Dental â Low Plan (Maximum Allowable Charge ... - Midlothian ISD
Dental â Low Plan (Maximum Allowable Charge ... - Midlothian ISD
Dental â Low Plan (Maximum Allowable Charge ... - Midlothian ISD

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
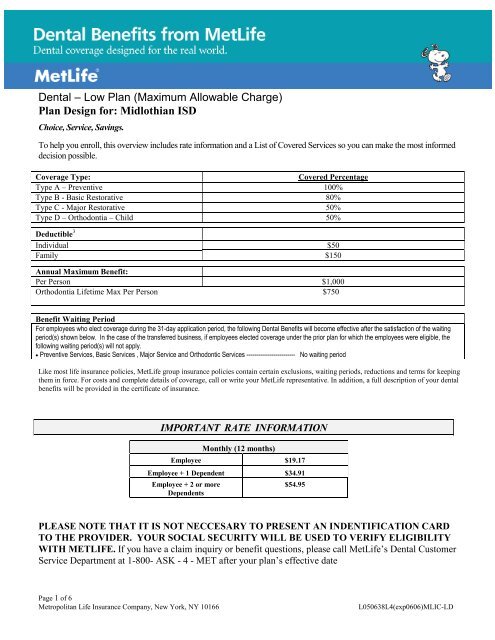
<strong>Dental</strong> – <strong>Low</strong> <strong>Plan</strong> (<strong>Maximum</strong> <strong>Allowable</strong> <strong>Charge</strong>)<br />
<strong>Plan</strong> Design for: <strong>Midlothian</strong> <strong>ISD</strong><br />
Choice, Service, Savings.<br />
To help you enroll, this overview includes rate information and a List of Covered Services so you can make the most informed<br />
decision possible.<br />
Coverage Type:<br />
Covered Percentage<br />
Type A – Preventive 100%<br />
Type B - Basic Restorative 80%<br />
Type C - Major Restorative 50%<br />
Type D – Orthodontia – Child 50%<br />
Deductible 3<br />
Individual $50<br />
Family $150<br />
Annual <strong>Maximum</strong> Benefit:<br />
Per Person $1,000<br />
Orthodontia Lifetime Max Per Person $750<br />
Benefit Waiting Period<br />
For employees who elect coverage during the 31-day application period, the following <strong>Dental</strong> Benefits will become effective after the satisfaction of the waiting<br />
period(s) shown below. In the case of the transferred business, if employees elected coverage under the prior plan for which the employees were eligible, the<br />
following waiting period(s) will not apply.<br />
• Preventive Services, Basic Services , Major Service and Orthodontic Services ------------------------- No waiting period<br />
Like most life insurance policies, MetLife group insurance policies contain certain exclusions, waiting periods, reductions and terms for keeping<br />
them in force. For costs and complete details of coverage, call or write your MetLife representative. In addition, a full description of your dental<br />
benefits will be provided in the certificate of insurance.<br />
IMPORTANT RATE INFORMATION<br />
Monthly (12 months)<br />
Employee $19.17<br />
Employee + 1 Dependent $34.91<br />
Employee + 2 or more<br />
Dependents<br />
$54.95<br />
PLEASE NOTE THAT IT IS NOT NECCESARY TO PRESENT AN INDENTIFICATION CARD<br />
TO THE PROVIDER. YOUR SOCIAL SECURITY WILL BE USED TO VERIFY ELIGIBILITY<br />
WITH METLIFE. If you have a claim inquiry or benefit questions, please call MetLife’s <strong>Dental</strong> Customer<br />
Service Department at 1-800- ASK - 4 - MET after your plan’s effective date<br />
Page 1 of 6<br />
Metropolitan Life Insurance Company, New York, NY 10166<br />
L050638L4(exp0606)MLIC-LD
Type A – Preventive<br />
Oral Exams<br />
Oral Exams-Problem Focused<br />
Full Mouth X-Rays<br />
Periapical X-Rays<br />
Other X-Rays<br />
Bitewing X-Rays<br />
Prophylaxis / Cleanings<br />
Fluoride Treatments<br />
Sealants<br />
Type B – Basic Restorative<br />
Labs & Other Tests<br />
Space Maintainers<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
List of Covered Services & Limitations*<br />
How Many/How Often:<br />
Oral exams (including problem focused) but not more than 1 time in 6 months.<br />
Full mouth or Panoramic X-rays but not more than once every 5 calendar years.<br />
Bitewing X-rays 1 time in 12 months for a child under 14; and 1 time in 12 months for everyone else.<br />
Cleaning of teeth (oral prophylaxis) 1 time in 6 months.<br />
Topical fluoride treatment for a child under age 13, 1 time in 1 calendar year.<br />
Sealants for a child under age 13, which are applied to non-restored, non-decayed first and second<br />
permanent molars once per tooth in 60 months<br />
How Many/How Often:<br />
Space Maintainers limited to one per lifetime per area for a child under 14 years of age.<br />
<br />
Fillings<br />
<br />
<br />
Amalgam or Resin Composite filling replacements if at least 24 months have passed since the existing<br />
filling was placed; or a new surface of decay is identified on that tooth.<br />
