedure, 2 mg on the morning of post op day 1 and 1 mg on each of<br />
the subsequent two days. All of this of course is in addition to the Amoxicillin and<br />
Penicillin V as mentioned in number 4 above.<br />
6. Patients who are allergic to Penicillin (non skin rash only) should receive a single dose of<br />
Clindamycin 600 mg PO instead of the 2 grams of Amoxicillin PO and should receive<br />
Clindamycin 300 mg PO three times a day instead of the Penicillin V.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 21<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>3 PROPHYLACTIC ANTIBIOTIC DENTAL COVERAGE CONT.<br />
7. Patients undergoing an elective root canal with localized abscesses should receive 48 hours<br />
of Penicillin V PO prior to their dental procedures at 300 mg four times a day which should<br />
then be continued <strong>for</strong> at least four days thereafter.<br />
Post Transplant Patients<br />
The American Heart Association <strong>Guidelines</strong> <strong>for</strong> the Prevention of Infective Endocarditis<br />
recommend antibiotic prophylaxis be<strong>for</strong>e dental procedures ONLY <strong>for</strong> patients who have a<br />
history of previous infective endocarditis, or who have had cardiac valve replacement, or<br />
surgically constructed pulmonary shunts, or conduits (1) .<br />
Prophylactic antibiotic coverage <strong>for</strong> dental procedures is recommended ONLY <strong>for</strong> the<br />
following transplant recipients:<br />
<br />
<br />
<br />
<br />
Prosthetic cardiac valve<br />
Previous infective endocarditis<br />
Congenital heart disease (CHD)<br />
Unrepaired cyanotic CHD<br />
months following repair of CHD with any prosthetic material or<br />
device<br />
Repaired CHD with residual defects<br />
Cardiac transplant recipients who develop cardiac valvulopathy<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 22<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>3 PROPHYLACTIC ANTIBIOTIC DENTAL COVERAGE CONT.<br />
Recommended Antibiotic Regimens <strong>for</strong> a Dental Procedure (1)<br />
SITUATION ANTIBIOTIC REGIMEN: SINGLE DOSE 30 TO 60<br />
MIN PRIOR TO PROCEDURE<br />
Adults<br />
Children<br />
Oral Amoxicillin 2 grams 50 mg/kg<br />
Unable to take Oral<br />
Medication<br />
Ampicillin<br />
OR<br />
Cefazolin* or<br />
2 grams IV or IM<br />
1 gram IV or IM<br />
50 mg/kg IV or IM<br />
50 mg/kg IV or IM<br />
Ceftriaxone * *<br />
True Allergy to<br />
Penicillin Allergic<br />
to Penicillins or<br />
Ampicillin - Oral<br />
Cephalexin*<br />
OR<br />
Clindamycin<br />
OR<br />
Azithromycin or<br />
Clarithromycin<br />
2 grams<br />
600 mg<br />
500 mg<br />
50 mg/kg<br />
20 mg/kg<br />
15 mg/kg<br />
Allergic to<br />
penicillins or<br />
ampicillin and<br />
unable to take oral<br />
medication<br />
Cefazolin or<br />
Ceftriaxzone * *<br />
OR<br />
Clindamycin<br />
1gm IV or IM<br />
600 mg IV or IM<br />
50 mg/kg IM or IV<br />
20 mg/kg IV or IM<br />
* Or other first or second generation oral cephalosporin in equivalent adult or pediatric<br />
dosage<br />
**<br />
Cephalosporins should not be used in an individual with a history of anaphylaxis,<br />
angioedema or urticaria with penicillins or ampicillin<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 23<br />
See Page 1 <strong>for</strong> disclaimer
<strong>4.</strong><strong>4.</strong>4 LATE COMPLICATIONS<br />
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Rejection is less common after nine months, although acute rejection can occur at any time<br />
after transplantation. Rejection is almost always confirmed by liver biopsy be<strong>for</strong>e treatment is<br />
instituted. Patients then are treated the same as they are in the immediate perioperative period,<br />
with Methylprednisolone (Solu Medrol ® ), at a dosage of approximately 10 mg/kg IV daily <strong>for</strong><br />
three days. Patients with severe rejection or steroid-resistant rejection may require treatment<br />
with a polyclonal antibody (ATG) IV <strong>for</strong> 7 to 10 days. In addition, they may have their<br />
maintenance immunosuppressive treatment intensified.<br />
CMV infection is common 3 weeks to 6 months after transplantation. Typically, this occurs<br />
in patients who are already CMV positive by CMV PCR testing, as the immunosuppression<br />
decreases the body’s immune surveillance of the virus. Patients may develop generalized<br />
malaise, low-grade fever and often, upper GI complaints. To permit prompt initiation of<br />
therapy, CMV PCR tests are per<strong>for</strong>med routinely according to the CMV Prophylaxis and<br />
Treatment Regimens <strong>for</strong> <strong>Liver</strong> Transplant Recipients (See Appendix I).<br />
These tests are not 100% reliable and diagnosis may have to be confirmed by upper GI<br />
endoscopy or some other method of demonstrating tissue invasion. Patients who are a CMVmismatch,<br />
meaning the donor is positive and the recipient is negative, are at very high risk of<br />
CMV disease.<br />
(See Appendix I: CMV Prophylaxis and Treatment Regimens)<br />
Renal Dysfunction is one of the common complications of long-term immunosuppression.<br />
This is typically associated with calcineurin inhibitors (Cyclosporine and Tacrolimus). Patients<br />
with decreased renal function may need to have their immunosuppressive regime modified.<br />
Those whose serum creatinine continues to rise will be referred to a nephrologist. Occasional<br />
patients may eventually require dialysis.<br />
Hypertension is common after transplantation. This may be related in part to unmasking of<br />
essential hypertension. However, Cyclosporine and Tacrolimus can cause hypertension, partly<br />
through direct effects on blood flow in the kidney. There is a view that calcium channel<br />
blockers may be of benefit, as they cause vasodilatation and preserve renal function. In general,<br />
hypertension in these patients should be treated similarly to that in the non-transplant setting.<br />
Bile duct disease is a common complication of liver transplantation, occurring in up to 15%<br />
of patients. This is typically related to ischemic injury but may be associated with strictures<br />
occurring at the area of anastomosis. Usually patients are asymptomatic and these problems are<br />
detected only on the basis of increasing liver enzymes, however, they may also present with<br />
jaundice or episodes of cholangitis. Rapid identification of the problem is paramount. Patients<br />
require immediate assessment with blood tests, blood cultures and ultrasound. They will often<br />
require an ERCP or percutaneous transhepatic cholangiogram (PTC). Patients with evidence of<br />
biliary tract stenosis may require stenting at the time of the ERCP or placement of a<br />
percutaneous catheter at the time of their PTC. These stents are typically left in place <strong>for</strong> a<br />
period of a few months and exchanged.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 24<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>4 LATE COMPLICATIONS CONT.<br />
Some patients will benefit from this and require no further therapy after their stents are<br />
eventually removed six months later. Not infrequently, patients will ultimately require<br />
reconstructive surgery with the revision of their anastomosis or conversion to Rouxtoentoy.<br />
Patients with significant intrahepatic strictures who continue to develop recurrent cholangitis<br />
may eventually require retransplantation. Initial treatment of patients who develop cholangitis is<br />
usually with a combination of broad spectrum antibiotics with gram negative enterococcal<br />
coverage. The antibiotics are adjusted when culture and sensitivity results are available. If the<br />
patient develops cholangitis and is treated <strong>for</strong> cholangitis at a hospital other than VGH, it is<br />
important that the transplant team be notified.<br />
Diabetes is present in approximately 10% of patients prior to liver transplantation. This is<br />
worsened with the use of Prednisone and calcineurin inhibitors in the post-transplant period.<br />
While in hospital, patients may require insulin, although insulin-dependent diabetes typically<br />
presents several weeks after transplantation. This is particularly true in patients who receive<br />
Tacrolimus. Ten to twenty percent of patients may develop de novo diabetes post-transplant<br />
secondary to steroids and calcineurin inhibitors.<br />
Hyperlipidemia is another long-term complication. Lipid profiles are checked <strong>for</strong> this at the<br />
