

The Outcomes of Concomitant Radiation Plus Temozolomide ... - NCI
The Outcomes of Concomitant Radiation Plus Temozolomide ... - NCI
The Outcomes of Concomitant Radiation Plus Temozolomide ... - NCI

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
±IU W / 3<br />
Journal <strong>of</strong> the Egyptian Nat. Cancer Inst., Vol. 21, No. 2, June: 107-119, 2009<br />
<strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
Followed by Adjuvant <strong>Temozolomide</strong> for Newly Diagnosed<br />
High Grade Gliomas: <strong>The</strong> Preliminary Results <strong>of</strong> Single<br />
Center Prospective Study<br />
HANAN SHAWKY, M.D.; ABDEL HALIM ABO HAMAR, M.D.; SAMAR GALAL, M.D.;<br />
FATMA ZAKARIA, M.D. and DALIA EL-SHORBAGY, M.D.<br />
<strong>The</strong> Department <strong>of</strong> Clinical Oncology, Tanta University Hospital.<br />
ABSTRACT<br />
Purpose: <strong>Temozolomide</strong> (TMZ) is an oral alkylating<br />
agent with demonstrated efficacy as second-line therapy<br />
for patients with recurrent anaplastic astrocytoma and<br />
glioblastoma multiforme (GBM). We reported the<br />
preliminary results <strong>of</strong> the treatment with concomitant<br />
radiation therapy (RT) plus TMZ followed by adjuvant<br />
TMZ therapy in patients with newly diagnosed high grade<br />
gliomas (HGG) to determine the safety, tolerability, and<br />
efficacy.<br />
Patients and Methods: Between January, 2006 and<br />
December, 2007, a total <strong>of</strong> 27 patients over the age <strong>of</strong> 18<br />
years with newly diagnosed, histologically confirmed<br />
HGG were assigned to receive oral TMZ (75 mg/m 2 /d x<br />
7 d/wk for 6 weeks, from the first to the last day <strong>of</strong> RT)<br />
with fractionated RT (60 Gy total dose: 2 Gy x 5 d/wk for<br />
6 weeks) followed by TMZ monotherapy (150 to 200<br />
mg/m 2 /d x 5 days, every 28 days for six cycles) at Clinical<br />
Oncology Department, Faculty <strong>of</strong> Medicine, Tanta<br />
University Hospital. <strong>The</strong> primary end point was overall<br />
survival; secondary end points were progression-free<br />
survival, safety and tolerability.<br />
Results: At a median follow-up period <strong>of</strong> 17 months<br />
(range; 5-30 months), the median progression-free survival<br />
(PFS) for all patients with HGG was 11 months, and the<br />
one-year PFS rate was 43.14%. <strong>The</strong> median overall survival<br />
(OS) was 19 months and the one-year OS rate was 81.2%.<br />
Patients with GBM were analyzed separately from HGG,<br />
and the median overall survival (OS) was 17 months, and<br />
the one-year OS rate was 83.3%. <strong>The</strong> median PFS was 10<br />
months, and the one-year PFS rate was 27.8%. <strong>The</strong> mean<br />
age was 50.2 years (standard deviation ±9.7284), and<br />
44.4% <strong>of</strong> patients had undergone biopsy only. <strong>The</strong>re was<br />
no mortality caused by drug toxicity. Patients younger<br />
than 50 years old and patients who underwent debulking<br />
Correspondence: Dr Hanan Shawky Gamal El-Deen, 37-<br />
Ibn Sinna Street, kafr El Zayat, Gharbya, hannshawky@<br />
yahoo.com<br />
surgery had the best survival outcome.<br />
Conclusion: <strong>The</strong> addition <strong>of</strong> TMZ to RT followed by<br />
adjuvant TMZ was well tolerated, and has shown promising<br />
activity in the treatment <strong>of</strong> newly diagnosed HGG. Further<br />
investigation is warranted.<br />
Key Words: <strong>Temozolomide</strong> – Radiotherapy – High grade<br />
glioma.<br />
INTRODUCTION<br />
Primary brain tumors comprise only<br />
approximately 2% <strong>of</strong> all malignant diseases [1].<br />
However, with an incidence <strong>of</strong> 5 per 100,000<br />
persons, more than 17,000 cases are diagnosed<br />
every year in the United States, with<br />
approximately 13,000 associated deaths [2]. In<br />
adults, the most common histologies are grade<br />
3 anaplastic astrocytoma (AA) and grade 4<br />
glioblastoma multiforme (GBM) [1,3]. <strong>The</strong><br />
standard management <strong>of</strong> malignant gliomas<br />
involves surgical resection to the extent that is<br />
safely feasible [4], followed by radiotherapy<br />
(RT) with or without adjuvant chemotherapy<br />
[5-10]. Despite this multidisciplinary approach,<br />
the prognosis for patients with GBM remains<br />
poor. <strong>The</strong> median survival rates for GBM are<br />
typically in the range <strong>of</strong> 9 to 12 months, with<br />
2-year survival rates in the range <strong>of</strong> only 8%<br />
to 12% [11-15].<br />
In the United States, adjuvant carmustine,<br />
a nitrosourea drug, is commonly prescribed<br />
[16,17]. Nitrosoureas are the main<br />
chemotherapeutic agents used in the treatment<br />
<strong>of</strong> malignant brain tumors; however, they have<br />
107
108<br />
<strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
shown only modest antitumor activity [11,13].<br />
Cooperative-group trials have investigated the<br />
addition <strong>of</strong> various chemotherapeutic regimens<br />
to radiotherapy [18-21], but no randomized phase<br />
3 trial <strong>of</strong> nitrosourea-based adjuvant<br />
chemotherapy has demonstrated a significant<br />
survival benefit as compared with radiotherapy<br />
alone, although there were more long-term<br />
survivors in the chemotherapy groups in some<br />
studies [22].<br />
<strong>Temozolomide</strong> (TMZ) is a novel, oral,<br />
second-generation, alkylating agent that has<br />
demonstrated antitumor activity as a single<br />
agent or in combination with other<br />
chemotherapeutic agents in the treatment <strong>of</strong><br />
recurrent and newly diagnosed GBM [23-32].<br />
After oral administration, temozolomide is<br />
rapidly absorbed with almost 100%<br />
bioavailability [33]. It readily crosses the bloodbrain<br />
barrier and achieves effective<br />
concentrations in the CNS with a reported<br />
plasma-CSF ratio <strong>of</strong> approximately 30% to 40%<br />
<strong>of</strong> those observed in the plasma [34,35]. <strong>The</strong><br />
approved conventional schedule is a daily dose<br />
<strong>of</strong> 150 to 200 mg per square meter <strong>of</strong> bodysurface<br />
area for 5 days <strong>of</strong> every 28-day cycle.<br />
Daily therapy at a dose <strong>of</strong> 75 mg per square<br />
meter for up to seven weeks is safe; this level<br />
<strong>of</strong> exposure to temozolomide [36] depletes the<br />
DNA-repair enzyme O6-methylguanine-DNA<br />
methyltransferase (MGMT) [37]. This effect<br />
may be important because low levels <strong>of</strong> MGMT<br />
in tumor tissue are associated with longer<br />
survival among patients with glioblastoma [38,39]<br />
who are receiving nitrosourea-based adjuvant<br />
chemotherapy [40,41].<br />
<strong>The</strong> concurrent administration <strong>of</strong> TMZ and<br />
