View - Sandra Kalil Bussadori
View - Sandra Kalil Bussadori
View - Sandra Kalil Bussadori

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Original Paper<br />
Caries Res 2008;42:79–87<br />
DOI: 10.1159/000113160<br />
Received: June 4, 2007<br />
Accepted: October 29, 2007<br />
Published online: January 15, 2008<br />
Reproducibility and Accuracy of the<br />
ICDAS-II for Detection of Occlusal Caries<br />
in vitro<br />
a<br />
A. Jablonski-Momeni V. Stachniss b D.N. Ricketts c M. Heinzel-Gutenbrunner a<br />
K. Pieper a<br />
Departments of a Paediatric and Community Dentistry and b Operative Dentistry, Philipps University<br />
of Marburg, Marburg , Germany; c Section of Operative Dentistry, Fixed Prosthodontics and Endodontology,<br />
Dundee Dental School, University of Dundee, Dundee , UK<br />
Key Words<br />
Histology International Caries Detection and Assessment<br />
System Microscopy Occlusal caries Visual inspection<br />
detection of occlusal caries at varying stages of the disease<br />
process which are comparable to previously reported data<br />
using similar visual classification systems.<br />
Copyright © 2008 S. Karger AG, Basel<br />
Abstract<br />
Aim: The aim of this study was to assess inter- and intraexaminer<br />
reproducibility and accuracy in the detection and<br />
assessment of occlusal caries in extracted human teeth using<br />
a newly developed visual method for caries diagnosis<br />
(International Caries Detection and Assessment System,<br />
ICDAS-II). Serial sectioning and microscopy were used as the<br />
‘gold standard’. Methods: The occlusal surfaces of 100 teeth<br />
were examined by 4 dentists using the ICDAS-II graded<br />
scores 0–6. Thereafter the teeth were serially sectioned and<br />
assessed for depth of the lesion with two histological classification<br />
systems. Results: The weighted kappa values for<br />
inter- and intra-examiner reproducibility for the ICDAS-II<br />
examination were 0.62–0.83. There was a moderate relationship<br />
between the visual and both histological examinations<br />
(r s = 0.43–0.72). At the D1 diagnostic threshold (enamel and<br />
dentine lesions) specificity was 0.74–0.91 and sensitivity was<br />
0.59–0.73. At the D3 diagnostic threshold (dentine lesions)<br />
specificity was 0.82–0.94 and sensitivity was 0.48–0.83 for<br />
the 4 examiners. Conclusion: The ICDAS-II system has demonstrated<br />
reproducibility and diagnostic accuracy for the<br />
Dentists have a number of methods at their disposal<br />
for the clinical detection of dental caries on occlusal surfaces.<br />
Apart from purely visual and visual-tactile caries<br />
diagnosis, these include radiography, laser or light fluorescence-based<br />
methods and electrical impedance measurements.<br />
Unfortunately, where occlusal caries is concerned,<br />
a lesion which is reliably detected from a bitewing<br />
radiograph will be advanced, having extended into the<br />
middle third of dentine [Ricketts et al., 1995]. Whilst research<br />
into laser fluorescence methods has resulted in the<br />
production of a commercially available device for clinical<br />
use, a systematic review of the literature has shown that<br />
the majority of studies using it have been in vitro and that<br />
false positive results (low specificity) are a problem [Bader<br />
and Shugars, 2004]. Sheehy et al. [2001] have also<br />
commented that visual inspection seems better suited to<br />
epidemiological investigations than laser fluorescence,<br />
for example. Like the laser fluorescence device, electrical<br />
conductance methods for caries detection suffer from a<br />
lower specificity than clinical visual methods of caries<br />
Fax +41 61 306 12 34<br />
E-Mail karger@karger.ch<br />
www.karger.com<br />
© 2008 S. Karger AG, Basel<br />
0008–6568/08/0422–0079$24.50/0<br />
Accessible online at:<br />
www.karger.com/cre<br />
Dr. Anahita Jablonski-Momeni<br />
Department of Paediatric and Community Dentistry<br />
Philipps University of Marburg, Georg-Voigt-Strasse 3<br />
DE–35033 Marburg (Germany)<br />
Tel. +49 6421 286 3215, Fax +49 6421 286 6691, E-Mail momeni@staff.uni-marburg.de
detection and further research is required before they<br />
could be used in caries clinical trials [Longbottom and<br />
Huysmans, 2004].<br />
In epidemiological examinations, caries has usually<br />
been diagnosed according to the WHO standard, that is,<br />
lesions are recorded at the cavitation level. As defined by<br />
the WHO [1997], caries requires operative treatment (D 3<br />
level) when exposed dentine is visible or undermined<br />
enamel with softened margins can be felt. Such lesions<br />
are likely to be extensive, extending well into dentine,<br />
and rapidly progressive. Therefore, subtler indices are required<br />
which can also register lesions at an earlier noncavitated<br />
stage. This is the only way to establish a valid<br />
basis for caries management aimed at remineralisation of<br />