time of annual post-transplant assessments. Sirolimus is associated with an increased risk of<br />
hyperlipidemia.<br />
Hyperkalemia is another common side effect of Cyclosporine and Tacrolimus. This is usually<br />
readily treated with a potassium exchange resin. Fifteen grams of Kayexalate ® given two to<br />
three times a day is usually sufficient. Patients with peripheral edema are also treated with<br />
Furosemide. It should be noted that those patients who are also receiving sulfa/trimethoprim<br />
(Septra ® ), are at increased risk of hyperkalemia, as trimethoprim has an amiloride - like effect.<br />
Osteoporosis is another important metabolic complication of transplantation. Supplemental<br />
calcium and vitamin D is part of the standard protocol. High-risk patients are evaluated further<br />
with bone densities and if abnormal, are referred to an endocrinologist and bisphosphonates<br />
may be recommended.<br />
Infection with fungus such as Candida is common in the post-transplant setting. Patients who<br />
are colonized with fungus, as demonstrated by routine cultures of body fluids, are treated<br />
prophylactically with Fluconazole at a dosage of 200 mg a day <strong>for</strong> ten days. This usually results<br />
in eradication and it is rare to develop systemic fungemia. Rarely, patients can develop<br />
Cryptococcal meningitis. This is manifest by subtle neurological complaints, variable physical<br />
findings and mild fever. These patients need to be aggressively assessed and treated.<br />
Pneumocystis carinii is an organism, which occasionally causes pneumonia. This occurs in<br />
approximately 2 to 3% of patients. Some transplant programs prophylaxis against pneumocytis<br />
pneumonia (PCP) with the use of Cotrimoxazole. In our experience, the incidence of PCP has<br />
been too low to justify routine prophylaxis.<br />
(See Appendix J: Treatment <strong>for</strong> Other Opportunistic Infections)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 25<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong><strong>4.</strong>4 LATE COMPLICATIONS CONT.<br />
Recurrence of Hepatitis C is essentially universal after transplantation and typically<br />
manifests approximately three months after transplantation. It is characterized by mild to<br />
moderate elevations of the transaminase levels, with a normal alkaline phosphatase and a<br />
gamma GT less than 200 units. The diagnosis should be confirmed by liver biopsy to be sure<br />
there are no other causes of the abnormal liver tests. While some patients have a fairly benign<br />
outcome, most patients develop gradually progressive liver disease that leads to cirrhosis over a<br />
decade or so. Although no treatment has been clearly shown to be effective in the transplant<br />
recipient, patients with aggressive hepatitis should be considered <strong>for</strong> treatment with Pegylated<br />
Interferon and Ribavirin. Occasional patients will develop rapidly progressive liver disease,<br />
with jaundice, accelerated fibrosis and progression to liver failure. This can occur at any time,<br />
but often within a few years of their transplant. Results of retransplantation are poor and the<br />
prognosis of this <strong>for</strong>m of recurrent Hepatitis C is dismal.<br />
Immunologically mediated liver diseases including primary biliary cirrhosis (PBC),<br />
autoimmune chronic hepatitis and primary sclerosing cholangitis can all recur after<br />
transplantation despite immunosuppression. Patients with PBC can be treated with<br />
ursodeoxycholic acid (UDCA). The risk of recurrence is thought to be increased after<br />
discontinuation of steroids; so low-dose Prednisone is sometimes continued in such patients.<br />
Post-transplantation autoimmune hepatitis may require Prednisone <strong>for</strong> prolonged periods.<br />
Finally, some transplant recipients may experience protracted psychological adjustment<br />
problems. Individual and group interventions are available to facilitate long-term emotional<br />
adjustment.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 26<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>5 Pediatric <strong>Transplantation</strong><br />
<strong>4.</strong>5.1 INTRODUCTION<br />
While the general principles of liver transplantation are similar in children and adults, a number<br />
of additional factors must be considered <strong>for</strong> the pediatric patient. First, the size of the pediatric<br />
patient may affect the transplant outcome. Candidates weighing less than 10 kg may be at high<br />
risk <strong>for</strong> transplant complications and the nutritional status of any young patient with liver<br />
disease is a major concern. Second, the immunization status of a child referred <strong>for</strong> liver<br />
transplant evaluation requires thorough review. Children who are potential transplant candidates<br />
should receive an accelerated immunization schedule whose goal is to complete as many of the<br />
primary immunizations as possible prior to the transplant. Third, the vessels that supply blood<br />
to the liver may be quite small in caliber, especially in young infants. Abnormalities of the<br />
hepatic vasculature are relatively common in children and the risk <strong>for</strong> post-transplant vessel<br />
blockage is higher <strong>for</strong> those infants with small caliber vessels. A thorough radiological<br />
assessment of the liver vessels is crucial <strong>for</strong> the pediatric patient prior to undergoing a liver<br />
transplant. Finally, particular attention must be paid to the child’s environment. The<br />
psychosocial needs of the child, the reliability of the child’s caregivers, the stability of the home<br />
environment and religious or cultural beliefs need to be assessed to ensure adequate and<br />
responsible care of the transplanted child after discharge.<br />
<strong>4.</strong>5.2 WHEN TO REFER<br />
As part of the liver transplantation protocol, potential pediatric candidates will undergo a<br />
thorough preoperative evaluation of their liver disease to determine their eligibility <strong>for</strong><br />
transplantation. We prefer to see potential candidates early in their disease course as this<br />
enables us to anticipate any problems as well as to correct any disease associated complications.<br />
In addition, it af<strong>for</strong>ds the transplantation team an opportunity to become familiar with the<br />
patient and their family.<br />
In a child with liver disease, the presence of one or more of the following features indicates<br />
significant hepatic dysfunction and warrants a referral <strong>for</strong> transplant evaluation:<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Progressive jaundice<br />
Diminishing hepatic synthetic function (hypoalbuminemia, coagulopathy unresponsive<br />
to vitamin K, hypoglycemia)<br />
The onset of encephalopathy<br />
Progressive cholestasis/pruritus/refractory cholangitis<br />
Portal hypertension with its complications (variceal bleeding, ascites, hypersplenism)<br />
Growth retardation despite aggressive nutritional therapy<br />
Poor quality of life<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 27<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>5.2 WHEN TO REFER CONT.<br />
The ultimate goal of the transplant evaluation process is to:<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Confirm the diagnosis<br />
Evaluate alternative therapies<br />
Determine potential disease complications<br />
Decide if there are any contraindications <strong>for</strong> transplant<br />
Initiate aggressive nutritional therapy<br />
Review medications<br />
Ensure appropriate immunization schedule<br />
Educate and prepare patient and family<br />
<strong>4.</strong>5.3 WHAT HAPPENS DURING ASSESSMENT<br />
All pediatric candidates are evaluated by members of the pediatric transplantation team<br />
following which a decision is made as to whether the candidate is suitable <strong>for</strong> transplant.<br />
This pediatric multidisciplinary team includes the following consultants: Surgeon,<br />
Gastroenterologist, Intensivist, Microbiologist, Radiologist, Anaesthesiologist, Pathologist,<br />
Psychiatrist, <strong>Clinical</strong> Nurse, Ethicist, Social Worker, Dietician and <strong>Transplantation</strong><br />
Coordinator. Other consultants whose expertise may be needed include Nephrologists,<br />
Hematologists, Neurologists, Respirologists, Immunologists, etc.<br />
During the assessment, a complete history and physical examination is per<strong>for</strong>med and a number<br />
of tests are obtained to assess the extent of the liver disease and confirm the diagnosis. The<br />