radiation has been explored in vitro and in vivo<br />
[42]. In vitro studies have shown that, depending<br />
on the cell line, treatment <strong>of</strong> glioma cells with<br />
TMZ and x-rays can have either an additive or<br />
synergistic effect. In a phase II study by Stupp,<br />
et al. [43], demonstrated that concomitant RT<br />
plus continuous daily TMZ followed by adjuvant<br />
TMZ is well tolerated and improves survival<br />
in patients with newly diagnosed GBM. Another<br />
completed phase III studies by the European<br />
Organisation for Research and Treatment <strong>of</strong><br />
Cancer (EORTC) had confirmed this data [23,44].<br />
On the basis <strong>of</strong> this evidence, we initiated<br />
this study to investigate the safety, tolerability,<br />
and survival <strong>of</strong> concomitant RT plus TMZ<br />
therapy followed by adjuvant TMZ therapy in<br />
patients with newly diagnosed HGG.<br />
PATIENTS AND METHODS<br />
Patients:<br />
Between January, 2006 and December, 2007,<br />
32 patients over the age <strong>of</strong> 18 years with newly<br />
diagnosed, histologically confirmed HGG, were<br />
the subjects <strong>of</strong> this study, <strong>of</strong> which 27 were<br />
assessable for response at Clinical Oncology<br />
Department, Faculty <strong>of</strong> Medicine, Tanta<br />
University Hospital. Five patients were<br />
ineligible, not treated, or incorrectly treated:<br />
reasons included treatment refusal (n=2) and<br />
hepatic insufficiency (n=3). Patients were<br />
required to have a Karn<strong>of</strong>sky performance status<br />
(KPS) <strong>of</strong> ≥70 and adequate hematologic, renal,<br />
and hepatic functions, defined as absolute<br />
neutrophil count 1.5x10 9 cells per liter; platelet<br />
count 100x10 9 cells per liter; hemoglobin more<br />
than 90 g/L; serum creatinine and total serum<br />
bilirubin 1.5 times the upper limit <strong>of</strong> normal;<br />
aspartate aminotransferase or alanine<br />
aminotransferase less than 2.5 times the upper<br />
limit <strong>of</strong> normal; and alkaline phosphatase less<br />
than 2.5 times the upper limit <strong>of</strong> normal. Study<br />
enrollment had to be within six weeks from<br />
diagnostic biopsy or resection. Eligible patients<br />
were also required to have no other severe<br />
underlying disease (including chronic hepatitis<br />
B or C infection). Exclusion criteria included<br />
any medical condition that could interfere with<br />
the oral administration <strong>of</strong> temozolomide or any<br />
previous or concurrent malignancies at other<br />
sites.<br />
Study design and treatment:<br />
Within six weeks after the histologic<br />
diagnosis <strong>of</strong> HGG, we assigned eligible patients<br />
to receive temozolomide (marketed as Temodal)<br />
at a dose <strong>of</strong> 75 mg per square meter per day,<br />
given 7 days per week from the first day <strong>of</strong><br />
radiotherapy until the last day <strong>of</strong> radiotherapy,<br />
in a fasting state, 1 hour before RT, and in the<br />
morning on days without RT. <strong>Concomitant</strong> focal<br />
RT was delivered once daily at 2 Gy per fraction,<br />
5 d/wk, for a total <strong>of</strong> 60 Gy. Adequate<br />
immobilization masks were required to ensure<br />
reproducibility. Treatment volumes were<br />
determined on the basis <strong>of</strong> preoperative contrastenhanced<br />
computed tomography (CT) or<br />
gadolinium-enhanced magnetic resonance
Hanan Shawky, et al. 109<br />
imaging (MRI) <strong>of</strong> the brain. Treatment volume<br />
generally included the contrast-enhancing lesion<br />
plus a 2- to 3-cm margin, depending on the<br />
location. <strong>Radiation</strong> therapy was delivered with<br />
60Co photons. After a 4-week break, patients<br />
were then to receive up to six cycles <strong>of</strong> adjuvant<br />
temozolomide according to the standard 5-day<br />
schedule every 28 days. <strong>The</strong> dose was 150 mg<br />
per square meter for the first cycle and was<br />
increased to 200 mg per square meter beginning<br />
with the second cycle, so long as there were no<br />
hematologic toxic effects. Prophylactic<br />
antiemetics were used only as required during<br />
concomitant RT plus temozolomide therapy.<br />
Prophylactic antiemetics, including<br />
metoclopramide or 5-hydroxytryptamine-3<br />
antagonists, were routinely prescribed once a<br />
day before adjuvant temozolomide.<br />
Anticonvulsants and corticosteroids were<br />
administered as needed.<br />
Surveillance and follow-up:<br />
<strong>The</strong> baseline examination included a<br />
complete medical history, physical examination,<br />
determination <strong>of</strong> performance status,<br />
hematology and clinical chemistry assessments,<br />
and gadolinium-enhanced MRI or contrastenhanced<br />
CT <strong>of</strong> the brain. During radiotherapy<br />
with temozolomide, complete blood counts were<br />
checked weekly, and blood chemistry was<br />
checked monthly. During adjuvant<br />
temozolomide therapy, patients underwent a<br />
monthly clinical evaluation and a comprehensive<br />
evaluation at the end <strong>of</strong> cycles 3 and 6. Tumor<br />
progression was defined according to the<br />
modified WHO criteria as an increase in tumor<br />
size by 25 percent, the appearance <strong>of</strong> new<br />
lesions, or an increased need for corticosteroids<br />
[45]. When there was tumor progression, patients<br />
were treated at the investigator's discretion, and<br />
the type <strong>of</strong> second-line therapy was recorded.<br />
Toxic effects were graded according to the<br />
National Cancer Institute Common Toxicity<br />
Criteria, version 2.0, with a score <strong>of</strong> 1 indicating<br />
mild adverse effects, a score <strong>of</strong> 2 moderate<br />
adverse effects, a score <strong>of</strong> 3 severe adverse<br />
effects, and a score <strong>of</strong> 4 life-threatening adverse<br />
effects.<br />
Statistical analysis:<br />
<strong>The</strong> primary end point was overall survival;<br />
secondary end points were progression-free<br />
survival, and safety. Toxicity was graded<br />
according to the common toxicity criteria<br />
(version 2.0). Safety and toxicity are reported<br />
for all treated patients.<br />
Toxic effects are reported separately for the<br />
radiotherapy period, defined as extending from<br />
day 1 <strong>of</strong> radiotherapy until 28 days after the<br />
last day <strong>of</strong> radiotherapy, or until the first day<br />
<strong>of</strong> adjuvant temozolomide therapy. <strong>The</strong><br />
adjuvant-therapy period was defined as<br />
extending from the first day <strong>of</strong> adjuvant<br />
temozolomide therapy until 35 days after day<br />
1 <strong>of</strong> the last cycle <strong>of</strong> temozolomide. Findings<br />