Adjustments of dentures if at least 6 months have passed since the installation of the denture and not<br />
more than once in any 12 month period.<br />
<br />
<br />
<br />
<br />
<br />
Rebases / Relines<br />
Simple Extractions<br />
Surgical Extractions<br />
Oral Surgery<br />
Emergency Palliative<br />
Treatment<br />
<br />
<br />
Relining and Rebasing of existing removable dentures: if at least 6 months have passed since the<br />
installation; and not more than once in any 36 month period.<br />
Tissue Conditioning, but not more than 1 time in 36 months.<br />
Type C - Major Restorative<br />
How Many/How Often:<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Cone Beam Imaging<br />
Crowns<br />
Inlays / Onlays<br />
Prefabricated Stainless Steel<br />
and Resin Crowns<br />
Recementations<br />
Crown Build-ups / Post & Core<br />
Repairs<br />
Root Canal<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Cone Beam Imaging but not more than once for the same tooth position in any 60 month period.<br />
Initial installation of Cast Restorations (inlays, onlays, crowns).<br />
- Replacement of any Cast Restorations with the same or a different type of Cast Restoration but<br />
not more than one replacement for the same tooth surface within 10 calendar years of a prior<br />
replacement.<br />
Prefabricated stainless steel crowns or prefabricated resin crowns, but not more than one replacement<br />
for the same tooth surface within any 10 calendar year period.<br />
Recementation of Crowns, Inlays, Onlays, Dentures and Bridgework is limited to 1 time in 12 months.<br />
Crown Buildups / Post and Core but no more than once per tooth in a period of 10 calendar years.<br />
Repairs to Crowns, Inlays, Onlays, Dentures and Bridgework are limited to 1 time in 12 months.<br />
Root canal treatment not more often than once per lifetime for the same tooth.<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Periodontal Surgery<br />
Periodontal Surgery - Soft and<br />
Connective Tissue Grafts<br />
Periodontics – Non-Surgical<br />
Periodontal Maintenance<br />
Dentures<br />
Fixed Bridges<br />
General Anesthesia<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Periodontal surgery not mentioned elsewhere, including gingivectomy, gingivoplasty, gingival curettage,<br />
and osseous surgery, but no more than one surgical procedure per quadrant in any 36 month period.<br />
Periodontal Soft or Connective Tissue Grafts, but no more than one surgical procedure per quadrant in<br />
any 36 month period.<br />
Periodontal scaling and root planing but not more than once per quadrant in any 24 month period.<br />
Periodontal Maintenance: Where periodontal treatment (including scaling, root planing and periodontal<br />
surgery such as gingivectomy, gingivoplasty, osseous surgery) has been performed. Periodontal<br />
maintenance is limited to 2 times in any year less the number of teeth cleanings received during such<br />
12 month period.<br />
Replacement of a non-serviceable removable partial denture, removable full denture or fixed bridgework<br />
if installed more than 10 calendar years prior to replacement.<br />
Initial installation of fixed bridgework, a partial removable denture or a full removable denture when<br />
needed to replace congenitally missing teeth or to replace natural teeth lost while this dental insurance<br />
coverage is in effect.<br />
Administration of general anesthesia or intravenous sedation in connection with oral surgery,<br />
extractions, or other covered services, when dentally necessary as determined by Metropolitan in terms<br />
of generally accepted dental standards.<br />
<br />
<br />
<br />
Consultations<br />
Occlusal Adjustments<br />
Implants<br />
<br />
<br />
Consultations, but not more than 1 time in a 12 month period.<br />
Occlusal Adjustments, but not more than 1 time in a 12 month period.<br />
Type D – Orthodontia<br />
• All dental procedures performed in connection with orthodontic treatment are payable as Orthodontia<br />
• Payments are on a repetitive basis.