patient is screened <strong>for</strong> a variety of viruses and the immunization schedule is reviewed. A<br />
complete nutritional assessment with aggressive dietary management to maximize the growth of<br />
infants with liver disease is an integral part of the pediatric transplant evaluation. During the<br />
assessment phase, the transplant team also provides patients and their families with in<strong>for</strong>mation<br />
about liver transplantation, including the risks and benefits of the procedure and the<br />
transplantation process.<br />
The following tests are routinely completed during this assessment phase:<br />
Complete blood count<br />
Assessment of liver function: AST, ALT, gamma GT, alk phos, total and direct<br />
bilirubin, total protein albumin, PT, PTT, Factor V<br />
Assessment of renal function: serum electrolytes, BUN, Ca, creatinine, PO4, Mg, U/A,<br />
urinary electrolytes, GFR<br />
Other biochemistries: glucose, amylase, immunoglobulins, cholesterol, triglycerides<br />
Viral screen: serology <strong>for</strong> CMV, Hep A IgM, HBsAg, HBcAb, HBsAb, HIV, EBV,<br />
Hep C<br />
PPD<br />
Blood group and match<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 28<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>5.3 WHAT HAPPENS DURING ASSESSMENT CONT.<br />
<br />
<br />
<br />
<br />
<br />
<br />
Other diagnostic tests: alphato1 antitrypsin level, ceruloplasmin, CEA, alpha-fetoprotein<br />
Imaging studies: abdominal ultrasound with doppler, CXR<br />
ECG<br />
Dentistry consult if needed<br />
Ophthalmology consult if required<br />
Immunology consult if indicated<br />
<strong>4.</strong>5.4 ACTIVATION<br />
Once this extensive evaluation is completed, the pediatric multidisciplinary transplant team will<br />
meet and review each candidate to determine eligibility <strong>for</strong> transplantation.<br />
If the candidate has been deemed eligible <strong>for</strong> transplantation, he/she will be placed on the active<br />
list and the family will be given a pager and instructions to communicate any change in their<br />
location or health status to the transplant coordinator. While on the waiting list, the patient and<br />
family will be closely followed by the transplant team.<br />
<strong>4.</strong>5.5 TRANSPLANT OPERATION<br />
The technical aspects of liver transplantation are complex. Several modifications have recently<br />
occurred which have advanced the procedure and its outcome, especially <strong>for</strong> the pediatric<br />
patient. The ability to divide a deceased donor liver and use only a small part of it <strong>for</strong><br />
transplantation into a young infant has had a significant impact in pediatric transplantation. This<br />
procedure is known as a reduced liver transplant. The development of living related liver<br />
transplantation where a parent can donate a part of their liver to the affected child has been<br />
another major achievement in the field.<br />
The operation itself is essentially the same as the adult operation described in section <strong>4.</strong>2.5. The<br />
main difference is that infants and small children will usually receive split livers.<br />
<strong>4.</strong>5.6 POST-TRANSPLANT CARE AND FOLLOW-UP<br />
See sections <strong>4.</strong>3 and <strong>4.</strong>4<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 29<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>4.</strong>6 Appendices<br />
Appendix A<br />
Appendix B<br />
Appendix C<br />
Appendix D<br />
Appendix E<br />
Appendix F<br />
Appendix G<br />
Appendix H<br />
Appendix I<br />
Appendix J<br />
Appendix K<br />
Appendix L<br />
Appendix M<br />
Appendix N<br />
Appendix O<br />
Appendix P<br />
Appendix Q<br />
Appendix R<br />
Appendix S<br />
<strong>Liver</strong> Transplant Referral Form<br />
Pre-<strong>Liver</strong> Transplant Assessment - Adult<br />
<strong>Liver</strong> Transplant Post-operative Orders in ICU<br />
Table <strong>for</strong> Target Tacrolimus / Cyclosporine Blood Concentrations/Assays<br />
Table <strong>for</strong> Sirolimus Target Therapeutic Concentrations<br />
BCT Fax Form: Application <strong>for</strong> Sirolimus, <strong>Liver</strong> Transplant Recipients<br />
VHHSC Standing Lab Orders <strong>for</strong> <strong>Liver</strong> Transplant Program<br />
Protocol <strong>for</strong> Hepatitis B <strong>Liver</strong> Transplant Recipients<br />
CMV Prophylaxis and Treatment Regimes <strong>for</strong> <strong>Liver</strong> Transplant Recipients<br />
Treatment <strong>for</strong> Other Opportunistic Infections in <strong>Liver</strong> Transplant Recipients<br />
Authorization <strong>for</strong> Release of In<strong>for</strong>mation<br />
Consent to Diagnosis, Treatment and Care<br />
Consent <strong>for</strong> Surgical Care and Transfusion of Blood Products<br />
Recipient Activation Form<br />
Contract <strong>for</strong> Abstinence<br />
<strong>Liver</strong> Transplant Baseline Assessment<br />
When a <strong>Liver</strong> Becomes Available<br />
VGH Transplant Checklist<br />
Fax Coversheet and Recommended Follow-up Testing <strong>for</strong> Recipients<br />
Transplanted under Risk <strong>for</strong> Viral Mediated Disease Transmission<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 30<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
LIVER TRANSPLANT REFERRAL FORM<br />
APPENDIX A<br />
Referral Date:__________________________<br />
Last Name: _____________________ First Name:__________________ Initial: ___________<br />
Street Address:___________________________________________________________________<br />
City:________________________ Province: _____________ Postal Code: ________________<br />
DOB: __________________ Age: ________ Sex: _________ Race: ________________________<br />
Home Phone: __________________Other Phone: _____________________________________<br />
Contact Name: ___________________ Phone: _____________Relationship: ______________<br />
GP: ____________________________ Phone: _______________ Fax: _____________________<br />
Address: ______________________________________________________________________<br />
Ref. MD: ________________________ Phone: ________________Fax: _____________________<br />
Address: ______________________________________________________________________<br />
Health Plan: ______________________ Insurance #: __________________________________<br />
Diagnosis: Primary _____________________________________________________________<br />
Secondary ___________________________________________________________<br />
Does patient/family speak and understand English? Yes______ No ______<br />
If No, what language: ___________________ Height:______________Weight: _______<br />
Previous Surgery ___________________________________________________<br />
Is this patient VRE+________<br />
Is this patient MRSA+_________<br />
*PLEASE SEND PERTINENT MEDICAL HISTORY AND DOCUMENTATION – INCLUDING<br />
LAB TESTS AND OTHER PROCEDURAL TESTS AND CONSULTATION NOTES.<br />
Please mail to:<br />
<strong>Clinical</strong> Coordinator<br />
<strong>British</strong> Columbia Transplant<br />
West Tower, 3 rd Floor<br />
555 West 12 th Avenue<br />
Vancouver, BC V5Z 3X7 Phone: (604) 877-2240 Fax: (604) 877-2111<br />
Toll Free: 1-800-663-6189<br />
The completion of this <strong>for</strong>m will expedite your patient’s investigations and subsequent<br />
consideration <strong>for</strong> transplantation. Thank you <strong>for</strong> your cooperation in providing this material.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 31<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 32<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 33<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 34<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 35<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 36<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 37<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 38<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 39<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 40<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix B (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 41<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix C<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 42<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix C (cont.)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 43<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix D<br />
Target Cyclosporine Blood Concentrations <strong>for</strong> <strong>Liver</strong> Transplant Recipients<br />