with respect to the quality <strong>of</strong> life are not reported<br />
here.<br />
Overall survival was calculated from the<br />
time <strong>of</strong> study entry until death or last followup<br />
according to the Kaplan-Meier method [46]<br />
with SPSS [Statistical package] (version 9.0).<br />
Mean and standard deviation were estimates <strong>of</strong><br />
quantitative data. Overall survival and<br />
progression-free survival were compared by the<br />
Kaplan-Meier method [46] with statistical<br />
significance assessed by the log-rank test. All<br />
p values were two-tailed; a value <strong>of</strong> ≤0.05 was<br />
considered significant.<br />
RESULTS<br />
Patient characteristics:<br />
Patients ≥18 years <strong>of</strong> age with newly<br />
diagnosed and histologically proven HGG were<br />
eligible for the study. Patient demographics and<br />
baseline disease characteristics for the eligible<br />
27 patients are listed in Table (1). <strong>The</strong> mean<br />
age was 50.2±9.7 years old, (range; 21-71 years<br />
old). <strong>The</strong> majority <strong>of</strong> patients had a Karn<strong>of</strong>sky<br />
performance status (KPS) <strong>of</strong> ≥80. About 44%<br />
<strong>of</strong> the patients underwent biopsy only, 22.2%<br />
underwent gross total resection, and 18.5%<br />
underwent subtotal resection, however,<br />
immediate postoperative imaging was not<br />
performed in all patients. Histopthological slide<br />
revisions were confirmed the diagnosis <strong>of</strong><br />
glioblastoma in 66.7% <strong>of</strong> the reviewed cases;<br />
25.9% had anaplastic astrocytoma (WHO grade<br />
III), and in 7.4% <strong>of</strong> the patients the diagnosis<br />
was oligodendroglioma (WHO grade III). <strong>The</strong><br />
mean time from diagnosis to the start <strong>of</strong> therapy<br />
with RT plus temozolomide was 2.7 weeks,<br />
standard deviation ±0.9842, (range, 1-5 weeks).<br />
Table (2) summarizes the details <strong>of</strong><br />
treatment. Among the 27 patients who were<br />
assigned to receive concomitant radiotherapy
110<br />
<strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
plus temozolomide, 17 (63%) completed both<br />
radiotherapy and temozolomide as planned. Ten<br />
patients (37%) prematurely discontinued<br />
adjuvant temozolomide because <strong>of</strong> toxic effects<br />
(in 3 patients), disease progression (in 5), or<br />
other reasons (in 2). <strong>The</strong> majority <strong>of</strong> patients<br />
completed their RT within the prescribed 6<br />
weeks (42±3 days). Unplanned interruptions in<br />
RT were usually brief (median, four days) and<br />
interruptions due to the toxicity <strong>of</strong> therapy<br />
Table (1): Demographic characteristics <strong>of</strong> the 27 patients<br />
with high grade gliomas at baseline.<br />
Characteristic<br />
Age (years):<br />
Mean<br />
Range<br />
Hanan Shawky, et al. 111<br />
was discontinued early because <strong>of</strong> progressive<br />
disease in 5 patients (18.5%)]. Only 5 patients<br />
discontinued adjuvant temozolomide because<br />
<strong>of</strong> toxic effects. Beginning with cycle 2, the<br />
dose <strong>of</strong> temozolomide was increased to 200 mg<br />
per square meter in 70.4% <strong>of</strong> patients.<br />
Seventeen patients (63%) received all<br />
concomitant and adjuvant temozolomide as<br />
planned in the protocol. <strong>The</strong> response rate,<br />
including complete remission and partial<br />
remission, was 55.6%.<br />
Safety and tolerability:<br />
We analyzed adverse events separately<br />
during radiotherapy with concomitant<br />
temozolomide, the adjuvant-therapy period, and<br />
the entire study period (from study entry until<br />
disease progression or last follow-up).<br />
Hematologic toxicity and infection:<br />
<strong>Concomitant</strong> phase <strong>of</strong> treatment. During the<br />
concomitant RT plus temozolomide phase, grade<br />
3 or 4 neutropenia occurred in 2 patients (7.4%)<br />
(Table 3), and grade 3 or 4 thrombocytopenia<br />
occurred in 2 patients (7.4%), with 1 patient<br />
experiencing platelet counts <strong>of</strong> less than 10,000<br />
cells per cubic millimeter. Grade 3 or 4<br />
lymphocytopenia occurred in 3 patients (11.1%).<br />
Two patients had infections that required<br />
hospitalization and treatment interruption.<br />
Analysis indicated that 1 <strong>of</strong> the 2 patients<br />
developed pneumonia. This patient was<br />
receiving corticosteroids and experienced grade<br />
4 neutropenia and lymphocytopenia at the time<br />
<strong>of</strong> infection. One patient required surgical<br />
revision <strong>of</strong> a scar infection and osteomyelitis 3<br />
weeks after start <strong>of</strong> RT. However, this patient's<br />
blood counts were within normal limits during<br />
treatment.<br />
Adjuvant temozolomide: During the adjuvant<br />
temozolomide phase, grade 3 or 4 neutropenia<br />
or thrombocytopenia occurred in 7.4% and<br />
18.5% <strong>of</strong> patients, respectively. Five patients<br />
required a dose reduction or delay because <strong>of</strong><br />
grade 3 or 4 thrombocytopenia.<br />
Non-hematologic toxicities:<br />
Non-hematologic toxicities were mild to<br />
moderate (Table 4). During the CCRT phase,<br />
prophylactic antiemetics were required in 59.3%<br />
<strong>of</strong> patients; however, only 7 patients (25.9%)<br />
received antiemetics for longer than the first<br />
Table (3): Hematologic toxicities and infection in the 27 patients with high grade<br />
gliomas.<br />
RT with concomitant TMZ<br />
Adjuvant TMZ<br />
Adverse Event<br />
Grade 3<br />
Grade 4<br />
Grade 3<br />
Grade 4<br />
No. %<br />
No. %<br />
No.<br />
%<br />
No.<br />
%<br />
Anemia<br />
Neutropenia<br />
Thrombocytopenia<br />
Lymphocytopenia<br />
Infection<br />
1<br />
1<br />
1<br />
2<br />
1<br />
3.7<br />
3.7<br />
3.7<br />
7.4<br />
3.7<br />
0<br />
1<br />
1<br />
2<br />
1<br />
0<br />
3.7<br />
3.7<br />
3.7<br />
3.7<br />
1<br />
1<br />
2<br />
3<br />
0<br />
3.7<br />
3.7<br />
7.4<br />
11.1<br />
0<br />
0<br />
1<br />
3<br />
3<br />
0<br />
0<br />
3.7<br />
11.1<br />
11.1<br />
0<br />
Table (4): Non-hematologic toxicities in the 27 patients with high grade gliomas.<br />
Adverse Event<br />
RT with concomitant TMZ<br />
Grade 2 Grade 3 Grade 4 Grade 2<br />
Adjuvant TMZ<br />
Grade 3 Grade 4<br />
No.<br />
%<br />
No.<br />
%<br />
No. % No. %<br />
No. % No. %<br />
Nausea/vomiting<br />
Rash<br />
Fatigue<br />
6<br />
0<br />
4<br />
22.2<br />
0<br />
14.8<br />
1<br />
1<br />
1<br />
3.7<br />
3.7<br />
3.7<br />
0<br />
0<br />
0<br />
0<br />
0<br />
0<br />
7<br />
0<br />
4<br />
25.9<br />
0<br />
14.8<br />
2<br />
0<br />
1<br />
7.4<br />
0<br />
3.7<br />
0<br />
0<br />
0<br />
0<br />
0<br />
0
112 <strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
