

Download
Download
Download

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Assessment and Management of Venous Leg Ulcers<br />
The literature also stresses the importance of clear and comprehensive documentation of<br />
information during history taking, and suggests several examples of leg ulcer assessment<br />
forms. The RNAO guideline development panel does not consider one assessment form to<br />
be superior to another. (For examples of leg ulcer assessment forms, see Appendices D and E).<br />
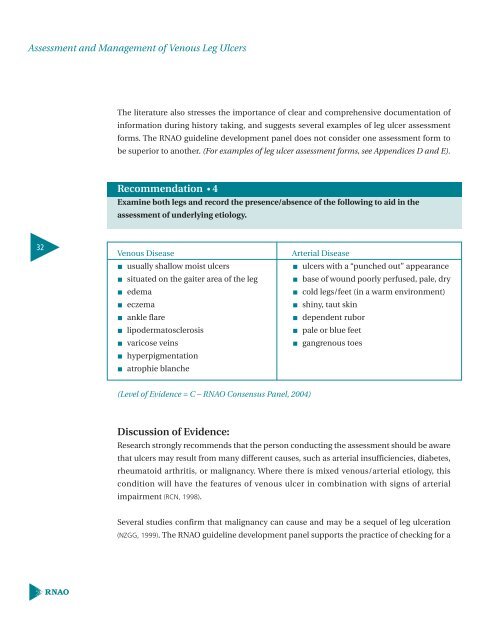
Recommendation • 4<br />
Examine both legs and record the presence/absence of the following to aid in the<br />
assessment of underlying etiology.<br />
32<br />
Venous Disease<br />
usually shallow moist ulcers<br />
situated on the gaiter area of the leg<br />
edema<br />
eczema<br />
ankle flare<br />
lipodermatosclerosis<br />
varicose veins<br />
hyperpigmentation<br />
atrophie blanche<br />
Arterial Disease<br />
ulcers with a “punched out” appearance<br />
base of wound poorly perfused, pale, dry<br />
cold legs/feet (in a warm environment)<br />
shiny, taut skin<br />
dependent rubor<br />
pale or blue feet<br />
gangrenous toes<br />
(Level of Evidence = C – RNAO Consensus Panel, 2004)<br />
Discussion of Evidence:<br />
Research strongly recommends that the person conducting the assessment should be aware<br />
that ulcers may result from many different causes, such as arterial insufficiencies, diabetes,<br />
rheumatoid arthritis, or malignancy. Where there is mixed venous/arterial etiology, this<br />
condition will have the features of venous ulcer in combination with signs of arterial<br />
impairment (RCN, 1998).<br />
Several studies confirm that malignancy can cause and may be a sequel of leg ulceration<br />
(NZGG, 1999). The RNAO guideline development panel supports the practice of checking for a














