2012 Benefit Enrollment Guide - Education Management Corporation
2012 Benefit Enrollment Guide - Education Management Corporation
2012 Benefit Enrollment Guide - Education Management Corporation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
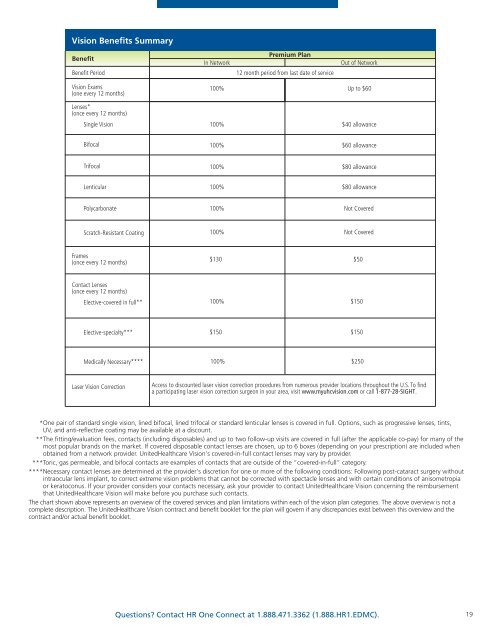
Vision <strong>Benefit</strong>s Summary<br />
<strong>Benefit</strong><br />
<strong>Benefit</strong> Period<br />
In Network<br />
Premium Plan<br />
12 month period from last date of service<br />
Out of Network<br />
Vision Exams<br />
(one every 12 months)<br />
100%<br />
Up to $60<br />
Lenses*<br />
(once every 12 months)<br />
Single Vision<br />
100% $40 allowance<br />
Bifocal<br />
100% $60 allowance<br />
Trifocal<br />
100% $80 allowance<br />
Lenticular<br />
100%<br />
$80 allowance<br />
Polycarbonate<br />
100%<br />
Not Covered<br />
Scratch-Resistant Coating<br />
100%<br />
Not Covered<br />
Frames<br />
(once every 12 months)<br />
$130 $50<br />
Contact Lenses<br />
(once every 12 months)<br />
Elective-covered in full**<br />
100%<br />
$150<br />
Elective-specialty***<br />
$150 $150<br />
Medically Necessary****<br />
100%<br />
$250<br />
Laser Vision Correction<br />
Access to discounted laser vision correction procedures from numerous provider locations throughout the U.S. To find<br />
a participating laser vision correction surgeon in your area, visit www.myuhcvision.com or call 1-877-28-SIGHT.<br />
****One pair of standard single vision, lined bifocal, lined trifocal or standard lenticular lenses is covered in full. Options, such as progressive lenses, tints,<br />
UV, and anti-reflective coating may be available at a discount.<br />
****The fitting/evaluation fees, contacts (including disposables) and up to two follow-up visits are covered in full (after the applicable co-pay) for many of the<br />
most popular brands on the market. If covered disposable contact lenses are chosen, up to 6 boxes (depending on your prescription) are included when<br />
obtained from a network provider. UnitedHealthcare Vision’s covered-in-full contact lenses may vary by provider.<br />
****Toric, gas permeable, and bifocal contacts are examples of contacts that are outside of the “covered-in-full” category.<br />
****Necessary contact lenses are determined at the provider’s discretion for one or more of the following conditions: Following post-cataract surgery without<br />
intraocular lens implant, to correct extreme vision problems that cannot be corrected with spectacle lenses and with certain conditions of anisometropia<br />
or keratoconus. If your provider considers your contacts necessary, ask your provider to contact UnitedHealthcare Vision concerning the reimbursement<br />
that UnitedHealthcare Vision will make before you purchase such contacts.<br />
The chart shown above represents an overview of the covered services and plan limitations within each of the vision plan categories. The above overview is not a<br />
complete description. The UnitedHealthcare Vision contract and benefit booklet for the plan will govern if any discrepancies exist between this overview and the<br />
contract and/or actual benefit booklet.<br />
Questions? Contact HR One Connect at 1.888.471.3362 (1.888.HR1.EDMC).<br />
19