early enamel and dentine lesions. A system for clinical<br />
caries diagnosis would be ideal if on the one hand it could<br />
detect caries at an early stage and on the other provide<br />
practitioners with a basis for suitable therapies.<br />
The International Caries Detection and Assessment<br />
System (ICDAS) for clinical caries diagnosis was developed<br />
to provide clinicians, epidemiologists and researchers<br />
with an evidence-based system which would allow<br />
standardised data collection in different settings and better<br />
comparison between studies. The aim is to provide<br />
better understanding of caries and its management within<br />
the population and at an individual level [Pitts, 2004].<br />
ICDAS was developed on the basis of insights gained<br />
from a systematic review of the literature on clinical caries<br />
detection systems [Ismail, 2004] and other sources<br />
[Ekstrand et al., 1997, 2001, 2005; Fyffe et al., 2000a;<br />
Chesters et al., 2002; Ricketts et al., 2002]. Use of the<br />
ICDAS was intended to make subsequent studies more<br />
useful for comparison, reviews or meta-analyses and thus<br />
fulfil the requirements of evidence-based dentistry [Richards,<br />
2005].<br />
The aim of this in vitro study was to validate the<br />
ICDAS-II system for caries detection in pits and fissures<br />
using two histological classification systems used in previous<br />
studies. In addition, the reproducibility of the<br />
method was checked against a reference examiner who<br />
was familiar with the ICDAS-II system as well as intraexaminer<br />
reliability.<br />
Materials and Methods<br />
Sample Selection<br />
One hundred unrestored molar (n = 85) and premolar teeth<br />
(n = 15) were selected from a group of extracted teeth stored in<br />
thymol. These were cleaned carefully with a rotating brush and<br />
water and then stored in water.<br />
Table 1. ICDAS-II criteria<br />
ICDAS-II<br />
code<br />
Criteria<br />
0 Sound tooth surface: no evidence of caries after prolonged<br />
air drying (5 s)<br />
1 First visual change in enamel: opacity or discoloration<br />
(white or brown) is visible at the entrance to the pit or<br />
fissure after prolonged air drying, which is not or hardly<br />
seen on a wet surface<br />
2 Distinct visual change in enamel: opacity or discoloration<br />
distinctly visible at the entrance to the pit and fissure<br />
when wet, lesion must still be visible when dry<br />
3 Localized enamel breakdown due to caries with no visible<br />
dentine or underlying shadow: opacity or discoloration<br />
wider than the natural fissure/fossa when wet and<br />
after prolonged air drying<br />
4 Underlying dark shadow from dentine 8 localised<br />
enamel breakdown<br />
5 Distinct cavity with visible dentine: visual evidence of<br />
demineralisation and dentine exposed<br />
6 Extensive distinct cavity with visible dentine and more<br />
than half of the surface involved<br />
One to four easily re-located sites within the pit and fissure<br />
system of each tooth were chosen as potential investigation sites<br />
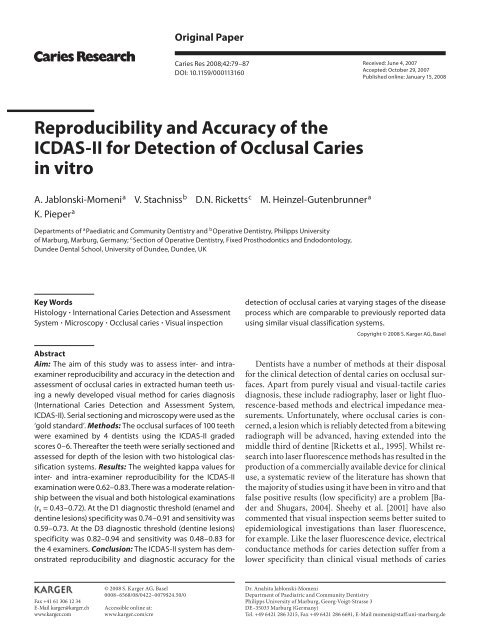
(total sites 181). Digital images of the occlusal surfaces were taken<br />
with the teeth surrounded by a right-angled coordinate system,<br />
which allowed accurate recording and identification of the investigation<br />
sites ( fig. 1 ). Black and white copies of these, printed in<br />
draft quality on plain paper, were used by the examiners during<br />
this study and were only suitable for lesion location.<br />
Training in ICDAS-II<br />
Prior to the visual examination, the reference examiner<br />
(D.N.J.R.) trained 3 other examiners (K.P., V.S. and A.J.-M.) in<br />
the ICDAS-II classification system in a 2-hour session. The training<br />
involved a 30-min lecture on the ICDAS-II system and the<br />
importance of examining clean teeth when both wet and dry. The<br />
details of each score were discussed and a series of images of the<br />
occlusal surface and corresponding histological appearance were<br />
shown to demonstrate that small and subtle changes at the entrance<br />
to the fissure can correspond to marked histological<br />
changes. Following this a series of approximately 20 projected,<br />
magnified images of the occlusal surfaces of teeth with a range<br />
of appearances were discussed and a consensus ICDAS-II score<br />
assigned. This was followed by examination of approximately 20<br />
extracted teeth that were not included in the main study, representing<br />
all ICDAS-II scores. These teeth were initially examined<br />
blind to other examiners, followed by discussion and a consensus<br />
score given.<br />
80<br />
Caries Res 2008;42:79–87<br />
Jablonski-Momeni /Stachniss /Ricketts /<br />
Heinzel-Gutenbrunner /Pieper
ML<br />
b<br />
ML<br />
ML<br />
H<br />
<br />
a<br />
ML<br />
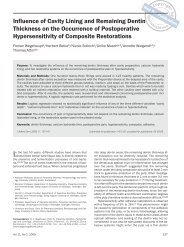