As of June 2010, in <strong>British</strong> Columbia there are two different types of assays used <strong>for</strong> the determination of<br />
Cyclosporine blood concentrations:<br />
1. Immunoassay (Abbott TDX ® )<br />
2. Mass Spectrometry Assay.<br />
Mass spectrometry results are 24% lower than the Abbott TDX Assay.<br />
You must know which assay was used <strong>for</strong> measuring the Cyclosporine concentrations to interpret the<br />
result. There is a chart below which lists the assays used to monitor Cyclosporine concentrations at different<br />
hospitals in the province.<br />
Time Post<br />
Transplant<br />
(Months)<br />
Cyclosporine<br />
Trough<br />
Concentration<br />
(ng/mL)<br />
Immunoassay<br />
Cyclosporine C 2<br />
(ng/mL)<br />
Immunoassay<br />
Cyclosporine Trough<br />
Concentration<br />
(ng/mL)<br />
Mass Spectrometry<br />
Assay<br />
Cyclosporine C 2<br />
(ng/mL)<br />
Mass<br />
Spectrometry<br />
Assay<br />
0 to 3 300 to 350 1000 250 to 275 750<br />
3 to 6 250 to 300 800 200 to 250 600<br />
6 to 9 200 to 250 600 150 to 200 450<br />
9 to 12 150 to 200 600 125 to 150 450<br />
Greater than 12 125 to150 600 100 to 125 450<br />
Prepared by Nilu Partovi, Pharm D. March 10, 2004<br />
Target Trough Tacrolimus Blood Concentrations <strong>for</strong> <strong>Liver</strong> Transplant Recipients<br />
As of June 2010, in <strong>British</strong> Columbia there are two different types of assays used <strong>for</strong> the determination<br />
of Tacrolimus blood concentrations:<br />
1. Immunoassay (Abbott TDX ® )<br />
2. Mass Spectrometry Assay.<br />
Mass spectrometry results are 24% lower than the Abbott TDX Assay.<br />
You must know which assay was used <strong>for</strong> measuring the Tacrolimus concentrations to interpret<br />
the result. There is a chart below which lists the assays used to monitor Tacrolimus concentrations at<br />
different hospitals in the province.<br />
Time Post-<br />
Transplant<br />
(Months)<br />
Tacrolimus Trough<br />
Blood Concentration<br />
(ng/mL)<br />
12 hours Post-Dose<br />
Immunoassay<br />
Tacrolimus Trough Blood<br />
Concentration (ng/mL)<br />
12 hours Post-Dose<br />
Mass Spectrometry Assay<br />
Less than 1 10 to 15 8 to 12<br />
1 to 3 8 to 12 6 to 9<br />
Greater than 3 5 to 10 4 to 8<br />
For <strong>Liver</strong> Transplant Patients With Hepatitis C or Renal Failure<br />
Less than 1 8 to 12 6 to 9<br />
1 to 3 5 to 10 4 to 8<br />
Greater than 3 5 to 10 4 to 8<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 44<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Cyclosporine and Tacrolimus Assays Used in <strong>British</strong> Columbia<br />
Appendix D (cont.)<br />
HOSPITAL LABORATORY<br />
Vancouver General Hospital<br />
St. Paul’s Hospital<br />
B.C.’s Children’s Hospital<br />
Royal Jubilee Hospital, Victoria<br />
Prince George Regional Hospital<br />
Penticton Regional Hospital<br />
Kootenay Boundary Hospital<br />
Royal Inland Hospital<br />
Kelowna General Hospital<br />
LifeLabs<br />
TYPE OF CYCLOSPORINE<br />
ASSAY AS OF JUNE 2010<br />
Mass Spectrometry<br />
Mass Spectrometry<br />
Abbott TDX Immunoassay<br />
Mass Spectrometry<br />
Abbott TDX Immunoassay<br />
Mass Spectrometry<br />
Sent to Penticton Regional Hospital<br />
Sent to Penticton Regional Hospital<br />
Sent to Penticton Regional Hospital<br />
Mass Spectrometry<br />
The different Mass Spectrometry Assays used at Vancouver General, St. Paul’s Hospital,<br />
Royal Jubilee Hospital and Penticton Regional Hospital produce very similar results.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 45<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix E<br />
Target Whole - Blood Sirolimus Trough Concentrations<br />
For LIVER Transplant Recipients<br />
HPLC-TMS Assay *<br />
TIME POST-TRANSPLANT<br />
(MONTHS)<br />
TROUGH SIROLIMUS<br />
CONCENTRATIONS (NG/ML)<br />
(WHEN USED WITH<br />
TACROLIMUS OR<br />
CYCLOSPORINE +/-<br />
MYCOPHENOLATE AND<br />
STEROIDS)<br />
TROUGH SIROLIMUS<br />
CONCENTRATIONS (NG/ML)<br />
(WHEN SIROLIMUS IS USED AS<br />
A SINGLE AGENT +/- STEROIDS)<br />
Less than 1 10 to 15 12 to16<br />
1 to 3 months 8 to 12 10 to 12<br />
Greater than 3 5 to 10 8 to 12<br />
Prepared by Nilu Partovi, Pharm D, Nov 2008<br />
* HPLC-TMS: High per<strong>for</strong>mance liquid chromatography - Tandem mass spectrometry<br />
Assay is only done at Vancouver General Hospital. Samples must be sent to Vancouver<br />
General Hospital <strong>for</strong> testing.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 46<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix F<br />
BCT FAX FORM: APPLICATION FOR SIROLIMUS LIVER TRANSPLANT<br />
RECIPIENTS<br />
Please complete & fax to Dawn Strong <strong>for</strong> Dr. YOSHIDA at B.C. Transplant (604)- 877-2111<br />
DATE:<br />
TO:<br />
FROM:<br />
Dr. Eric Yoshida<br />
Medical Director, <strong>Liver</strong> Transplant Program, BCT<br />
BCT #:_______________________<br />
Name: Last: _________________________________ First: ______________________<br />
Hospital: _________________________ Hepatologist: _________________________<br />
Indications <strong>for</strong> Sirolimus Use:<br />
1. Patient has developed calcineurin toxicity despite blood concentrations within therapeutic range.<br />
Cyclosporine concentration _________ng/mL (date________)<br />
Tacrolimus concentration __________ng/mL (date________)<br />
a) biopsy-proven severe nephrotoxicity. Increase in serum creatinine must be 50% above baseline.<br />
Biopsy result ____________________________________(date_________)<br />
Baseline serum creatinine ____________________µmol/L (date_________)<br />
Current serum creatinine ____________________µmol/L (date_________)<br />
b) Neurotoxicity (describe reaction) ______________________________________ (date______)<br />
2. Patient has developed calcineurin inhibitor intolerance: hypersensitivity reaction or microangiopathy<br />
Cyclosporine (date_________) Tacrolimus (date______)<br />
3. Recurrent (≥ 2) biopsy-proven, acute rejection, while on calcineurin inhibitors despite blood<br />
concentrations within the therapeutic range.<br />
Biopsy result: ___________________________ (date_______)<br />
Biopsy result: ___________________________ (date________)<br />
Cyclosporine concentration: _________________mol/L (date_________)<br />
Tacrolimus concentration: _________________mol/L (date_________)<br />
<strong>4.</strong> Maintenance immunosuppression following steroid-resistant rejection. ATG use __________(date)<br />
5. Renal dysfunction due to: hepato-renal syndrome or post transplant acute tubular necrosis<br />
6. Acute rejection not requiring ATG, but sirolimus is necessary <strong>for</strong> maintenance<br />
immunosuppression.<br />
Physician’s Signature: __________________________ Date: ____________<br />
Approval by BCT: _____________________________ Date: ____________<br />
FEB/2010<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 47<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix G<br />
VANCOUVER HOSPITAL & HEALTH SCIENCES CENTER<br />
DOCTOR’S ORDERS<br />
STANDING LAB ORDERS FOR LIVER TRANSPLANT PROGRAM<br />
Date:<br />
Full BLOOD WORK<br />
CBC with differential<br />
PTT, INR<br />
Na, K, C1, PO4, Mg, Ca, CO 2<br />
BUN, Cr, Glucose (random), uric acid,<br />
Total/direct bilirubin, Alk. phosphatase, GGT, AST, ALT<br />
Amylase, albumin, total protein<br />
Cyclosporine level, Sirolimus level or FK506 (Tacrolimus) level<br />
Mini BLOOD WORK<br />
CBC with differential<br />
PTT, INR<br />
K, BUN, Cr,<br />
Total/direct bilirubin, Alk. phosphatase, GGT, AST, ALT<br />
Cyclosporine level, Sirolimus level or FK506 (Tacrolimus) level<br />
ANNUAL BLOOD WORK<br />
Same as full blood work plus the following tests:<br />
HgAIC:<br />
Done at 3 months post transplant.<br />
If the values are abnormal and/or diabetic patient, repeat q 3 months and consult doctor.<br />
If the values are normal, then annually thereafter.<br />
Lipid studies: (Cholesterol, triglycerides, HDL, LDL):<br />
Done at 6 months and annually thereafter.<br />
If the values are elevated, follow level and consult doctor.<br />
Hepatitis Screening:<br />
Done at 1 year post-transplant and as ordered thereafter.<br />
Hepatitis B positive patient/or donor: HBV DNA, HCV Ab<br />
*HBV DNA annually thereafter.<br />
Hepatitis C positive patient: HBsAg, HBc Ab(total)<br />
Non Hep B & Hep C: HBsAg, HBc Ab(total), HCV Ab<br />
AFP test: Every 4 months x 3 years and annually thereafter on patient who has any one of the<br />
following conditions: Hep B, Hep C and/or malignancy.<br />
CA19to9: Every 4 months x 3 years and annually thereafter on patient who has gallbladder<br />
malignancy.<br />