week <strong>of</strong> the concomitant treatment. During the<br />
adjuvant temozolomide phase, 33.3% <strong>of</strong> patients<br />
required antiemetic therapy. One patient<br />
experienced a treatment-induced rash that<br />
resulted in early discontinuation <strong>of</strong><br />
temozolomide after 7 days <strong>of</strong> CCRT. Moderate<br />
to severe fatigue was reported in 5 patients<br />
during the CCRT phase (grade 3; one patient)<br />
and in 5 patients during the adjuvant<br />
temozolomide phase (grade 3; one patient).<br />
<strong>The</strong> short duration <strong>of</strong> follow-up precludes<br />
definitive assessment <strong>of</strong> late radiation toxicity;<br />
only 9 patients were alive with a follow-up<br />
longer than 24 months. However, signs <strong>of</strong><br />
leukoencephalopathy, without evident clinical<br />
impairment, were apparent on MRI in all <strong>of</strong><br />
these patients. One patient developed<br />
intracranial hypertension, refractory seizures,<br />
and loss <strong>of</strong> vision 25 months after beginning<br />
RT. <strong>The</strong> loss <strong>of</strong> vision may in part be due to<br />
prior RT. Subsequent work-up indicated a spinal<br />
dissemination <strong>of</strong> the disease with positive CSF<br />
cytology and no evidence <strong>of</strong> local recurrence.<br />
A second patient developed neurologic<br />
deterioration with progressive short-term<br />
memory loss and hemiplegia 17 months after<br />
beginning RT. At 26 months, this patient was<br />
still alive without evidence <strong>of</strong> tumor progression.<br />
<strong>The</strong> remaining patients with follow-up longer<br />
than 18 months are doing well without any<br />
clinical signs <strong>of</strong> neurologic impairment.<br />
Thromboembolic events occurred in 3<br />
patients (11.1%). Two patients died <strong>of</strong> cerebral<br />
hemorrhage in the absence <strong>of</strong> a coagulation<br />
disorder or thrombocytopenia.<br />
Survival:<br />
At the time <strong>of</strong> this analysis, 19 patients had<br />
died. <strong>The</strong> median duration <strong>of</strong> follow-up was 17<br />
months, (range, 5-30 months). On the basis <strong>of</strong><br />
Kaplan-Meier estimates, the median overall<br />
survival for the all patients with high grade<br />
gliomas (n=27) was 19 months (95% confidence<br />
interval, 13.58-24.42) (Table 5). About 33.3%<br />
<strong>of</strong> our patients were alive at 2 years, (Table 5).<br />
<strong>The</strong> median progression-free survival was<br />
11 months (95% confidence interval, 8.56-<br />
13.44) (Table 5). <strong>The</strong> two-year progression-free<br />
survival rate was 26.1%.<br />
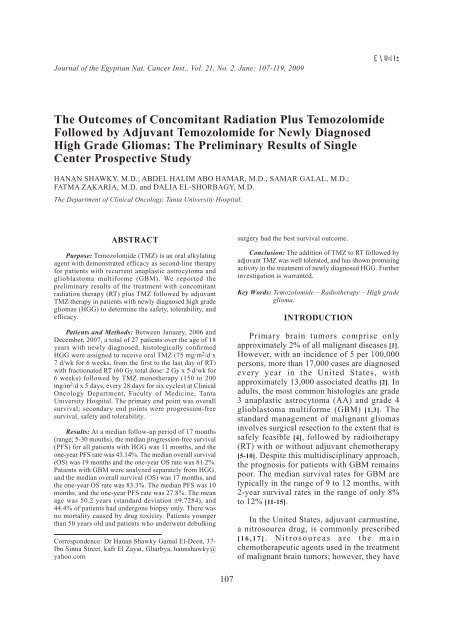
<strong>The</strong> 18 patients with glioblastoma were<br />
analyzed separately from the other patients with<br />
high grade gliomas, and the median overall<br />
survival was 17 months (95% confidence<br />
interval, 13.9-20.1). <strong>The</strong> one-year and two-year<br />
overall survival rate were 83.3% and 38.1%<br />
respectively (Fig. 1).<br />
<strong>The</strong> median progression-free survival for<br />
the 18 patients with glioblastoma was 10 months<br />
(95% confidence interval, 8.99-11.01) (Fig. 2).<br />
<strong>The</strong> six-month progression-free survival rate<br />
was 72.22%.<br />
Prognostic factors:<br />
We analyzed the median overall survival<br />
and survival rates <strong>of</strong> the eligible patient<br />
populations in relation to prognostic indicators.<br />
In patients younger than 50 years old, the median<br />
survival was not reached at 24 months, with<br />
66.7% <strong>of</strong> these patients still alive at 24 months.<br />
In patients 50 years old, the 24 months overall<br />
survival was only 35.7% months (p=0.005),<br />
(Fig. 3). <strong>The</strong> prognosis by surgical respectability<br />
was also analyzed in these eligible patients.<br />
Patients who underwent gross total resection,<br />
near-total removal and subtotal resection had<br />
24 months overall survival <strong>of</strong> 57%. However,<br />
for patients who underwent partial removal or<br />
biopsy, the 24 months overall survival was<br />
26.8% (p=0.0017), (Fig. 4).<br />
As regard to pathological type, the 24 months<br />
overall survival for patients with glioblastoma<br />
and anaplastic astrocytoma (WHO grade III),<br />
was 38.1% and 77.8% respectively (p=0.0025),<br />
(Fig. 5).<br />
Survival according to other possible<br />
prognostic factors were included, Karn<strong>of</strong>sky<br />
Table (5): Overall Survival and progression-free survival<br />
<strong>of</strong> all patients with high grade gliomas (n=27).<br />
Variable<br />
Overall Survival (months):<br />
Median<br />
95% confidence interval<br />
12-month<br />
24-month<br />
Progression-free survival<br />
(months):<br />
Median<br />
95% confidence interval<br />
12-month<br />
24-month<br />
Survival<br />
19.00 months<br />
13.58-24.42 months<br />
81.16%<br />
33.3%<br />
11.00<br />
8.56-13.44 months<br />
43.14%<br />
26.14%
Hanan Shawky, et al. 113<br />
Oveall Survival<br />
1.0<br />
0.8<br />
0.6<br />
0.4<br />
0.2<br />
Survival Function<br />
Censored<br />
Progrssion free Survival<br />
1.0<br />
0.8<br />
0.6<br />
0.4<br />
0.2<br />
Survival Function<br />
Censored<br />
0.0<br />
0 6 12 18 24 30 36<br />
Time (Months)<br />
Fig. (1): Overall survival <strong>of</strong> patients with glioblastoma<br />
(n =18).<br />
1.0<br />
0.8<br />
0.0<br />
0 6 12 18 24 30 36<br />
Time (Months)<br />
Fig. (2): Progression-free survival <strong>of</strong> patients with glioblastoma<br />
(n =18).<br />
1.0<br />
0.8<br />
Oveall Survival<br />
0.6<br />
0.4<br />
0.2<br />
Oveall Survival<br />
0.6<br />
0.4<br />
0.2<br />
0.0<br />
0 6 12 18 24 30 36<br />
Time (Months)<br />
Age<br />
114 <strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
Oveall Survival<br />
1.0<br />
0.8<br />
0.6<br />
0.4<br />
0.2<br />
0.0<br />
0 6 12 18 24 30 36<br />
Time (Months)<br />
Sex<br />
Female<br />
Female-censored<br />
Fig. (7): Overall Survival <strong>of</strong> patients with high grade gliomas<br />
according to sex.<br />
performance status (KPS) (p=
Hanan Shawky, et al. 115<br />
In this study, lymphocytopenia is <strong>of</strong>ten<br />
observed with TMZ treatment but may, in part,<br />
be due to the frequent administration <strong>of</strong><br />
corticosteroids as was described in another<br />
phase I trial [36]. Although lymphocytopenia<br />
occurs frequently, it is not typically associated<br />
with clinical sequelae. However, one <strong>of</strong> the 27<br />
patients we treated with concomitant RT plus<br />
TMZ therapy developed pneumonia. <strong>The</strong><br />
frequency <strong>of</strong> opportunistic infections in a similar<br />
patient population treated with RT alone is<br />
unknown.<br />