Fig. 1. Occlusal view of a molar tooth with right-angled triangle coordinating system. The length of the embedded<br />
coloured foil (grey in the printed version) allows accurate location of the section in the y-axis, using the<br />
formula H = 2(a – ML). The position of the lesion along each section can then be determined by the x-axis coordinate.<br />
Examiners<br />
The examiners were experienced dentists with an interest in<br />
cariology. The examiners had been qualified for 8, 20, 31 and 37<br />
years, 2 treated both paediatric and adult patients and 2 treated<br />
adults only. All examiners had a history of training in the assessment<br />
of histological sections of teeth. The reference examiner had<br />
been involved in numerous published studies using histological<br />
assessments comparable to those used in this study.<br />
Visual Examination<br />
The teeth were kept moist (in water) throughout the study other<br />
than drying for the examinations, when they were dried with<br />
a 3-in-1 syringe as required. Each examiner examined the teeth<br />
blind to each other according to the ICDAS-II criteria for occlusal<br />
caries ( table 1 , http://www.icdas.org/).<br />
After 3 weeks, 3 of the trained examiners re-examined all of<br />
the teeth in order to determine intra-examiner reproducibility.<br />
The reference examiner was not available to repeat the examinations,<br />
being abroad.<br />
Reproducibility/Accuracy of a Method for<br />
Caries Detection<br />
Caries Res 2008;42:79–87 81
Table 2. Criteria used in the histological examinations<br />
Score<br />
Criteria used in the Downer histological examination<br />
[Downer, 1975]<br />
Criteria used in the ERK histological examination<br />
[Ekstrand et al., 1997]<br />
0 No enamel demineralisation or a narrow surface zone of<br />
opacity (edge phenomenon)<br />
1 Enamel demineralisation limited to the outer 50% of the<br />
enamel layer<br />
2 Demineralisation involving the inner 50% of the enamel,<br />
up to the enamel-dentine junction<br />
No enamel demineralisation or a narrow surface zone of opacity<br />
(edge phenomenon)<br />
Enamel demineralisation limited to the outer 50% of the enamel<br />
layer<br />
Demineralisation involving between 50% of the enamel and outer<br />
third of the dentine<br />
3 Demineralisation involving the outer 50% of the dentine Demineralisation involving the middle third of the dentine<br />
4 Demineralisation involving the inner 50% of the dentine Demineralisation involving the inner third of the dentine<br />
Histological Preparation<br />
For histological examination the roots were resected from the<br />
teeth just apical to the cementum-enamel junction. The crowns<br />
of the teeth were then dehydrated by serially submerging them in<br />
increasing concentrations of alcohol solutions (40, 60, 80, 100,<br />
100%) for 12 h in each. This progressive dehydration of the tooth<br />
reduced damage and facilitated penetration of an alcohol/light<br />
cure acrylic (1: 1) mix (Technovit 7200 VLC, Heraeus Kulzer, Germany)<br />
into which the tooth was placed for 36 h. The acrylic was<br />
then light cured for 10 h (Histolux, Exakt, Germany).<br />
To further reduce section damage and aid mounting of the<br />
specimen for the three-dimensional cutting technique [Stachniss,<br />
2005], the teeth underwent a second stage of embedding in an<br />
acrylic tube which was filled with acrylic (Technovit 7200 VLC)<br />
to completely cover the tooth. Because visual access to the occlusal<br />
surface and investigation sites was now impaired, an accurate<br />
coordinating system was required to correctly assign each section<br />
to the corresponding position within the tooth. To achieve this,<br />
the cut root face was placed on a triangle of foil of known dimensions<br />
(a = 9 mm), height (b = 18 mm) and angle ( = 63.5°) prior<br />
to placement of the specimen in the acrylic tube and the second<br />
embedding stage ( fig. 1 ). The base (a) of the triangle was aligned<br />
with the mesial surface of the tooth and ran parallel with the occlusal<br />
surface. The embedded tooth together with the foil triangle<br />
were then serially sectioned in a buccolingual direction. Each embedded<br />
section therefore contained a section of the coloured foil<br />
in the form of a distinct line in relation to the cut root face. If the<br />
length of the coloured line at the base of the section was ML<br />
( fig. 1 ), the formula H = 2(a – ML) gives the height (H) or y coordinate<br />
of the section. The correct sections could then be determined<br />
for each investigation site, using the x coordinate recorded<br />
on the digital photograph of the occlusal surface. Prior to histological<br />
examination the sections were ground and polished on<br />
waterproof silicon carbide paper (1,200, 2,400 and 4,000 grit; Hermens<br />
or Wirz, Germany) to a specimen thickness of 200 ( 8 30)<br />