Abdominal ultrasound with Doppler<br />
____________________<br />
Physician Signature<br />
________________________________<br />
Printed Name/PIC<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 48<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix H<br />
PROTOCOL FOR HEPATITIS B LIVER TRANSPLANT RECIPIENTS<br />
Protocol:<br />
1) Lamivudine 100 mg PO daily and<br />
2) HBIG<br />
{HBIG is available as:<br />
Bay-Hep ® 5ml (1085 units) given IM<br />
- must only be given IM (no IV administration)<br />
A. Induction phase (Intra-operatively)<br />
Bay-Hep ® 10ml (2170IU) IM as 5ml into each deltoid muscle<br />
B. HBIG protocol <strong>for</strong> week 1 to week 52:<br />
1. Post-transplant Week 1 to 6: Bay-Hep ® 10ml (2170IU) IM as 5ml into each gluteal muscle until Hep<br />
B titer is > 1000 U/L. Then, Bay-Hep ® 10ML IM (as 5ml into each gluteal/deltoid muscle) Twice<br />
weekly (Q Mon, Thurs) <strong>for</strong> 6 weeks (maintain trough Hep B titer > 500 U/L).<br />
2. Post-transplant weeks 7 to 10: if Hep B titer is > 500 U/L, then give Bay-Hep ® 10ml IM (as 5ml<br />
into each gluteal muscle) weekly.<br />
3. Post-transplant weeks 11 to 24: give Bay-Hep ® 10ml every 2 to 4 weeks to maintain Hep B titer<br />
> 500 IU/L<br />
<strong>4.</strong> Post-transplant week 25 to 52: give Bay-Hep ® 10ml every 4 weeks to maintain Hep B titer ><br />
250 IU/L<br />
C. HBIG protocol <strong>for</strong> > 1 year post-transplant:<br />
Dose: BaytoHep ® 10ml IM. (as 5ml into each gluteal muscle)<br />
Patient to get Hep B AB titer done in the local lab 4 weeks after each injection. The results will be sent<br />
to outpatient liver transplant clinic.<br />
Then, the frequency of administration of HBIG will be adjusted based on Hep B Ab titer according to<br />
the following table<br />
Hep B Ab titer (IU/L)<br />
Action<br />
> 300 Level in 2 weeks<br />
200 to 300 Injection in 3 weeks*<br />
150 to 200 Injection in 2 weeks*<br />
100 to 150 Injection in 1 week*<br />
< 100 Injection ASAP*<br />
* Please obtain Hep B titer be<strong>for</strong>e each injection<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 49<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
CMV PROPHYLAXIS AND TREATMENT REGIMENS FOR LIVER TRANSPLANT RECIPIENTS Appendix I<br />
CMV STATUS<br />
THERAPY<br />
DONOR RECIPIENT PROPHYLAXIS PRE-EMPTIVE TREATMENT DISEASE TREATMENT<br />
Negative Negative No prophylactic Valganciclovir<br />
If CMV PCR > 1000 cp/mL follow treatment protocol<br />
CMV PCR testing with bloodwork (maximum q weekly) <strong>for</strong><br />
4 months post-transplant and <strong>for</strong> 2 months following any<br />
antiviral treatment.<br />
Asymptomatic:<br />
Valganciclovir 900 mg PO bid adjusted <strong>for</strong> renal function<br />
<strong>for</strong> 2 weeks followed by 900 mg PO daily <strong>for</strong> 4 months.<br />
Symptomatic:<br />
Ganciclovir 5 mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function x 2 weeks followed by Valganciclovir 900 mg PO<br />
daily adjusted <strong>for</strong> renal function <strong>for</strong> 4 months.<br />
Positive<br />
(Mismatch)<br />
Negative<br />
Ganciclovir 5mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function x 14 days or until hospital discharge, then<br />
Valganciclovir 900 mg PO daily adjusted <strong>for</strong> renal<br />
function until 4 months post transplant.<br />
During Lymphocyte Depleting Therapies:<br />
Ganciclovir 5 mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function or Valganciclovir 900mg PO daily adjusted <strong>for</strong><br />
renal function <strong>for</strong> 2 months.<br />
If CMV PCR > 1000 cp/mL and patient is asymptomatic<br />
then:<br />
Valganciclovir 900 mg PO daily adjusted <strong>for</strong> renal<br />
function until CMV PCR test is < 1000 cp/mL <strong>for</strong> 2<br />
consecutive weeks and patient is clinically stable<br />
(minimum 1 month therapy)<br />
Increase Valganciclovir dose to 900 mg PO bid<br />
adjusted <strong>for</strong> renal function if CMV PCR is rising<br />
Ganciclovir 5 mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function x 2 weeks followed by Valganciclovir 900 mg<br />
PO daily adjusted <strong>for</strong> renal function <strong>for</strong> 4 months.<br />
If no diarrhea, consider:<br />
Valganciclovir 900 mg PO bid adjusted <strong>for</strong> renal function<br />
x 2 weeks followed by Valganciclovir 900 mg PO daily<br />
adjusted <strong>for</strong> renal function <strong>for</strong> 4 months.<br />
Positive OR<br />
Negative<br />
Positive<br />
CMV PCR testing with bloodwork (maximum q weekly) <strong>for</strong><br />
6 months post-transplant and <strong>for</strong> 2 months following any<br />
antiviral treatment.<br />
No prophylactic Valganciclovir<br />
During Lymphocyte Depleting Therapies<br />
Ganciclovir 5 mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function or Valganciclovir 900 mg PO daily adjusted <strong>for</strong><br />
renal function <strong>for</strong> 2 months.<br />
CMV PCR testing with bloodwork (maximum q weekly) <strong>for</strong><br />
4 months post-transplant and <strong>for</strong> 2 months following any<br />
antiviral treatment.<br />
If CMV PCR > 5000 cp/mL and patient is asymptomatic<br />
then:<br />
Valganciclovir 900 mg PO daily adjusted <strong>for</strong> renal<br />
function until CMV PCR test is < 2000 cp/mL and<br />
decreasing <strong>for</strong> 2 consecutive weeks and patient is<br />
clinically stable (minimum 1 month therapy).<br />
Increase Valganciclovir dose to 900 mg PO bid<br />
adjusted <strong>for</strong> renal function if CMV PCR is rising.<br />
Ganciclovir 5 mg/kg/dose q 12h IV adjusted <strong>for</strong> renal<br />
function x 2 weeks followed by Valganciclovir 900 mg<br />
PO daily adjusted <strong>for</strong> renal function <strong>for</strong> at least 2 weeks<br />
(CMV PCR test should be < 2000 cp/mL and decreasing<br />
<strong>for</strong> 2 consecutive weeks and patient clinically stable prior<br />
to discontinuation of Valganciclovir).<br />
If no diarrhea, consider:<br />
Valganciclovir 900 mg PO bid adjusted <strong>for</strong> renal function<br />
x 2 weeks followed by Valganciclovir 900 mg PO daily<br />
adjusted <strong>for</strong> renal function <strong>for</strong> at least 2 weeks (CMV PCR<br />
test should be < 2000 cp/mL and decreasing <strong>for</strong> 2<br />
consecutive weeks and patient clinically stable prior to<br />
discontinuation of Valganciclovir).<br />
Hepatitis C positive recipient (donor or recipient CMV +) Follow mismatch protocol<br />
Oral Valganciclovir tablets are supplied free of charge through the BCT Pharmacy Program <strong>for</strong> outpatients on the above protocol.<br />
If total WBC is less than 2.5 x 10 9 /L decrease Valganciclovir dose to 450 mg PO daily.<br />
If total WBC is less than 1.5 x 10 9 /L hold Valganciclovir until WBC is greater than 3.5 x 10 9 /L, then restart Valganciclovir at 450 mg PO daily. December 11, 2008<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 50<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Valganciclovir and Ganciclovir Dose<br />
Appendix I (con't)<br />
The Valganciclovir dose depends on patient’s renal function, white blood cell count and whether or<br />
not the patient is receiving Valganciclovir <strong>for</strong> CMV prophylaxis, pre-emptive treatment or disease<br />
treatment. Refer to the tables of Valganciclovir dosing with impaired renal function and CMV<br />
prophylaxis and treatment protocols <strong>for</strong> renal, liver and lung recipients on the following pages.<br />
Valganciclovir is administered with food.<br />
Ganciclovir IV Dose <strong>for</strong> Adult Patients with Impaired Renal Function (6)<br />
Creatinine Clearance<br />
(mL/min)<br />
Greater and equal to 70<br />
Ganciclovir IV Dose<br />
(mg/kg)<br />
5 mg/kg/dose q 12h<br />
50 to 69 5 mg/kg/dose q 24h or 2.5 m/kg/dose q 12h<br />
25 to 49 2.5 mg/kg/dose q 24h<br />
10 to 24 1.25 mg/kg/dose q 24h<br />
Less than 10<br />
1.25 mg/kg/dose 3 times weekly post dialysis<br />
Valganciclovir Oral TABLET Dose <strong>for</strong> Adult Patients with Impaired Renal Function (7)<br />
Creatinine Clearance (mL/min) Valganciclovir TABLETS PO Dose<br />
Greater and equal to 60<br />
900 mg PO daily<br />
40 to 59 450 mg PO daily<br />
25 to 39 450 mg PO every 2 days<br />
10 to 24 450 mg PO twice weekly<br />
Valganciclovir Oral SOLUTION Dose <strong>for</strong> Adult Patients with<br />
Impaired Renal Function (7)<br />
Creatinine Clearance (mL/min)<br />
Greater and equal to 60<br />
Valganciclovir SOLUTION PO Dose<br />
900 mg PO daily<br />
40 to 59 450 mg PO daily<br />