Nausea and vomiting, the most frequently<br />
reported non-hematologic adverse events, were<br />
also mild to moderate and could be readily<br />
controlled with the administration <strong>of</strong> standard<br />
antiemetics. Non-hematologic toxicity observed<br />
with temozolomide treatment was in agreement<br />
with the report published by Stupp, et al. [43].<br />
Late toxicity resulting from exposure to<br />
alkylating agents or combined modality<br />
treatment remains a concern. <strong>Concomitant</strong> RT<br />
plus TMZ therapy did not increase late toxicities<br />
associated with RT during our follow-up period;<br />
however, follow-up remains too short to make<br />
any conclusions with regard to late toxicities<br />
resulting from treatment with TMZ.<br />
Some reports <strong>of</strong> concomitant RT plus TMZ<br />
followed by adjuvant TMZ therapy for GBM<br />
were published. In 2005, the efficacy <strong>of</strong><br />
postoperative TMZ radiochemotherapy in<br />
malignant glioma was reported in Germany [65].<br />
According to that report, median PFS time was<br />
7.3 months for primary glioblastoma, treated<br />
with concomitant RT plus TMZ. That study also<br />
reported that the median overall survival time<br />
for patients with glioblastoma was 14.6 months.<br />
Another randomized prospective study <strong>of</strong><br />
concomitant RT plus TMZ was reported in 2005<br />
proving that this protocol is more effective than<br />
RT alone in patients with newly diagnosed<br />
glioblastoma [66]. This randomized study<br />
compared concomitant RT plus TMZ with RT<br />
alone in patients with newly diagnosed<br />
glioblastoma. It reported that the median overall<br />
survival time for patients with glioblastoma<br />
was 14.6 months with RT plus TMZ and 12.1<br />
months with RT alone. <strong>The</strong> 2-year overall<br />
survival rate was 26.5% with RT plus TMZ and<br />
10.4% with RT alone. That study confirmed the<br />
effectiveness <strong>of</strong> concomitant RT plus TMZ for<br />
glioblastoma patients.<br />
Survival results in our study are encouraging.<br />
Indeed, the median PFS time <strong>of</strong> 10 months, the<br />
median overall survival <strong>of</strong> 17 months and the<br />
2-year overall survival rate <strong>of</strong> 38.1% for the 18<br />
patients with glioblastoma in our series treated<br />
with concomitant RT plus TMZ followed by<br />
adjuvant TMZ therapy compares favorably with<br />
the other previous reported protocols. At present<br />
concomitant RT plus TMZ followed by adjuvant<br />
TMZ therapy is widely accepted as the current<br />
standard care for patients with glioblastoma<br />
[23,32,42,44,67-72].<br />
Unlike glioblastoma, there is no definite<br />
consensus about the standard regimen for WHO<br />
grade III gliomas, such as anaplastic astrocytoma<br />
and anaplastic oligodendroglioma. For example,<br />
a phase III trial <strong>of</strong> RT plus chemotherapy using<br />
procarbazine, lomustine and vincristine (PCV)<br />
to treat anaplastic oligodendroglioma was<br />
published in 2006 [73]. This study concluded<br />
that PCV plus RT did not prolong the survival<br />
<strong>of</strong> patients with anaplastic oligodendroglioma<br />
and the longer PFS was associated with<br />
significant toxicity. <strong>The</strong>refore, it is essential to<br />
verify the role <strong>of</strong> TMZ in the treatment WHO<br />
grade III glioma. Since the above-mentioned<br />
landmark study <strong>of</strong> Stupp, et al. [66] in 2005,<br />
there have been many phase II and III clinical<br />
studies <strong>of</strong> the treatment <strong>of</strong> HGG with TMZ in<br />
adults [67,68,74-77]. <strong>The</strong>se trials have reported<br />
good outcomes, and our present results for<br />
patients with WHO grade III and IV gliomas<br />
are also favorable, with tolerable toxicity. In<br />
our study the median PFS time was 11 months,<br />
and the median overall survival was 19 months<br />
for the 27 patients with HGG treated with<br />
concomitant RT plus TMZ followed by adjuvant<br />
TMZ therapy. Our results are consistent with<br />
most <strong>of</strong> these reports, confirming that<br />
concomitant RT plus TMZ followed by adjuvant<br />
TMZ therapy <strong>of</strong>fers good clinical outcomes in<br />
the treatment <strong>of</strong> HGG.<br />
Subanalyses performed to determine the<br />
existence <strong>of</strong> prognostic factors in the patient<br />
population under evaluation revealed that<br />
baseline KPS was an important prognostic factor<br />
that correlated meaningfully with median<br />
survival (p=
116<br />
<strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
substantially better survival rates than patients<br />
who had a biopsy only. <strong>The</strong>se prognostic factors<br />
observed in our patient population under<br />
evaluation were in agreement with the report<br />
published by Stupp, et al. [43].<br />
In conclusion, this is the first report <strong>of</strong> results<br />
<strong>of</strong> concomitant RT plus TMZ followed by<br />
adjuvant TMZ therapy in the treatment <strong>of</strong> HGG<br />
in Clinical Oncology Department, Tanta<br />
University Hospital, Faculty <strong>of</strong> Medicine, Tanta<br />
University, Egypt. This study demonstrated<br />
concomitant RT plus TMZ followed by adjuvant<br />
TMZ therapy, is a promising regimen for<br />
patients with HGG and we propose concomitant<br />
RT plus TMZ followed by adjuvant TMZ<br />
therapy as an alternative approach with tolerable<br />
toxicities for patients with WHO grade III<br />
gliomas, as well as for those with glioblastoma,<br />
nevertheless, the challenge remains to improve<br />
clinical outcomes further. To confirm this, a<br />
multicenter, meta-analysis and a randomized<br />
trial with a large number <strong>of</strong> patients are required<br />
in the near future. Many questions remain<br />
unanswered regarding the applications <strong>of</strong> this<br />
regimen to lower grade gliomas and the optimal<br />
combination <strong>of</strong> radiotherapy and temozolomide.<br />
REFERENCES<br />
1- Wen PY, Kesari S. Malignant Gliomas in Adults.<br />
NEJM. 2008, 359: 492-507.<br />
2- Ries LAG, Eisner MP, Kosary CL, Hankey BF, Miller<br />
BA, Clegg LX, et al. (eds). SEER Cancer Statistics.<br />
2001, 1973-1998. Bethesda, MD, National Cancer<br />
Institute.<br />
3- Kleihues P, Burger PC, Scheithauer BW. <strong>The</strong> new<br />
WHO classification <strong>of</strong> brain tumours. Brain Pathol.<br />
1993, 3: 255-68.<br />
4- Pichlmeier U, Bink A, Schackert G, Stummer W, the<br />
ALA Glioma Study Group. Resection and survival in<br />
glioblastoma multiforme: An RTOG recursive<br />
partitioning analysis <strong>of</strong> ALA study patients. Neurooncol.<br />
2008, 10(6): 1025-34.<br />
5- Sigmond J, Honeywell RJ, Postma TJ, Dirven CMF,<br />
de Lange SM, van der Born K, et al. Gemcitabine<br />