m (checked with a digital micrometer; Müller, Germany). In total<br />
11–15 sections were produced per crown and 1–4 sections were<br />
available to view for each investigation site.<br />
Histological Examination<br />
For each investigation site the selected sections were examined<br />
by all 4 examiners using a binocular microscope (Wild Heerbrugg<br />
AG, Gais, Switzerland) using ! 16 magnification and reflected<br />
light. Two different histological classification systems [Downer,<br />
1975; Ekstrand et al., 1997] were used to record caries severity at<br />
each investigation site and this was carried out blindly to the other<br />
examiners ( table 2 ).<br />
Up to 4 sections were available which could be assigned to each<br />
investigation site. A histological score was given to each section<br />
and the worst/deepest score was taken as the definitive score for<br />
further analysis. For each investigation site and each histological<br />
classification system the results from all 4 examiners were then<br />
compared to achieve a consensus score for each site. Where 3 or<br />
more examiners agreed on the histological score, this was taken<br />
as consensus. Where there was greater disagreement, the sections<br />
were reviewed by all examiners and after discussion a consensus<br />
was reached. Caries extent was based upon colour and structural<br />
changes in enamel and dentine, with emphasis being placed on<br />
differentiating carious changes from protective changes of the<br />
pulp-dentine complex, such as tubular sclerosis and reactionary<br />
dentine formation.<br />
Data Management and Statistical Evaluation<br />
Both the ICDAS-II and histology scores were recorded on special<br />
sheets and later transferred to an Excel table. Multiple investigation<br />
sites on a single tooth do not represent statistically independent<br />
data. To ensure that statistical analysis was based on independent<br />
data, one site was randomly chosen (SPSS 14.0) for<br />
each tooth with more than one investigation site, and used as the<br />
score for that tooth.<br />
For the ICDAS-II scores, interexaminer reproducibility was<br />
calculated for all pairs of examiners and intra-examiner reproducibility<br />
was calculated for the trained examiners using weighted<br />
Cohen’s kappa (using linear weights).<br />
For each examiner, the relationship between the visual scoring<br />
system and both of the histological scoring systems (Downer and<br />
ERK) was assessed using the Spearman rank correlation. The<br />
consensus Downer histology was used to calculate sensitivity and<br />
specificity at the D1 and D3 diagnostic threshold. At the D1 diag-<br />
82<br />
Caries Res 2008;42:79–87<br />
Jablonski-Momeni /Stachniss /Ricketts /<br />
Heinzel-Gutenbrunner /Pieper
nostic threshold all histological scores 1–4 were classed as caries<br />
and each ICDAS-II cut-off was used to calculate sensitivity and<br />
specificity for each examiner. Similarly for the D3 diagnostic<br />
threshold histological scores 3 and 4 were classed as caries only<br />
and sensitivity and specificity calculated at each ICDAS-II cutoff.<br />
The ERK histology, using the classification 2–3 as a histological<br />
threshold, was also used to calculate sensitivity and specificity<br />
for each ICDAS-II cut-off. Using these sensitivity and specificity<br />
values ROC analyses were carried out at the D1, D3 and ERK<br />
2–3 thresholds for each examiner.<br />
Table 3. Inter- and intra-examiner reproducibilities for visual<br />
ICDAS-II examinations<br />
Weighted kappa<br />
examiner 1 examiner 2 examiner 3 examiner 4<br />
Examiner 1 0.82 0.74 0.77<br />
Examiner 2 0.78 a 0.70 0.74<br />
Examiner 3 0.74 a 0.62<br />
Examiner 4<br />
0.83 a<br />
a<br />
Intra-examiner data in italics.<br />
R e s u l t s<br />
Initially, 100 teeth and up to 4 sections per independent<br />
investigation site were planned for investigation,<br />
but, owing to section damage on some teeth and to some<br />
not being scored by all examiners, only 93 investigation<br />
sites and 201 corresponding sections were available for<br />
analysis (14 investigations sites had 1 section, 54 had 2<br />
sections, 21 had 3 sections and 4 had 4 sections). The<br />
number of sections per investigation site was dictated by<br />
the size and spread of the lesion.<br />
Three or more examiners agreed on the histological<br />
assessment in 89% of investigation sites when using the<br />
Downer classification and 84% of investigation sites when<br />
using the ERK classification. The interexaminer weighted<br />
kappa values were 0.66–0.75 for the Downer classification<br />
and 0.60–0.74 for the ERK classification. Where disagreement<br />
occurred, a consensus decision was made following<br />
discussion and this was used in subsequent<br />
analyses.<br />
Table 3 shows the intra- and interexaminer reproducibilities<br />
(kappa values) for the visual ICDAS-II examinations.<br />