25 to 39 225 mg PO daily<br />
10 to 24 125 mg PO daily<br />
Less than 10<br />
100 mg PO three times a week post dialysis<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 51<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix I (con’t)<br />
Valganciclovir Oral Dose <strong>for</strong> Pediatric Patients with Impaired Renal Function (8)<br />
Creatinine<br />
Clearance<br />
(mL/min/1.73 m 2 )<br />
Patient Weight<br />
< 30 kg<br />
Greater and equal to 10 to 12 mg/kg PO<br />
60<br />
daily<br />
40 to 59 5 to 6 mg/kg PO<br />
daily<br />
25 to 39 5 to 6 mg/kg PO<br />
every other day<br />
10 to 24 5 to 6 mg/kg PO<br />
2 times/week<br />
Valganciclovir Oral Dose<br />
Patient Weight<br />
30 to 50 kg<br />
Patient Weight<br />
greater and equal<br />
to 50 kg<br />
450 mg PO daily 900 mg PO daily<br />
225 mg PO daily 450 mg PO daily<br />
225 mg PO every<br />
other day<br />
225 mg PO<br />
2 times/week<br />
450 mg PO every<br />
other day<br />
450 mg PO<br />
2 times/week<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 52<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix I (con't)<br />
References<br />
For CMV Prophylaxis and Treatment and Dental Prophylaxis<br />
1. Wilson W, Taubert KA, Gewitz M et al. Prevention of infective endocarditis. <strong>Guidelines</strong> from<br />
The American Heart Association. Circulation 2007; 116:1736-1754<br />
2. Asberg A, Humar A, Rollag H et al. Oral valganciclovir is noninferior to intravenous<br />
ganciclovir <strong>for</strong> treatment of cytomegalovirus disease in solid organ transplant recipients. American<br />
Journal of <strong>Transplantation</strong> 2007:7; 2106-2113.<br />
3. Khoury JA, Storch GA, Bohl DL et al. Prophylactic versus preemptive oral valganciclovir <strong>for</strong><br />
the management of cytomegalovirus infection in adult renal transplant recipients. American<br />
Journal of <strong>Transplantation</strong> 2006:6; 2134-2143.<br />
<strong>4.</strong> Preiksaitis JK, Brennan DC, Fishman J et al. Canadian society of transplantation consensus<br />
workshop on cytomegalovirus management in solid organ transplantation final report. American<br />
Journal of <strong>Transplantation</strong>. 2005:5; 218-227.<br />
5. Reischig T. Jindra P. Hes O. Svecova M. Klaboch J. Treska V. Valacyclovir prophylaxis versus<br />
preemptive valganciclovir therapy to prevent cytomegalovirus disease after renal transplantation.<br />
American Journal of <strong>Transplantation</strong>. 2008: 8; 69-77.<br />
6. Kliem V, Fricke L, Wollbrink T et al. Improvement in long-term renal graft survival due to<br />
CMV prophylaxis with oral ganciclovir: results of a randomized clinical trial. American Journal of<br />
<strong>Transplantation</strong> 2008:8; 975-983.<br />
7. Cytovene® Product Monograph, Hoffman La Roche Ltd, Canada, revised May 29, 2009<br />
8. Valcyte® Monograph Roche Hoffman La Roche Ltd, revised March 5, 2008<br />
9. BCCH Transplant –Sirolimus Study SN-01, Children and Women’s Hospital. 2007<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 53<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix J<br />
TREATMENT FOR OTHER OPPORTUNISTIC INFECTIONS IN<br />
LIVER TRANSPLANT RECIPIENTS<br />
Organism Site of Infection Drug of Choice<br />
Herpes Simplex Virus (HSV)<br />
Mucocutaneous<br />
to mild<br />
Acyclovir 800 mg PO qid <strong>for</strong> 7 days<br />
OR<br />
Valacyclovir 1000 mg PO tid <strong>for</strong> 7 to 10 days<br />
Varicella-Zoster Virus (VZV)<br />
Pneumocytis Carinii Pneumonia<br />
to severe<br />
Respiratory<br />
Encephalitis<br />
Mild<br />
Severe<br />
Prophylaxis<br />
Treatment<br />
Acyclovir 5 mg/kg IV q 8h <strong>for</strong> 7 days<br />
Acyclovir 10 mg/kg IV q 8h <strong>for</strong> 10 days<br />
Acyclovir 10 mg/kg IV q 8h <strong>for</strong> 10 days<br />
Acyclovir 800 mg PO <strong>for</strong> 4 to 5x daily <strong>for</strong> 7 to 10<br />
days OR<br />
Valacyclovir 1g to tid x 7 to 10 days<br />
Acyclovir 10 to 12 mg/kg IV q 8h <strong>for</strong> 7 to 14 days<br />
None<br />
TMP-SMX 5 mg/kg IV (based on TMP<br />
component) q 6h <strong>for</strong> 21 days<br />
Sulfa allergy: Pentamidine IV 4mg/kg/daily <strong>for</strong> 21<br />
days<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 54<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
AUTHORIZATION FOR RELEASE OF INFORMATION<br />
Re: ____________________________________________________________<br />
(Name of Patient-Print in Full)<br />
(Date of Birth)<br />
Address of Patient: ______________________________________________________<br />
I, _____________________________________________, do hereby authorize you to<br />
permit __________________________________to release the following in<strong>for</strong>mation:<br />
(Name of institution)<br />
Appendix K<br />
(Note approximate dates in hospital and indicate what specific in<strong>for</strong>mation the records are required)<br />
_______________________________________________________________________<br />
_______________________________________________________________________<br />
to, BC Transplant:<br />
I consent to the use of this in<strong>for</strong>mation by the authorized recipient only <strong>for</strong> the purposes of:<br />
____________________________________________________________<br />
I am nineteen years of age or older.<br />
Dated this _______________________________day of__________________, 20____<br />
Signature: _______________________ Witness: _______________________<br />
(Patient)<br />
(Signature of Witness)<br />
_______________________<br />
(Print Name of Patient)<br />
________________________<br />
(Print Name of Witness)<br />
_______________________<br />
(Parent or Guardian)<br />
Address of witness if not an employee of BC Transplant:<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
Relationship to Patient: __________________________________________________<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 55<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix L<br />
CONSENT TO DIAGNOSIS, TREATMENT AND CARE<br />
I, the undersigned, do hereby authorize the physician and employees of BC Transplant (and persons<br />
authorized by such other institutions as may be requested by BC Transplant) to carry out examinations,<br />
procedures and treatment deemed necessary and advisable <strong>for</strong> the evaluation, diagnosis, treatment and<br />
continuing care. I, hereby authorize the release of follow-up in<strong>for</strong>mation pertaining to my condition and/or<br />
status (including medical diagnosis and relevant dates).<br />
Program: ________________________________________<br />
Registration Date: _________________________________<br />
Name: (Mr., Mrs., Ms.) __________________________________________________________________<br />
SURNAME<br />
GIVEN NAMES<br />
Date of Birth: _____________________________________________Sex:__________________________<br />
MONTH DAY YEAR<br />
Address: ______________________________________________________________________________<br />
NUMBER<br />
STREET<br />
Address:_______________________________________________________________________________<br />
CITY<br />
PROVINCE<br />
Address: ____________________________<br />
POSTAL CODE<br />
Telephone Number (home): (________)__________________ PHN:_____________________________<br />
SIGNATURE:_________________________________<br />
(PATIENT OR GUARDIAN)<br />
WITNESS:____________________________________<br />
(SIGN)<br />
_____________________________________<br />
(PRINT NAME IF NOT THE PATIENT)<br />
_____________________________________<br />
(PRINT NAME)<br />
DATE: ___________________________________<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 56<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix M<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 57<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix M con’t.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 58<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Recipient Activation Form<br />
BCT #: Activation Date:<br />
Appendix N<br />
dd/mmm/yyyy<br />
Program:<br />
Pancreas<br />
<strong>Liver</strong><br />
Heart<br />
Heart/Lung<br />
Single Lung<br />
Double Lung<br />
Other: _________________<br />
Tx Centre:<br />
Tx No.: Date of Previous Tx: Previous Tx Prg:<br />
VGH<br />
SPH<br />
CHH<br />
Patient Name:<br />
Date of Birth:<br />
Pager #:<br />
Home Phone#:<br />
Work Phone #: Cell #:<br />
Contact Name 1: Phone #:<br />
Contact Name 2: Phone #:<br />
Specialist: Phone #:<br />
Family Physician: Phone #:<br />
Activation Status:<br />
Previous CT Surgery:<br />