uptake in glioblastoma multiforme: potential as a<br />
radiosensitizer. Ann Oncol. 2009, 20: 182- 7.<br />
6- Vredenburgh JJ, Desjardins A, Reardon DA, Friedman<br />
HS. Experience with irinotecan for the treatment <strong>of</strong><br />
malignant glioma. Neuro Oncol. 2009, 11: 80-91.<br />
7- Stupp R, Hegi ME, van den Bent MJ, Mason WP,<br />
Weller M, Miriman<strong>of</strong>f RO, et al. Changing paradigmsan<br />
update on the multidisciplinary management <strong>of</strong><br />
malignant glioma. Oncologist. 2006, 11(2): 165-80.<br />
8- Gilbert MR. New treatments for malignant gliomas:<br />
careful evaluation and cautious optimism required.<br />
Ann Intern Med. 2006, 144 (5): 371-3.<br />
9- ReardonDA, Rich JN, Friedman HS, Bigner DD.<br />
Recent Advances in the Treatment <strong>of</strong> Malignant<br />
Astrocytoma. J. Clin. Oncol. 2006, 24 (8): 1253-65.<br />
10- Attenello FJ, Mukherjee D, Datoo G, McGirt MJ,<br />
Bohan E, Weingart JD, et al. Use <strong>of</strong> Gliadel (BCNU)<br />
Wafer in the Surgical Treatment <strong>of</strong> Malignant Glioma:<br />
A 10-Year Institutional Experience. Ann. Surg. Oncol.<br />
2008, 15: 2887-93.<br />
11- Galanis E, Buckner J. Chemotherapy for high-grade<br />
gliomas. Br J Cancer. 2000, 82: 1371-80.<br />
12- Levin V, Leibel S, Gutin P. Neoplasms <strong>of</strong> the central<br />
nervous system, in DeVita V Jr, Hellman S, Rosenberg<br />
S (eds): Cancer: Principles and Practice <strong>of</strong> Oncology.<br />
Philadelphia, PA, Lippincott-Raven. 1997, pp 2022-82.<br />
13- DeAngelis LM. Brain tumors. N Engl J Med. 2001,<br />
344: 114-23.<br />
14- Buckner JC. Factors influencing survival in highgrade<br />
gliomas. Semin Oncol. 2003, 30 (19): 10-14.<br />
15- Curran WJ, Scott CB, Horton J, Nelson JS, Weinstein<br />
AS, Fischbach AJ, et al. Recursive partitioning analysis<br />
<strong>of</strong> prognostic factors in three <strong>Radiation</strong> <strong>The</strong>rapy<br />
Oncology Group malignant glioma trials. J Natl Cancer<br />
Inst. 1993, 85: 704-10.<br />
16- Walker MD, Alexander E Jr, Hunt WE, MacCarty CS,<br />
Mahaley MS Jr, Mealey J Jr, et al. Evaluation <strong>of</strong><br />
BCNU and/or radiotherapy in the treatment <strong>of</strong><br />
anaplastic gliomas: a cooperative clinical trial. J<br />
Neurosurg. 1978, 49: 333-43.<br />
17- Walker MD, Green SB, Byar DP, Alexander E,<br />
Batzdorf U, Brooks WH, et al. Randomized<br />
comparisons <strong>of</strong> radiotherapy and nitrosoureas for the<br />
treatment <strong>of</strong> malignant glioma after surgery. N Engl<br />
J Med. 1980, 303 (23): 1323-29.<br />
18- Medical Research Council Brain Tumor Working<br />
Party. Randomized trial <strong>of</strong> procarbazine, lomustine,<br />
and vincristine in the adjuvant treatment <strong>of</strong> high-grade<br />
astrocytoma: a Medical Research Council trial. J Clin<br />
Oncol. 2001, 19: 509-18.<br />
19- Shapiro WR, Green SB, Burger PC, Mahaley MS Jr,<br />
Selker RG, VanGilder JC, et al. Randomized trial <strong>of</strong><br />
three chemotherapy regimens and two radiotherapy<br />
regimens and two radiotherapy regimens in postoperative<br />
treatment <strong>of</strong> malignant glioma: Brain Tumor Cooperative<br />
Group trial 8001. J Neurosurg. 1989, 71: 1-9.<br />
20- Chang CH, Horton J, Schoenfeld D, Salazer O, Perez-<br />
Tamayo R, Kramer S, et al. Comparison <strong>of</strong><br />
postoperative radiotherapy and combined postoperative<br />
radiotherapy and chemotherapy in the multidisciplinary<br />
management <strong>of</strong> malignant gliomas: a joint <strong>Radiation</strong><br />
<strong>The</strong>rapy Oncology Group and Eastern Cooperative<br />
Oncology Group study. Cancer. 1983, 52 (6): 997-<br />
1007.<br />
21- Green SB, Byar DP, Walker MD, Pistenmaa DA,<br />
Alexander E Jr, Batzdorf U, et al. Comparisons <strong>of</strong>
Hanan Shawky, et al. 117<br />
carmustine, procarbazine, and high-dose<br />
methylprednisolone as additions to surgery and<br />
radiotherapy for the treatment <strong>of</strong> malignant glioma.<br />
Cancer Treat Rep. 1983, 67: 121-32.<br />
22- Stupp R, Hegi ME. Recent developments in the<br />
management <strong>of</strong> malignant glioma. In: Perry MC, ed.<br />
ASCO 2003 educational book. Alexandria, Va.:<br />
American Society <strong>of</strong> Clinical Oncology. 2003, 779-<br />
88.<br />
23- Stupp R, Hegi ME, Mason WP, van den Bent MJ,<br />
Taphoorn MJ, Janzer RC, et al. Effects <strong>of</strong> Radiotherapy<br />
with <strong>Concomitant</strong> and Adjuvant <strong>Temozolomide</strong> versus<br />
Radiotherapy alone on survival in Glioblastoma in<br />
a Randomized Phase III study: 5-year Analysis <strong>of</strong> the<br />
EORTC-<strong>NCI</strong>C trial. <strong>The</strong> Lancet Oncology. 2009, 10<br />
(5): 459-66.<br />
24- Herrlinger U, Rieger J, Koch D, Loeser S, Blaschke<br />
B, Kortmann R-D, et al. Phase II Trial <strong>of</strong> Lomustine<br />
<strong>Plus</strong> <strong>Temozolomide</strong> Chemotherapy in Addition to<br />
Radiotherapy in Newly Diagnosed Glioblastoma:<br />
UKT-03. J. Clin. Oncol. 2006, 24 (27): 4412-7.<br />
25- Wick A, Felsberg J, Steinbach JP, Herrlinger U, Platten<br />
M, Blaschke B, et al. Efficacy and Tolerability <strong>of</strong><br />
<strong>Temozolomide</strong> in an Alternating Weekly Regimen in<br />
Patients With Recurrent Glioma. J. Clin. Oncol. 2007,<br />
25 (22): 3357-61.<br />
26- Kesari S, Schiff D, Henson JW, Muzikansky A, Gigas<br />
DC, Doherty L, et al. Phase II study <strong>of</strong> temozolomide,<br />
thalidomide, and celecoxib for newly diagnosed<br />
glioblastoma in adults. Neuro Oncol. 2008, 10:<br />
300-8.<br />
27- Wakabayashi T, Kayama T, Nishikawa R, Takahashi<br />
H, Yoshimine T, Hashimoto N, et al. A Multicenter<br />
Phase I Trial <strong>of</strong> Interferon-{beta} and <strong>Temozolomide</strong><br />
Combination <strong>The</strong>rapy for High-grade Gliomas<br />
(INTEGRA Study). Jpn. J. Clin. Oncol. 2008, 38:<br />
715-8.<br />
28- Brown PD, Krishnan S, Sarkaria JN, Wu W, Jaeckle<br />
KA, Uhm JH, et al. Phase I/II Trial <strong>of</strong> Erlotinib and<br />
<strong>Temozolomide</strong> With <strong>Radiation</strong> <strong>The</strong>rapy in the<br />
Treatment <strong>of</strong> Newly Diagnosed Glioblastoma<br />
Multiforme: North Central Cancer Treatment Group<br />
Study N0177 J. Clin. Oncol. 2008, 26: 5603-9.<br />
29- Prados MD, Chang SM, Butowski N, DeBoer R,<br />
Parvataneni R, Carliner H, et al. Phase II Study <strong>of</strong><br />
Erlotinib <strong>Plus</strong> <strong>Temozolomide</strong> During and After<br />
<strong>Radiation</strong> <strong>The</strong>rapy in Patients With Newly Diagnosed<br />
Glioblastoma Multiforme or Gliosarcoma. J. Clin.<br />
Oncol. 2009, 27: 579-84.<br />
30- van den Bent MJ, Brandes AA, Rampling R,<br />
Kouwenhoven MCM, Kros JM, Carpentier AF, et al.<br />