Table 4 shows the distribution of ICDAS-II data crosstabulated<br />
with both the Downer and ERK histological<br />
scores (consensus) for the independent investigation sites<br />
included in this study for the reference examiner. Table 5<br />
Table 4. Cross tables showing the relationship between the<br />
ICDAS-II scores for examiner 1 and the consensus decision for<br />
Downer and ERK histological classification systems for the independent<br />
data<br />
ICDAS-II<br />
0 1 2 3 4 5 6<br />
Downer histological score<br />
0 15 7 0 0 0 0 0 22<br />
1 4 4 4 1 0 0 0 13<br />
2 2 4 6 1 0 1 1 15<br />
3 0 5 5 14 6 6 0 36<br />
4 0 0 0 0 2 4 1 7<br />
Total 21 20 15 16 8 11 2 93<br />
ERK histological score<br />
0 15 7 0 0 0 0 0 22<br />
1 4 4 4 1 0 0 0 13<br />
2 2 5 10 9 2 2 1 31<br />
3 0 4 1 6 4 6 0 21<br />
4 0 0 0 0 2 3 1 6<br />
Total 21 20 15 16 8 11 2 93<br />
Table 5. Spearman’s correlation coefficients: visual versus histological scores<br />
Spearman’s correlation coefficient<br />
examiner 1 examiner 2 examiner 3 examiner 4 all examiners<br />
Visual versus Downer histological scores 0.60 0.72 0.59 0.48 0.58<br />
Visual versus ERK histological scores 0.58 0.68 0.54 0.43 0.54<br />
Reproducibility/Accuracy of a Method for<br />
Caries Detection<br />
Caries Res 2008;42:79–87 83
Table 6. Area under the ROC curve, optimum sensitivity and specificity and corresponding ICDAS-II threshold used, for each examiner<br />
at each diagnostic threshold (D1, D3 and ERK 2–3)<br />
D1 diagnostic threshold<br />
AUC (SE) CI opt.<br />
sens.<br />
D3 diagnostic threshold<br />
opt.<br />
spec.<br />
ICDAS<br />
cut-off<br />
AUC (SE) CI opt.<br />
sens.<br />
opt.<br />
spec.<br />
ICDAS<br />
cut-off<br />
Examiner 1 0.85 (0.05) 0.75–0.94 0.71 0.91 1–2 0.88 (0.04) 0.81–0.96 0.79 0.90 2–3<br />
Examiner 2 0.86 (0.05) 0.77–0.94 0.73 0.83 1–2 0.87 (0.04) 0.80–0.95 0.69 0.90 2–3<br />
Examiner 3 0.73 (0.06) 0.62–0.84 0.59 0.78 1–2 0.87 (0.04) 0.80–0.94 0.48 0.94 2–3<br />
Examiner 4 0.80 (0.05) 0.70–0.90 0.73 0.74 1–2 0.88 (0.04) 0.80–0.95 0.83 0.82 2–3<br />
AUC = Area under the curve; SE = standard error; CI = 95% confidence interval; opt. sens. = optimum sensitivity; opt. spec. = optimum<br />
specificity.<br />
shows the Spearman’s correlation coefficient for ICDAS-<br />
II visual examination for each examiner, for both Downer<br />
and ERK histological scores. It is generally accepted<br />
that a correlation coefficient of 0.7 or above represents a<br />
strong relationship between two variables.<br />
Table 6 shows the area under the curve for each examiner,<br />
the optimum sensitivity and specificity and the<br />
ICDAS-II cut-off that resulted in this outcome, for the<br />
D1, D3 and ERK 2–3 diagnostic thresholds.<br />
At the D1 diagnostic threshold the optimum sensitivity<br />
and specificity for each examiner was obtained using<br />
ICDAS-II cut-off 1–2. To correctly reflect the D1 diagnostic<br />
threshold all lesions including those with an<br />
ICDAS-II code 1 should have been classed as caries. However,<br />
when this was done, sensitivity was high (mean =<br />
0.89, min. = 0.76, max. = 0.96), but specificity was low<br />
(mean = 0.52, min. = 0.39, max. = 0.61).<br />
The D3 diagnostic threshold used the enamel-dentine<br />
junction to differentiate sound and caries, whereas the<br />
ERK 2–3 diagnostic threshold was deeper, between the<br />
outer third of dentine and middle third of dentine and yet<br />
the same ICDAS-II cut-off gave the optimum sensitivity<br />
and specificity. If a higher ICDAS-II cut-off of 3–4 was<br />
used to reflect this increased severity of lesion when validated<br />
with the ERK 2–3 histological threshold a mean<br />
sensitivity of 0.60 (min. = 0.56, max. = 0.64) and mean<br />
specificity of 0.90 (min. 0.84, max. 0.94) were obtained.<br />
Discussion<br />
Occlusal caries accounts for the majority of new lesions<br />
in the permanent dentition of children, adolescents<br />
and young adults. Whilst one of the most readily accessible<br />
tooth surfaces, it has a complex invaginated anatomy,<br />
which makes caries detection more difficult. There<br />
are numerous treatment options for occlusal caries and<br />
ultimately the aim is to link detection, diagnosis and appropriate<br />
treatment and this study addresses the first step<br />
in this process.<br />
To date little has been published on the visual ICDAS-<br />
II system, but other similar scoring systems have previously<br />
been used. In one study an interexaminer kappa<br />
value of 0.91 and intra-examiner kappa value of 0.9 was<br />
found between 2 examiners using an eight-point scoring<br />
system for diagnosing occlusal caries [Ekstrand et al.,<br />
1995]. Using a five-point scoring system, kappa values of<br />
0.54–0.69 were found for interexaminer reproducibility<br />
of 3 examiners and 0.73–0.89 for intra-examiner agreement<br />
[Ekstrand et al., 1997]. In another study using the<br />