ABO:__________ Rh: ____________ Height (cm): ________ Weight(kg): __________<br />
Cytotoxicity (PRA): Current: _____________ Date: _______________<br />
Viral Screen: CMV: ______ CMV Tested Date:___________ HCV: ______ HIV: ________ EBV: _______<br />
HbsAg(HBV):______ HBV Date Tested: _________ HbsAB: ____ HbcAB (Total): ________<br />
VZV:____________ RPR: ____________ HBV DNA:_____ HSV:______<br />
Comments:<br />
Ascites:<br />
No Small Moderate Large Unknown<br />
HCV Genotype: ___________ PVR: _____________ X-Match:_________________<br />
HCV Genotype Sub-Category: ____<br />
TLC (Actual): __________ TLC (Predicted): ____________<br />
Completed By:<br />
Entered into PROMIS By:<br />
Date:<br />
Date:<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 59<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix O<br />
CONTRACT FOR ABSTINENCE<br />
The policy of BC Transplant is that no patient with an ongoing substance abuse problem be accepted<br />
<strong>for</strong> liver transplantation. In order to be considered a possible liver transplant candidate, patients with<br />
a history of alcohol or drug abuse will have to demonstrate at least six continuous months of<br />
abstinence.<br />
In order to do everything to ensure a successful outcome to transplantation,<br />
I, _________________________________________, AGREE TO COMPLETELY ABSTAIN FROM ALCOHOL,<br />
ILLICIT DRUGS AND OTHER ABUSABLE SUBSTANCES FOR THE REST OF MY LIFE. In addition, I will refrain<br />
from abusing any prescription medications.<br />
I may also be required to avail myself of the services of an alcohol and drug (A&D) treatment program to<br />
help ensure relapse prevention and I will adhere to the recommendations of the A&D counsellor. In addition,<br />
I will allow random testing of my blood, breath and urine as evidence of my abstinence.<br />
I give permission to have family members, significant others and relevant health care providers be contacted<br />
to help verify my continuing abstinence and <strong>for</strong> purposes of ongoing transplant assessment.<br />
Following completion of the initial required period of abstinence, I will be re-assessed by the Transplant<br />
Team to determine my status regarding transplantation. I UNDERSTAND THAT VIOLATING THIS AGREEMENT<br />
WILL RESULT IN MY FORFEITING MY TRANSPLANT CANDIDACY STATUS.<br />
I further understand that lifelong abstinence from all abusable substances is an important part of my<br />
ability to maintain my health and the health of the transplanted liver following surgery.<br />
Resuming substance use any time following acceptance into the transplant program will result in my<br />
being removed from the transplant waiting list.<br />
If I relapse after surgery, I agree to enter a substance abuse program chosen <strong>for</strong> me by the Transplant Team. I<br />
ALSO UNDERSTAND THAT IF I RELAPSE TO SUBSTANCE USE FOLLOWING TRANSPLANTATION, I WILL NOT<br />
BE OFFERED A SECOND TRANSPLANT SHOULD ONE BECOME NECESSARY.<br />
I have read the above and agree to the conditions set <strong>for</strong>th and I have a copy of this contract <strong>for</strong> my records.<br />
____________________________________<br />
Patient Signature<br />
__________________________________<br />
Signature of Witness<br />
____________________________________<br />
Date and Place<br />
___________________________________<br />
Print Name and Relationship to Patient<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 60<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
<strong>Liver</strong> Transplant Baseline Assessment<br />
Appendix P<br />
Pt. Name<br />
Blood Type:_______________________<br />
Hematology:<br />
WBC:_____________________________<br />
Hgb:______________________________<br />
MCV:_____________________________<br />
Platelet :___________________________<br />
INR:______________________________<br />
PTT:______________________________<br />
Chemistry:<br />
Na:_______________________________<br />
K:________________________________<br />
CL:_______________________________<br />
CO2:_____________________________<br />
Urea:_____________________________<br />
Creatinine:_________________________<br />
Est GFR:___________________________<br />
Calcium:___________________________<br />
Phosphate:________________________<br />
AlkPhos:__________________________<br />
GGT:_____________________________<br />
CK:_______________________________<br />
AST:______________________________<br />
ALT:______________________________<br />
Total Bili:__________________________<br />
Direct Bili:_________________________<br />
Protein:___________________________<br />
Albumin:___________________________<br />
Glucose:__________________________<br />
Other Results:<br />
AFP:______________________________<br />
CEA:_____________________________<br />
PSA:_____________________________<br />
Urinalysis:_________________________<br />
Stools <strong>for</strong> OB: #1_____#2_____#3_____<br />
TB Skin Test:_______________________<br />
Diagnostic:<br />
Antinuclear Ab:_____________________<br />
Antismooth muscle Ab:_______________<br />
Antimitochondial Ab:_________________<br />
Alpha 1 Antitrypsin level:______________<br />
Ceruloplasmin:_____________________<br />
Ferritin:____________ Iron:___________<br />
TIBC:______Fraction Saturation:_______<br />
Genetic Testing: ____________________<br />
Date of Blood work:<br />
Virology:<br />
DATE<br />
CMV IgG<br />
EBV IgG<br />
HepA Total<br />
HbsAg<br />
HbsAb<br />
HbcAB<br />
HbVDNA<br />
Hep C<br />
Genotpye<br />
HSV<br />
VZV<br />
HIV I &II<br />
Ancillary Testing:<br />
CXR:__________________________________<br />
EKG:__________________________________<br />
ECHO:_________________________________<br />
US:____________________________________<br />
CT:____________________________________<br />
MRI:___________________________________<br />
Mammogram:____________________________<br />
Dental:_________________________________<br />
Anesthesia:______________________________<br />
Tumor Rounds:__________________________<br />
Tumor Treatment:________________________<br />
MISC. Consults:_________________________<br />
_______________________________________<br />
_______________________________________<br />
Team Consults:<br />
Social Work:_____________________________<br />
Psychologist:_____________________________<br />
Nutritionist:______________________________<br />
Pre-Activation Talk:_______________________<br />
Ascites:_____________HE:____________<br />
MELD:____________PUGH:___________<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 61<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix Q<br />
WHEN A LIVER BECOMES AVAILABLE<br />
Keep your pager with you at all times and call the <strong>Clinical</strong> Coordinator on call 24 hours a day at<br />
1-800-663-6189 or (604) 877-2240 anytime your pager goes off.<br />
It is extremely important that the transplant team be able to reach you as soon as a liver becomes available.<br />
The transplant team should know where to get in touch with you at all times.<br />
If an organ becomes available and the transplant team has selected you as the most suitable recipient, the BCT<br />
Transplant Coordinator will attempt to contact you by first phoning your home telephone number. If there is<br />
no response, they will attempt paging you via your pager. Even though a donor liver receives special<br />
handling and will be stored in a special solution to keep it suitable <strong>for</strong> transplantation, there is a time limit.<br />
It is very important that if your telephone number changes, you should immediately in<strong>for</strong>m the BCT <strong>Liver</strong><br />
Transplant Coordinator.<br />
You may also want to get a telephone answering machine and check it often. If you plan on going out of<br />
town, be sure to leave your travel plans and contact numbers with the transplant coordinator.<br />
When you do get the call from your Transplant Centre, you will probably feel equal levels of excitement and<br />
fear. It will seem as if everything is a blur. This is why it is very important <strong>for</strong> you to make any plans in<br />
advance, whenever possible.<br />
Make sure you do not eat or drink anything once you have been called to the hospital. It is important that<br />
your stomach be empty in order to have surgery.<br />
If you are waiting at home, the call to come into hospital <strong>for</strong> transplant may come at any time of the day or<br />
night. The Transplant Coordinator will identify themselves and ask you a few questions. They will ask:<br />
How you are feeling<br />
If you have any colds or fever<br />
If you have a sore throat or diarrhea<br />