<strong>Midlothian</strong> <strong>ISD</strong> - MAC Fees<br />
PROCEDURE<br />
GENERALIST<br />
CODE DESCRIPTION PDP FEE<br />
00120 PERIODIC ORAL EXAMINATION $25<br />
00140 LTD ORAL EVALUATION - PROBLEM FOCUS $37<br />
00150 COMP ORAL EVALUATION - NEW/EST PT $35<br />
00180 COMP PERIODONTAL EVAL - NEW/EST PT $39<br />
00210 INTRAORAL-COMPLETE SERIES $73<br />
00220 INTRAORAL PERIAPICAL FIRST FILM $14<br />
00230 INTRAORL PERIAPICAL EA ADD FILM $6<br />
00240 OCCLUSAL XRAY $23<br />
00270 BITEWING - SINGLE FILM $14<br />
00272 BITEWINGS - TWO FILMS $22<br />
00274 BITEWINGS - FOUR FILMS $29<br />
00330 PANORAMIC FILM $61<br />
01110 PROPHYLAXIS - ADULT $53<br />
01120 PROPHYLAXIS - CHILD $43<br />
01203 TOP FLUORIDE - CHILD $27<br />
01204 TOP FLUORIDE - ADULT $27<br />
01206 TOP FLUORIDE VARNISH $41<br />
01351 SEALANT - PER TOOTH $25<br />
02140 AMALGAM-ONE SURFACE PRIMARY/PERM $66<br />
02150 AMALGAM-TWO SURFACES PRIMARY/PERM $81<br />
02160 AMALGAM-3 SURFACES PRIMARY/PERM $103<br />
02330 RESIN COMPOS - ONE SURFACE ANTERIOR $75<br />
02331 RESIN COMPOS - 2 SURFACES ANTERIOR $97<br />
02332 RESIN COMPOS - 3 SURFACES ANTERIOR $117<br />
02335 RSN COMPOS-4/> SURF/W/INCISAL ANG $141<br />
02391 RESIN COMPOS - 1 SURFACE POSTERIOR $81<br />
02392 RESIN COMPOS - 2 SURFACES POSTERIOR $110<br />
02393 RESIN COMPOS - 3 SURFACES POSTERIOR $136<br />
02740 CROWN - PORCELAIN/CERAMIC SUBSTRATE $688<br />
02750 CROWN - PORCELN FUSED HI NOBLE METL $683<br />
02751 CROWN PORCELAIN-BASE METAL $625<br />
02752 CROWN - PORCELAIN FUSED NOBLE METAL $653<br />
02790 CROWN - FULL CAST HIGH NOBLE METAL $642<br />
02792 CROWN - FULL CAST NOBLE METAL $586<br />
02920 RECEMENT CROWN $41<br />
02930 STAINLESS STEEL CROWN - CHILD $125<br />
02950 CORE BUILDUP INCLUDING ANY PINS $103<br />
02954 PREFABR POST&CORE ADDITION CROWN $158<br />
03120 PULP CAP - INDIRECT $36<br />
03310 ANTERIOR $397<br />
03320 BICUSPID $474<br />
03330 MOLAR $654<br />
04341 PRDNTL SCAL&ROOT PLAN 4/>TEETH-QUAD $116<br />
04342 PRDONTAL SCAL&ROOT PLAN 1-3 TEETH $73<br />
04355 FULL MOUTH DEBRID COMP EVAL&DX $57<br />
04381 LOC DEL ANTIMICROBIAL AGT TOOTH BR $60<br />
04910 PERIODONTAL MAINTENANCE $71
06010 ENDOSTEAL IMPLANT $1,339<br />
06240 PONTIC - PORCELAIN - HIGH NOBLE $659<br />
06750 CRWN PORCLN FUSD HI NOBL MTL-DENTUR $683<br />
07140 EXTRAC ERUPTED TOOTH/EXPOSED ROOT $68<br />
07210 SURG REMOVAL ERUPTED TOOTH $128<br />
07220 SURG REMOVAL IMPACTED TOOTH $166<br />
07230 REMOVAL IMPACT TOOTH - PARTLY BONY $204<br />
07240 REMOVAL IMPACTED TOOTH - CMPL BONY $269<br />
09110 PALLIATVE TX DENTAL PAIN-MINOR PROC $43<br />
09220 DP SEDATION/GEN ANES-1ST 30 MIN $226<br />
09221 DP SEDAT/GEN ANES-EA ADD 15 MIN $73<br />
09310 CONSULTATION $54<br />
09940 OCCLUSAL GUARD BY REPORT $352





![Course Catalog [PDF] - Midlothian ISD](https://img.yumpu.com/36431290/1/190x245/course-catalog-pdf-midlothian-isd.jpg?quality=85)