same system, kappa values of 0.47–0.61 between 3 examiners<br />
and 0.56–0.68 for intra-examiner reproducibility<br />
were achieved [Reis et al., 2004]. A recent study which<br />
also used a four-point system for 8 examiners [Souza-<br />
Zaroni et al., 2006], found kappa values of 0.35–0.5<br />
for interexaminer and 0.81–0.85 for intra-examiner reproducibility.<br />
The reproducibility achieved with the<br />
ICDAS-II seven-point scoring system in this study compared<br />
favourably with those cited. However, it is likely<br />
that the cited studies reported unweighted kappa values,<br />
like Ekstrand [1997], since they did not mention weighting.<br />
If we compare the unweighted kappas from the<br />
present study (interexaminer 0.32–0.61; intra-examiner<br />
0.54–0.65), the differences disappear. Although intra-examiner<br />
kappa values could not be calculated for<br />
the reference examiner, this examiner had used the<br />
ICDAS-II system extensively and achieved acceptable<br />
intra-examiner kappa values in a previously published<br />
84<br />
Caries Res 2008;42:79–87<br />
Jablonski-Momeni /Stachniss /Ricketts /<br />
Heinzel-Gutenbrunner /Pieper
ERK 2–3 diagnostic threshold<br />
AUC (SE) CI opt.<br />
sens.<br />
opt.<br />
spec.<br />
ICDAS<br />
cut-off<br />
0.84 (0.04) 0.76–0.93 0.84 0.75 2–3<br />
0.84 (0.05) 0.75–0.93 0.80 0.79 2–3<br />
0.86 (0.04) 0.78–0.94 0.64 0.90 2–3<br />
0.84 (0.04) 0.76–0.92 0.88 0.68 2–3<br />
study [Ekstrand et al., 1997] using comparable visual<br />
criteria. Interexaminer kappa values between the reference<br />
examiner and 3 trained examiners were also acceptable<br />
( table 3 ).<br />
Histological validation of caries and in particular occlusal<br />
caries is notoriously difficult as preparing thin sections<br />
entails tooth tissue loss. Simply hemisecting a tooth<br />
through the lesion may not pass through the deepest aspect<br />
of the lesion in question. Taking a single section<br />
through an investigation site is also problematic if only<br />
one side of the section is examined as the depth of a lesion<br />
will vary from one side of a section to another [Ricketts<br />
et al., 1998]. Whilst only one side of the section was viewed<br />
in this study because of the mounting technique used, the<br />
sections were serial and the side viewed on one section<br />
corresponded to the side not viewed on the preceding<br />
section. These problems arise because of the three-dimensional<br />
nature of the spread of caries dictated by the<br />
complex anatomy of the occlusal surface. A lesion may<br />
originate at one site on the surface of the tooth but spread<br />
obliquely and non-symmetrically beneath the tooth surface.<br />
To overcome this problem and to record the deepest<br />
aspect of the lesion from where it originated at the investigation<br />
site, 1–4 sections were used depending on the<br />
severity of the lesion. The use of the coordinate system<br />
ensured accurate location of each section and thus that<br />
the lesion on the section originated from the investigation<br />
site in question. Because of the mode of spread alluded<br />
to above, it could be argued that the appearance at<br />
one site may influence the decision at another. For example,<br />
if one site was obviously carious, the likelihood of<br />
an adjacent site also being carious and recorded as such<br />
is much higher. The data collected at multiple sites cannot<br />
therefore be regarded as independent. To overcome this<br />
problem one investigation site per tooth was randomly<br />
selected for analysis.<br />
In previous studies comparing both visual classification<br />
systems and histological classification systems of increasing<br />
lesion severity, the relationships between the<br />
two variables have been strong, with Spearman correlation<br />
coefficients of 0.87 for an eight-point visual scale<br />
[Ekstrand et al., 1995] and 0.87–0.93 for a five-point visual<br />
scale [Ekstrand et al., 1997]. In this study the relationship<br />
between the ICDAS-II visual classification system<br />
and either histological classification system was not<br />
as strong (r s = 0.48–0.72 using Downer histology and<br />
0.43–0.68 for ERK histology).<br />
For comparison with other studies using similar visual<br />
classification systems or different novel technologies,<br />
the Downer histology was used in the ROC analyses<br />
for each examiner at the D1 and D3 diagnostic threshold<br />
and the ERK histology was used similarly at the 2–3<br />
threshold. For all examiners the ICDAS-II system produced<br />
areas under the ROC curves in excess of 0.7.<br />
At the D1 diagnostic threshold the mean sensitivity<br />
and specificity of the ICDAS-II were 0.69 and 0.82, respectively<br />
( table 6 ). The sensitivity was found to be higher<br />
than that reported in a previous study using a different<br />
eight-point visual scale and three groups of examiners<br />