If you have had any recent infections<br />
If you are taking any antibiotics<br />
If they have no concerns regarding your present condition they will ask you to come to the hospital as soon as<br />
possible. If you live in the Lower Mainland/Vancouver area, it is expected that will arrive at the hospital<br />
within 2 hours of the telephone call. If you are coming by car, please ensure that you have someone drive<br />
you. If you are coming from outside of the lower Mainland, the Transplant Coordinator will give you detailed<br />
instructions regarding the transportation plan. You will either come by air ambulance, commercial flight, or<br />
charter flight. The Transplant Coordinator will make the travel arrangements.<br />
If you are coming by commercial flight or charter flight, you will need money <strong>for</strong> a taxi from the airport to<br />
Vancouver General Hospital (around $20.00). BC Transplant will cover the cost of commercial flight or<br />
charter flight. If you come by air ambulance, you can be billed up to $240.00 depending on where you live.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 62<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix Q (con’t)<br />
Once you have been admitted to hospital you will be prepared <strong>for</strong> surgery on the Transplant Unit.<br />
Once admitted, you can expect:<br />
<br />
<br />
<br />
<br />
<br />
<br />
Not to eat or drink anything<br />
To have blood work drawn<br />
To have an intravenous (IV) started<br />
To be asked <strong>for</strong> a urine specimen<br />
To have a chest x-ray and ECG<br />
To have your bowels cleared/prepped<br />
WHAT SHOULD I BRING TO THE HOSPITAL?<br />
<br />
<br />
Your Care Card/PHN number<br />
An accurate list of all medications (names, doses, frequency) that you take, or bring the<br />
medications with you.<br />
After your surgery, once you are transferred to the Transplant Unit, your family can bring:<br />
1. The “Living With <strong>Transplantation</strong> Manual”<br />
2. A credit card which you can use to pay <strong>for</strong> a television<br />
3. Any walking aid or cane you may be using<br />
<strong>4.</strong> Small change to cover the cost of newspaper, coffee shop, pay phone etc.<br />
5. A small overnight bag<br />
6. All needed toiletry items: soap, shampoo, comb/brush, toothbrush etc.<br />
7. Lip and skin moisturizer (the air in hospital tends to be very dry)<br />
8. Mouthwash (if you use it on a regular basis)<br />
9. Bathrobe which opens all the way down the front<br />
10. Slippers with closed-in heel and rubber soles, or running shoes.<br />
11. A good book or magazine<br />
12. BRING YOUR PAGER with you to return to the BCT after your transplant.<br />
Do NOT Bring<br />
<br />
<br />
<br />
<br />
Any valuables such as rings, watches or jewellery<br />
A large amount of cash (a maximum of $20.00 may be locked up on the ward.)<br />
Any large electrical equipment, which needs to be plugged in (you may bring an electrical<br />
razor or hair dryer or a small portable radio)<br />
A cellular phone (you cannot use this in the hospital)<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 63<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
VGH Transplant Checklist-<strong>Liver</strong>, Kidney, P/K<br />
Appendix R<br />
Patient<br />
Name<br />
DOB<br />
PHN<br />
CMV<br />
ABO<br />
Chart to ward<br />
Patrick Helton<br />
604-715-6693(24hr)<br />
250-629-3257<br />
604-270-6101<br />
EHS<br />
1-800-561-8011<br />
872-5151 L.Mainland<br />
Date:________________; CC Start time:___________Finish time:___________<br />
Donor Info: ABO _____; CMV _____; Retrieval Time _____<br />
<strong>Liver</strong> P/K Kidney 1 Kidney 2<br />
On call Nephrologist<br />
to contact patient<br />
N/A<br />
On call Nephrologist<br />
to contact patient<br />
ETA to hosp N/A N/A<br />
Emerg Admit<br />
Nephrologist to call Nephrologist to call<br />
875-4311<br />
VGH access director: P.<br />
675to6056 (local 55145)<br />
Any Infection<br />
Precautions? VRE, MRSA<br />
In<strong>for</strong>m Admitting, ward,<br />
OR, ICU<br />
T4D 875-4822<br />
Extrarenal: 2ACD,1 clot<br />
Nephrologist to call<br />
ICU 875-4275 N/A N/A N/A<br />
OR 875-4472 N/A N/A<br />
Recip. OR start time N/A N/A<br />
Blood Bank<br />
875-4420 (tell if HepB)<br />
Emerg. X-Ray<br />
875-5555 Local 62520<br />
<strong>Clinical</strong> Trials<br />
<strong>Liver</strong> Tx. Dr. on-call:<br />
Yoshida 875-5371 (O)<br />
872-9858 (P)<br />
Steinbrecher<br />
220-3273 (BB)<br />
Erb<br />
875-5039 (O)<br />
875-5618 (O)<br />
707-1397 (P)<br />
574-6360 (H)<br />
N/A<br />
N/A<br />
N/A<br />
Nephrologist to call<br />
N/A<br />
N/A<br />
N/A N/A N/A<br />
Program Coordinators Each program to notify Allied staff, Specialists & GP<br />
Linda Leung lleung4@bcts.hnet.bc.ca 604-877-2182<br />
Andrea<br />
aoshaughnessy@bcts.hnet.bc.ca 604-877-2134<br />
O’Shaughnessy<br />
Jan Emerton Jan_emerton@bcts.hnet.bc.ca 604-877-2120<br />
Wynne Chiu wchiu@providencehealth.ca 604-806-8887<br />
Sharon Duncan sharon_duncan@bcts.hnet.bc.ca 604-877-2110<br />
Reminders: Notify Transplant surgeon, retrieval, transplant physician, T4D if patient<br />
delayed.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 64<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
AMBULATORY DEPARTMENT<br />
BC Transplant (BCT)<br />
3 rd Floor, West Tower, 555 West 12th Ave.<br />
Vancouver, BC<br />
CANADA V5Z 3X7<br />
Telephone (604) 877-2240<br />
Toll Free 1-800-663-6189<br />
FAX (604) 604-877-2111<br />
Appendix S<br />
FAX COVERSHEET<br />
REQUIRED MEDICAL FOLLOW-UP<br />
FOR TRANSPLANT RECIPIENT(S)<br />
FROM:_____________________________<br />
Date:___________________<br />
Number of Pages _________________ [Attach copy of Exceptional Distribution]<br />
(including this page)<br />
SPH Heart Clinic Fax: 604-806-8763 Attention:<br />
SPH Kidney Clinic Fax: 604-806-8076 Attention:<br />
BCCH Fax: 604-875-2943 Attention:<br />
VGH SOT Clinic Fax: 604-875-4088 Attention:<br />
OTHER Fax: Attention:<br />
Please note that the organ recipient listed below requires Medical follow-up as<br />
a result of Exceptional Distribution of Organs:<br />
Date of Transplant:__________________________<br />
Name of Recipient: ________________________Organ transplanted:______________<br />
A copy of the Exceptional Distribution is attached.<br />
PLEASE INFORM THE RECIPIENT'S MEDICAL PHYSICIAN IMMEDIATELY.<br />
If further in<strong>for</strong>mation is required, please do not hesitate to contact our<br />
department.<br />
_____________________________________________________________________________________________________<br />
Notice of Confidentiality<br />
This communication is intended <strong>for</strong> the individual or institution to which it is addressed. It may not be distributed, <strong>for</strong>warded, or disclosed to<br />
other unauthorized persons. It may contain confidential or personal in<strong>for</strong>mation subject to the Freedom of In<strong>for</strong>mation and Protection of<br />
Privacy Act and the Personal In<strong>for</strong>mation Protection and Electronic Documents Act. If you receive this communication in error, please notify<br />
the sender immediately and destroy the communication, thank you.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 65<br />
See Page 1 <strong>for</strong> disclaimer
Guidebook <strong>for</strong> the Solid Organ Transplant Programme Chapter 4<br />
Appendix S (con’t)<br />
Recommended Follow-up Testing <strong>for</strong> Recipients Transplanted under Risk <strong>for</strong> Viral<br />
Mediated Disease Transmission<br />
NOTICE TO TRANSPLANT RECIPIENT MEDICAL TEAM:<br />
The following protocol has been approved by the BC Transplant Medical Advisory Committee<br />
(MAC) as a course of action <strong>for</strong> follow-up of recipients transplanted at risk <strong>for</strong> HIV and/or Hepatitis:<br />
IT IS RECOMMENDED THAT RECIPIENTS ARE RETESTED FOR HIV, HEPATITIS B AND<br />
HEPATITIS C at:<br />
• 4 weeks<br />
• 8 weeks<br />
• 6 months<br />
• 1 year<br />
Recommended Test Methods**:<br />
HIV - Conventional antibody testing<br />
HBV - HBsAg and HBcIgM<br />
HCV - Conventional antibody testing<br />
**NOTE: If there is clinical or epidemiological evidence to suggest a patient may have become<br />
infected with any of these viruses and antibody tests are negative, then PCR testing should be<br />
discussed with the medical team.<br />
Chapter 4 – <strong>Clinical</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Liver</strong> <strong>Transplantation</strong> – July, 2010 Page 66<br />
See Page 1 <strong>for</strong> disclaimer