Randomized Phase II Trial <strong>of</strong> Erlotinib Versus<br />
<strong>Temozolomide</strong> or Carmustine in Recurrent<br />
Glioblastoma: EORTC Brain Tumor Group Study<br />
26034. J. Clin. Oncol. 2009, 27: 1268-74.<br />
31- Glas M, Happold C, Rieger J, Wiewrodt D, Bahr O,<br />
Steinbach JP, et al. Long-Term Survival <strong>of</strong> Patients<br />
With Glioblastoma Treated With Radiotherapy and<br />
Lomustine <strong>Plus</strong> <strong>Temozolomide</strong>. J. Clin. Oncol. 2009,<br />
27: 1257-61.<br />
32- Beier D, Rohrl S, Pillai DR, Schwarz S, Kunz-<br />
Schughart L A, Leukel P, et al. <strong>Temozolomide</strong><br />
Preferentially Depletes Cancer Stem Cells in<br />
Glioblastoma. Cancer Res. 2008, 68: 5706-15.<br />
33- Newlands ES, Blackledge GR, Slack JA, Rustin GJ,<br />
Smith DB, Stuart NS, et al. Phase I trial <strong>of</strong><br />
temozolomide (CCRG 81045: M&B 39831: NSC<br />
362856). Br J Cancer. 1992, 65: 287-91.<br />
34- Marzolini C, Decosterd LA, Shen F, Gander M,<br />
Leyvraz S, Bauer J, et al. Pharmacokinetics <strong>of</strong><br />
temozolomide in association with fotemustine in<br />
malignant melanoma and malignant glioma patients:<br />
Comparison <strong>of</strong> oral, intravenous, and hepatic intraarterial<br />
administration. Cancer Chemother Pharmacol.<br />
1998, 42: 433-40.<br />
35- Stupp R, Ostermann S, Leyvraz S, Csajka C, Buclin<br />
T. Cerebrospinal fluid levels <strong>of</strong> temozolomide as a<br />
surrogate marker for brain penetration. Proc Am Soc<br />
Clin Oncol. 2001, 20: 59a, (abstr 232).<br />
36- Brock CS, Newlands ES, Wedge SR, Bower M, Evans<br />
H, Colquhoun I, et al. Phase I trial <strong>of</strong> temozolomide<br />
using an extended continuous oral schedule. Cancer<br />
Res. 1998, 58: 4363-7.<br />
37- Tolcher AW, Gerson SL, Denis L, Geyer C, Hammond<br />
LA, Patnaik A, et al. Marked inactivation <strong>of</strong> O6-<br />
alkylguanine-DNA alkyltransferase activity with<br />
protracted temozolomide schedules. Br J Cancer.<br />
2003, 88: 1004-11.<br />
38- Hegi ME, Liu L, Herman JG, Stupp R, Wick W, Weller<br />
M, et al. Correlation <strong>of</strong> O6-Methylguanine<br />
Methyltransferase (MGMT) Promoter Methylation<br />
With Clinical <strong>Outcomes</strong> in Glioblastoma and Clinical<br />
Strategies to Modulate MGMT Activity. J. Clin.<br />
Oncol.2008, 26 (25): 4189-99.<br />
39- Brandes AA, Franceschi E, Tosoni A, Blatt V, Pession<br />
A, Tallini G, et al. MGMT Promoter Methylation<br />
Status Can Predict the Incidence and Outcome <strong>of</strong><br />
Pseudoprogression After <strong>Concomitant</strong><br />
Radiochemotherapy in Newly Diagnosed Glioblastoma<br />
Patients. J. Clin. Oncol. 2008, 26 (13): 2192-7.<br />
40- Esteller M, Garcia-Foncillas J, Andion E, Goodman<br />
SN, Hidalgo OF, Vanaclocha V, et al. Inactivation <strong>of</strong><br />
the DNA-repair gene MGMT and the clinical response<br />
<strong>of</strong> gliomas to alkylating agents. N Engl J Med. 2000,<br />
343: 1350-4. [Erratum, N Engl J Med. 2000, 343:<br />
1740].<br />
41- Hegi ME, Diserens AC, Godard S, Dietrich P-Y, Regli<br />
L, Ostermann S, et al. Clinical trial substantiates the<br />
predictive value <strong>of</strong> O-6-methylguanine-DNA<br />
methyltransferase promoter methylation in<br />
glioblastoma patients treated with temozolomide. Clin<br />
Cancer Res. 2004, 10: 1871-4.<br />
42- Chakravarti A, Erkkinen MG, Nestler U, Stupp R,<br />
Mehta M, Aldape K, et al. <strong>Temozolomide</strong>-Mediated<br />
<strong>Radiation</strong> Enhancement in Glioblastoma: A Report<br />
on Underlying Mechanisms. Clin. Cancer Res. 2006,<br />
12 (15): 4738-46.<br />
43- Stupp R, Dietrich P-Y, Ostermann Kraljevic S, Pica<br />
A, Maillard I, Maeder P, et al. Promising survival for
118<br />
<strong>The</strong> <strong>Outcomes</strong> <strong>of</strong> <strong>Concomitant</strong> <strong>Radiation</strong> <strong>Plus</strong> <strong>Temozolomide</strong><br />
patients with newly diagnosed glioblastoma<br />
multiforme treated with concomitant radiation plus<br />
temozolomide followed by adjuvant temozolomide.<br />
J Clin Oncol. 2002, 20 (5): 1375- 82.<br />
44- Miriman<strong>of</strong>f RO, Gorlia T, Mason W, Van den Bent<br />
MJ, Kortmann RD, Fisher B, et al. Radiotherapy and<br />
<strong>Temozolomide</strong> for Newly Diagnosed Glioblastoma:<br />
Recursive Partitioning Analysis <strong>of</strong> the EORTC<br />
26981/22981-<strong>NCI</strong>C CE3 Phase III Randomized Trial.<br />
J. Clin. Oncol. 2006, 24 (16): 2563-9.<br />
45- Macdonald DR, Cascino TL, Schold SC Jr, Cairncross<br />
JG. Response criteria for phase II studies <strong>of</strong> supratentorial<br />
malignant glioma. J Clin Oncol. 1990, 8: 1277-80.<br />
46- Kaplan EL, Meier P. Nonparametric estimation from<br />
incomplete observations. J Am Stat Assoc. 1958, 53:<br />
457-81.<br />
47- Kristiansen K, Hagen S, Kollevold T, Torvik A, Holme<br />
I, Nesbakken R, et al. Combined modality therapy <strong>of</strong><br />
operated astrocytomas grade III and IV: Confirmation<br />
<strong>of</strong> the value <strong>of</strong> postoperative irradiation and lack <strong>of</strong><br />
potentiation <strong>of</strong> bleomycin on survival time-A<br />
prospective multicenter trial <strong>of</strong> the Scandinavian<br />
Glioblastoma Study Group. Cancer. 1981, 47: 649-<br />
52.<br />
48- Shapiro WR. Chemotherapy <strong>of</strong> malignant gliomas:<br />
studies <strong>of</strong> the BTCG. Rev Neurol. 1992, 148: 428-<br />
34.<br />
49- Grossman SA, O'Neill A, Grunnet M, Mehta M,<br />
Pearlman JL, Wagner H, et al. Phase III study<br />
comparing three cycles <strong>of</strong> infusional carmustine and<br />
cisplatin followed by radiation therapy with radiation<br />
therapy and concurrent carmustine in patients with<br />
newly diagnosed supratentorial glioblastoma<br />
multiforme: Eastern Cooperative Oncology Group<br />
Trial 2394. J Clin Oncol. 2003, 21: 1485-91.<br />
50- Deutsch M, Green SB, Strike TA, Burger PC,<br />
Robertson JT, Selker RG, et al. Results <strong>of</strong> a randomized<br />
trial comparing BCNU plus radiotherapy,<br />
streptozotocin plus radiotherapy, BCNU plus<br />
hyperfractionated radiotherapy, and BCNU following<br />
misonidazole plus radiotherapy in the postoperative<br />
treatment <strong>of</strong> malignant glioma. Int J Radiat Oncol<br />
Biol Phys. 1989, 16: 1389-96.<br />
51- Fisher BJ, Scott C, Macdonald DR, Coughlin C, Curran<br />
WJ. Phase I study <strong>of</strong> topotecan plus cranial radiation<br />
for glioblastoma multiforme: Results <strong>of</strong> <strong>Radiation</strong><br />
<strong>The</strong>rapy Oncology Group Trial 9507. J Clin Oncol.<br />
2001, 19: 1111-7.<br />
52- Del Rowe J, Scott C, Werner-Wasik M, Bahary JP,<br />
Curran WJ, Urtasun RC, et al. Single-arm, open-label<br />
phase II study <strong>of</strong> intravenously administered<br />