[Fyffe et al., 2000b] where sensitivity ranged between 0.46<br />
and 0.5. The specificity in this study was similar to that<br />
reported by Fyffe et al. [2000b], who found specificities<br />
of 0.66–0.86. However, in this study optimum sensitivity<br />
and specificity were achieved at the ICDAS-II cut-off 1–2<br />
and not 0–1, which would have been consistent with the<br />
D1 diagnostic threshold. When the 0–1 cut-off was used,<br />
sensitivity was high (mean = 0.89), but specificity was low<br />
(mean = 0.52). This means that a large number of sound<br />
sites were incorrectly scored as carious and this may have<br />
been due to stained sites, areas of fluorosis or developmental<br />
defects being incorrectly scored as caries. It is important<br />
to question what impact this would have clinically.<br />
From table 4 it can be seen that the sound sites<br />
that were incorrectly scored as carious were given a low<br />
ICDAS-II score which would not require operative treatment.<br />
The worse clinical outcome would therefore be giving<br />
prevention to a sound site, which in a high-risk patient<br />
would be of benefit.<br />
In this study, at the D3 diagnostic threshold mean sensitivity<br />
was 0.70 and specificity was 0.89 using ICDAS-II<br />
scores 2–3 to differentiate sound sites from those with<br />
dentine caries ( table 6 ). These are similar to those reported<br />
by Downer [1989], who in a review of the literature<br />
found that trained and experienced examiners using a<br />
Reproducibility/Accuracy of a Method for<br />
Caries Detection<br />
Caries Res 2008;42:79–87 85
visual method of diagnosis can detect dentine caries with<br />
a sensitivity in excess of 0.6 and a specificity in excess of<br />
0.8 in a sample of borderline lesions.<br />
In the Downer histology the enamel-dentine junction<br />
is taken as a diagnostic threshold to calculate diagnostic<br />
accuracy at the D3 level (code 2–3), whereas in the ERK<br />
histological system the enamel-dentine junction is not<br />
used and the histological threshold 2–3 corresponds to<br />
deeper dentine lesions (a threshold between outer third<br />
of dentine and middle third of dentine). Despite this, similar<br />
levels of sensitivity and specificity were obtained<br />
when the same ICDAS-II cut-off 2–3 was used. Using<br />
these ICDAS-II cut-offs and ERK histological threshold<br />
allowed comparison with previous work where higher<br />
sensitivity (0.92–0.97) and specificity (0.85–0.93) values<br />
were obtained [Ekstrand et al., 1997]. In the present study,<br />
when a higher ICDAS-II cut-off 3–4 was used, specificity<br />
values increased to a mean of 0.90 at the expense of sensitivity,<br />
which fell to a mean of 0.60. However, the level of<br />
overall accuracy (sensitivity plus specificity) was of the<br />
same order of magnitude as when ICDAS-II cut-off 2–3<br />
was used.<br />
A review of studies that included the validation of diagnostic<br />
techniques against a histological gold standard<br />
[Ie and Verdonschot, 1994] showed that visual inspection<br />
performed comparatively poorly for occlusal caries diagnosis<br />
compared to electrical resistance measurements<br />
and fibre-optic transillumination. In addition to this, another<br />
systematic review of the literature has shown that<br />
for visual examination specificity is high but sensitivity<br />
is low [Bader et al., 2001]. In these two reviews meta-analyses<br />
have either not been carried out or the results should<br />
be regarded with caution because of the heterogeneity of<br />
the studies included. However, it would appear that in<br />
general, visual examination has been regarded as poor for<br />
caries detection. In contrast, this study has shown that by<br />
meticulously examining clean dry teeth sensitivity of a<br />
visual examination can be improved after a short training<br />
period.<br />
In summary, after a relatively short training period 3<br />
examiners were able to achieve results using the ICDAS-<br />
II system that were comparable to that of the examiner<br />
carrying out the training. The ICDAS-II system demonstrated<br />
reproducibility and diagnostic accuracy for the<br />
detection of occlusal caries at varying stages of the disease<br />
process comparable to those published in previous<br />
studies using similar visual criteria. The moderate to<br />
strong relationship with histological extent also demonstrates<br />
its potential to monitor lesions with time. With the<br />
development of more extensive and advanced training<br />
packages and calibration exercises there may be scope to<br />
improve the reproducibility and accuracy further. In addition,<br />
such packages would allow further dissemination<br />
of ICDAS-II, allowing data from clinical studies in primary<br />
dental care, clinical trials and epidemiological surveys<br />
