Abnormal Case of Breast Hypertrophy - ePlasty
Abnormal Case of Breast Hypertrophy - ePlasty
Abnormal Case of Breast Hypertrophy - ePlasty

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Interesting <strong>Case</strong> Series<br />
<strong>Abnormal</strong> <strong>Case</strong> <strong>of</strong> <strong>Breast</strong> <strong>Hypertrophy</strong><br />
Ian Hoppe, BA a , and David Bleich, MD b<br />
a Department <strong>of</strong> Surgery, Division <strong>of</strong> Plastic Surgery, New Jersey Medical School—UMDNJ,<br />
Newark; and b Department <strong>of</strong> Medicine, Division <strong>of</strong> Endocrinology, New Jersey Medical<br />
School—UMDNJ, Newark<br />
Correspondence: hoppeic@umdnj.edu<br />
DESCRIPTION<br />
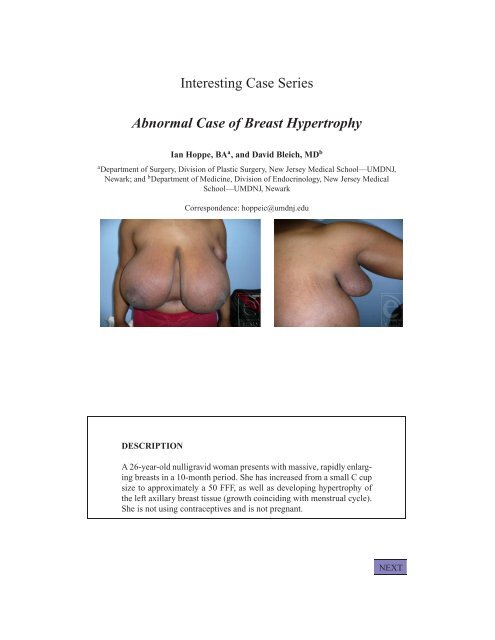
A 26-year-old nulligravid woman presents with massive, rapidly enlarging<br />
breasts in a 10-month period. She has increased from a small C cup<br />
size to approximately a 50 FFF, as well as developing hypertrophy <strong>of</strong><br />
the left axillary breast tissue (growth coinciding with menstrual cycle).<br />
She is not using contraceptives and is not pregnant.<br />
NEXT
QUESTIONS<br />
1. What is the differential diagnosis <strong>of</strong> this condition?<br />
2. What test(s) is appropriate?<br />
3. What surgical approach is appropriate?<br />
4. How should this patient be managed postoperatively?<br />
BACK<br />
NEXT
DISCUSSION<br />
Differential diagnoses for this case include juvenile fibroadenoma,<br />
virginal hypertrophy, fibrocystic disease, and cystosarcoma phylloides.<br />
This patient had no palpable masses and both breasts as well as the<br />
axillary tail <strong>of</strong> the breast were massively hypertrophic suggesting<br />
virginal hypertrophy.<br />
A very rare condition, virginal hypertrophy, is thought to be due<br />
to end-organ (breast) hypersensitivity to gonadal hormones. Virginal<br />
hypertrophy is a differential diagnosis. A serum estrogen and gonadotrophin<br />
assay should be conducted as well as a measurement <strong>of</strong><br />
urinary 17-keto and hydroxysteroid levels. These tests will give normal<br />
results in virginal hypertrophy, ruling out malignancy <strong>of</strong> adrenal,<br />
pituitary, or ovarian origin. A mammogram will not demonstrate malignancy.<br />
On the basis <strong>of</strong> these findings, along with the timing <strong>of</strong> the<br />
breast growth (coinciding with menstrual cycle) and the presence <strong>of</strong><br />
the axillary breast tail, a diagnosis <strong>of</strong> virginal hypertrophy is strongly<br />
supported.<br />
In this patient a keyhole pattern breast reduction and free nipple areola<br />
graft was most appropriate. Because <strong>of</strong> the large size <strong>of</strong> the breasts any<br />
<strong>of</strong> the pedicled options could not adequately reduce the breast size. The<br />
axillary breast was directly excised.<br />
There have been reports <strong>of</strong> breast regrowth after reduction,<br />
necessitating a second reduction surgery. Hormone therapy is a possible<br />
postoperative option to prevent recurrent breast growth. Medroxyprogesterone<br />
inhibits luteinizing hormone as well as exerts some<br />
antiestrogen activity. Possible disadvantages <strong>of</strong> this treatment include<br />
amenorrhea and interruption <strong>of</strong> ovulation. Tamoxifen is a selective estrogen<br />
receptor modulator that has been shown to arrest breast growth<br />
and to reduce breast size in some instances. It can be used postoperatively<br />
to prevent breast growth in cases <strong>of</strong> virginal hypertrophy.<br />
BACK<br />
NEXT
REFERENCES<br />
De Silva NK, Brandt ML. Disorders <strong>of</strong> the breast in children and adolescents, part 1: disorders <strong>of</strong> growth<br />
and infections <strong>of</strong> the breast. J Pediatr Adolesc Gynecol. 2006;19:345–9.<br />
Kreithen J, Caffee H, Rosenberg J, et al. A comparison <strong>of</strong> the LeJour and Wise pattern methods <strong>of</strong> breast<br />
reduction. Ann Plast Surg. 2005;54:235–41.<br />
Özerdem ÖR, Anlatici R, Maral T, Demiralay A. Modified free nipple graft reduction mammaplasty to<br />
increase breast projection with superior and inferior dermoglandular flaps. Ann Plastic Surg.<br />
2002;49:506–10.<br />
Pülzl P, Schoeller T, Tzankov A, Wechselberger G. Unilateral breast enlargement 5 years after reduction<br />
mammaplasty. Aesthetic Plast Surg. 2005;29:404–6.<br />
van Wingerden JJ. Avoiding free nipple grafting in gigantomastia with the inferior pedicle technique. Ann<br />
Plast Surg. 2006;56:465–6.<br />
Wilmink H, Spauween P, Hartman E, Hendriks J, Koeijers V. Preoperative injection using a diluted<br />
anesthethic/adrenaline solution significantly reduces blood loss in reduction mammaplasty. Plast<br />
Reconstruct Surg. 1998;102:373–6.<br />
BACK