tirapazamine and radiation therapy for glioblastoma<br />
multiforme. J Clin Oncol. 2000, 18: 1254-9.<br />
53- Kleinberg L, Grossman SA, Piantadosi S, Zeltzman<br />
M, Wharam M. <strong>The</strong> effects <strong>of</strong> sequential versus<br />
concurrent chemotherapy and radiotherapy on survival<br />
and toxicity in patients with newly diagnosed highgrade<br />
astrocytoma. Int J Radiat Oncol Biol Phys.<br />
1999, 44: 535-43.<br />
54- Brem H, Piantadosi S, Burger PC, Walker M, Selker<br />
R, Vick NA, et al. Placebo-controlled trial <strong>of</strong> safety<br />
and efficacy <strong>of</strong> intraoperative controlled delivery by<br />
biodegradable polymers <strong>of</strong> chemotherapy for recurrent<br />
gliomas: <strong>The</strong> Polymer-Brain Tumor Treatment Group.<br />
Lancet. 1995, 345: 1008-12.<br />
55- Westphal M, Hilt DC, Bortey E, Delavault P, Olivares<br />
R, Warnke PC, et al. A phase 3 trial <strong>of</strong> local<br />
chemotherapy with biodegradable carmustine (BCNU)<br />
wafers (Gliadel wafers) in patients with primary<br />
malignant glioma. Neuro-Oncology. 2003, 5 (2): 79-<br />
88.<br />
56- Friedman HS, Kerby T, Calvert H. <strong>Temozolomide</strong> and<br />
treatment <strong>of</strong> malignant glioma. Clin Cancer Res. 2000,<br />
6: 2585-97.<br />
57- Reid JM, Stevens DC, Rubin J, Ames MM.<br />
Pharmacokinetics <strong>of</strong> 3-methyl-(triazen-1-yl)imidazole-<br />
4-carboximide following administration <strong>of</strong><br />
temozolomide to patients with advanced cancer. Clin<br />
Cancer Res. 1997, 3: 2393-8.<br />
58- van den Bent MJ, Taphoorn MJB, Brandes AA, Menten<br />
J, Stupp R, Frenay M, et al. Phase II Study <strong>of</strong> First-<br />
Line Chemotherapy With <strong>Temozolomide</strong> in Recurrent<br />
Oligodendroglial Tumors: <strong>The</strong> European Organization<br />
for Research and Treatment <strong>of</strong> Cancer Brain Tumor<br />
Group Study 26971. J. Clin. Oncol. 2003, 21 (13):<br />
2525-8.<br />
59- Newlands ES, Stevens MFG, Wedge SR, Wheelhouse<br />
RT, Brock C. <strong>Temozolomide</strong>: a review <strong>of</strong> its discovery,<br />
chemical properties, pre-clinical development and<br />
clinical trials. Cancer Treat Rev. 1997, 23: 35-61.<br />
60- Stupp R, Gander M, Leyvraz S, Newlands E. Current<br />
and future developments in the use <strong>of</strong> temozolomide<br />
for the treatment <strong>of</strong> brain tumours. Lancet Oncol,<br />
2001;2: 552 - 60.<br />
61- Khan RB, Raizer JJ, Malkin MG, Bazylewicz KA,<br />
Abrey LE. A phase II study <strong>of</strong> extended low-dose<br />
temozolomide in recurrent malignant gliomas. Neurooncol.<br />
2002, 4 (1): 39 - 43.<br />
62- Yung WK, Prados MD, Yaya-Tur R, Rosenfeld SS,<br />
Brada M, Friedman HS, et al. Multicenter phase II<br />
trial <strong>of</strong> temozolomide in patients with anaplastic<br />
astrocytoma or anaplastic oligoastrocytoma at first<br />
relapse. J Clin Oncol. 1999, 17 (9): 2762- 71.<br />
63- Yung WK, Albright RE, Olson J, Fredericks R, Fink<br />
K, Prados MD, et al. A phase II study <strong>of</strong> temozolomide<br />
vs. procarbazine in patients with glioblastoma<br />
multiforme at first relapse. Br J Cancer. 2000, 83:<br />
588- 93.<br />
64- Brada M, Hoang-Xuan K, Rampling R, Dietrich P-Y,<br />
Dirix LY, Macdonald D, et al. Multicenter phase II<br />
trial <strong>of</strong> temozolomide in patients with glioblastoma<br />
multiforme at first relapse. Ann Oncol. 2001, 12: 259-<br />
66.<br />
65- Kocher M, Kunze S, Eich HT, Semrau R, Muller RP.<br />
Efficacy and toxicity <strong>of</strong> postoperative temozolomide<br />
radiochemotherapy in malignant glioma. Strahlenther<br />
Onkol. 2005, 181: 157-63.
Hanan Shawky, et al. 119<br />
66- Stupp R, Mason WP, van den Bent MJ, Weller M,<br />
Fisher B, Taphoorn MJ, et al. Radiotherapy plus<br />
<strong>Concomitant</strong> and Adjuvant <strong>Temozolomide</strong> for<br />
Glioblastoma. N Engl J Med. 2005, 352: 987-96.<br />
67- Stupp R, Hegi ME, Gilbert MR, Chakravarti A.<br />
Chemoradiotherapy in Malignant Glioma: Standard<br />
<strong>of</strong> Care and Future Directions. J. Clin. Oncol. 2007,<br />
25 (26): 4127-36.<br />
68- Perry J, Laperriere N, Zuraw L, Chmbers A, Spith<strong>of</strong>f<br />
K, Cairncross JG. Adjuvant chemotherapy for adults<br />
with malignant glioma: a systemic review. Can J<br />
Neurol Sci. 2007, 34: 402-10.<br />
69- Sathornsumetee S, Rich JN and Reardon DA. Diagnosis<br />
and treatment <strong>of</strong> high-grade astrocytoma. Neurol Clin.<br />
2007, 25: 1111-39.<br />
70- Cohen MH, Johnson JR and Pazdur R. Food and Drug<br />
Administration Drug Approval Summary:<br />
<strong>Temozolomide</strong> <strong>Plus</strong> <strong>Radiation</strong> <strong>The</strong>rapy for the<br />
Treatment <strong>of</strong> Newly Diagnosed Glioblastoma<br />
Multiforme. Clin. Cancer Res. 2005, 11 (19): 6767-<br />
71.<br />
71- Athanassiou H, Synodinou M, Maragoudakis E,<br />
Paraskevaidis M, Verigos C, Misailidou D, et al.<br />
Randomized Phase II Study <strong>of</strong> <strong>Temozolomide</strong> and<br />
Radiotherapy Compared With Radiotherapy Alone in<br />
Newly Diagnosed Glioblastoma Multiforme. J. Clin.<br />
Oncol. 2005, 23 (10): 2372-7.<br />
72- Glas M, Happold C, Rieger J, Wiewrodt D, Bahr O,<br />
Steinbach JP, et al. Long-Term Survival <strong>of</strong> Patients<br />
With Glioblastoma Treated With Radiotherapy and<br />
Lomustine <strong>Plus</strong> <strong>Temozolomide</strong>. J. Clin. Oncol. 2009,<br />
27: 1257-61.<br />
73- Cairncross G, Berkey B, Shaw E, Jenkins R,<br />
Scheithauer B, Brachman D, et al. Phase III trial <strong>of</strong><br />
chemotherapy plus radiotherapy compared with<br />
radiotherapy alone for pure and mixed anaplastic<br />
oligodendroglioma: Intergroup <strong>Radiation</strong> <strong>The</strong>rapy<br />
Oncology Group Trial 9402. J Clin Oncol. 2006, 24:<br />
2707-14.<br />
74- Corsa P, Parisi S, Raguso A, Troiano M, Perrone A,<br />
Cossa S, et al.. <strong>Temozolomide</strong> and Radiotherapy as<br />
first-line treatment <strong>of</strong> high-grade gliomas. Tumori.<br />
2006, 92: 299-305.<br />
75- Oshiro OS, Tsugu H, Komatsu F, Ohmura T, Ohta M,<br />
Sakamoto S, et al. Efficacy <strong>of</strong> <strong>Temozolomide</strong><br />
Treatment in Patients with High-grade Glioma.<br />
Anticancer Res. 2009, 29: 911-7.<br />
76- Wick W, Platten M and Weller M. New (alternative)<br />
temozolomide regimens for the treatment <strong>of</strong> glioma.<br />
Neuro-oncol, 2009, 11 (1): 69-79.<br />
77- Vogelbaum MA, Berkey B, Peereboom D, Macdonald<br />
D, Giannini C, Suh JH, et al. Phase II trial <strong>of</strong><br />
preirradiation and concurrent temozolomide in patients<br />
with newly diagnosed anaplastic oligodendrogliomas<br />
and mixed anaplastic oligoastrocytomas: RTOG<br />
BR0131. Neuro Oncol. 2009, 11: 167-75.