to have greater clarity and comparability for metaanalyses.<br />
References<br />
Bader JD, Shugars DA: A systematic review of the<br />
performance of a laser fluorescence device<br />
for detecting caries. J Am Dent Assoc 2004;<br />
135: 1413–1426.<br />
Bader JD, Shugars DA, Bonito AJ: Systematic reviews<br />
of selected dental caries diagnostic and<br />
management methods. J Dent Educ 2001; 65:<br />
960–968.<br />
Chesters RK, Pitts NB, Matuliene G, Kvedariene<br />
A, Huntington E, Bendinskaite R, Balciuniene<br />
I, Matheson JR, Nicholson JA, Gendvilyte<br />
A, Sabalaite R, Ramanauskiene J, Savage D,<br />
Mileriene J: An abbreviated caries clinical<br />
trial design validated over 24 months. J<br />
Dent Res 2002; 81: 637–640.<br />
Downer MC: Concurrent validity of an epidemiological<br />
diagnostic system for caries with<br />
the histological appearance of extracted<br />
teeth as validating criterion. Caries Res 1975;<br />
9: 231–246.<br />
Downer MC: Validation of methods used in dental<br />
caries diagnosis. Int Dent J 1989; 39: 241–<br />
246.<br />
Ekstrand KR, Kuzmina I, Bjørndal L, Thylstrup<br />
A: Relationship between external and histologic<br />
features of progressive stages of caries<br />
in the occlusal fossa. Caries Res 1995; 29:<br />
243–250.<br />
Ekstrand KR, Ricketts DN, Kidd EA: Reproducibility<br />
and accuracy of three methods for assessment<br />
of demineralization depth on the<br />
occlusal surface: an in vitro examination.<br />
Caries Res 1997; 31: 224–231.<br />
Ekstrand KR, Ricketts DN, Kidd EA: Occlusal<br />
caries: pathology, diagnosis and logical management.<br />
Dent Update 2001; 28: 380–387.<br />
Ekstrand KR, Ricketts DN, Longbottom C, Pitts<br />
NB: Visual and tactile assessment of arrested<br />
initial enamel carious lesions: an in vivo pilot<br />
study. Caries Res 2005; 39: 173–177.<br />
Fyffe HE, Deery CH, Nugent ZJ, Nuttall NM,<br />
Pitts NB: Effect of diagnostic threshold on<br />
the validity and reliability of epidemiological<br />
caries diagnosis using the Dundee Selectable<br />
Threshold Method for caries diagnosis<br />
(DSTM). Community Dent Oral Epidemiol<br />
2000a;28: 42–51.<br />
Fyffe HE, Deery C, Nugent ZJ, Nuttall NM, Pitts<br />
NB: In vitro validity of the Dundee Selectable<br />
Threshold Method for caries diagnosis<br />
(DSTM). Community Dent Oral Epidemiol<br />
2000b;28: 52–58.<br />
Ie YL, Verdonschot EH: Performance of diagnostic<br />
systems in occlusal caries detection<br />
compared. Community Dent Oral Epidemiol<br />
1994; 22: 187–191.<br />
Ismail AI: Visual and visuo-tactile detection of<br />
dental caries. J Dent Res 2004; 83(special No<br />
C):C56–C66.<br />
Longbottom C, Huysmans MC: Electrical measurements<br />
for use in caries clinical trials. J<br />
Dent Res 2004; 83(special No C):C76–C79.<br />
86<br />
Caries Res 2008;42:79–87<br />
Jablonski-Momeni /Stachniss /Ricketts /<br />
Heinzel-Gutenbrunner /Pieper
Pitts N: ‘ICDAS’ – an international system for<br />
caries detection and assessment being developed<br />
to facilitate caries epidemiology, research<br />
and appropriate clinical management.<br />
Community Dent Health 2004; 21:<br />
193–198.<br />
Reis A, Zach VL Jr, de Lima AC, de Lima Navarro<br />
MF, Grande RH: Occlusal caries detection:<br />
a comparison of DIAGNOdent and two<br />
conventional diagnostic methods. J Clin<br />
Dent 2004; 15: 76–82.<br />
Richards D: Outcomes, what outcomes? (Editorial).<br />
Evid Based Dent 2005; 6: 1.<br />
Ricketts DN, Ekstrand KR, Kidd EA, Larsen T:<br />
Relating visual and radiographic ranked<br />
scoring systems for occlusal caries detection<br />
to histological and microbiological evidence.<br />
Oper Dent 2002; 27: 231–237.<br />
Ricketts DN, Kidd EA, Smith BG, Wilson RF:<br />
Clinical and radiographic diagnosis of occlusal<br />
caries: a study in vitro. J Oral Rehabil<br />
1995; 22: 15–20.<br />
Ricketts DN, Watson TF, Liepins PJ, Kidd EA: A<br />
comparison of two histological validating<br />
techniques for occlusal caries. J Dent 1998;<br />
26: 89–96.<br />
Sheehy EC, Brailsford SR, Kidd EA, Beighton D,<br />
Zoitopoulos L: Comparison between visual<br />
examination and a laser fluorescence system<br />
for in vivo diagnosis of occlusal caries. Caries<br />
Res 2001; 35: 421–426.<br />
Souza-Zaroni WC, Ciccone JC, Souza-Gabriel<br />
AE, Ramos RP, Corona SAM, Palma-Dibb<br />
RG: Validity and reproducibility of different<br />
combinations of methods for occlusal caries<br />
detection: an in vitro comparison. Caries<br />
Res 2006; 40: 194–201.<br />
Stachniss V: Zur Hartschnitt-Technik nicht entkalkter<br />
Zähne und digitale makrofotografische<br />
Reproduktion histologischer Präparate.<br />
Research Report, Philipps University<br />
Marburg, 2005.<br />
WHO: Oral Health Surveys: Basic Methods,<br />
ed 4. Geneva, World Health Organization,<br />
1997.<br />
Reproducibility/Accuracy of a Method for<br />
Caries Detection<br />
Caries Res 2008;42:79–87 87