Claim Requirements and Dispute Guidelines - Tufts Health Plan
Claim Requirements and Dispute Guidelines - Tufts Health Plan
Claim Requirements and Dispute Guidelines - Tufts Health Plan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong><br />
Senior Care Options Provider Manual<br />
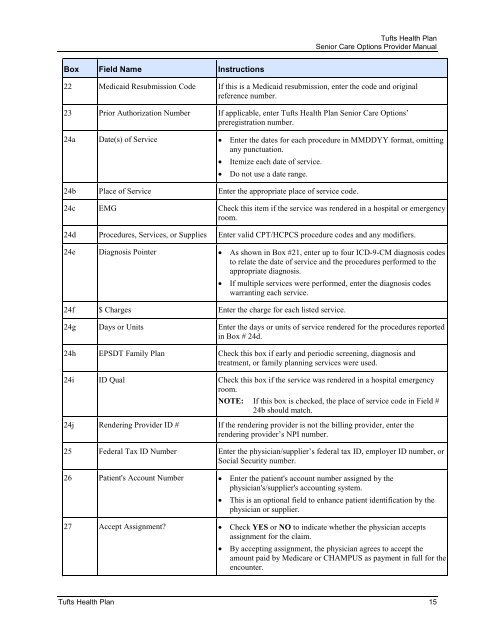
Box Field Name Instructions<br />
22 Medicaid Resubmission Code If this is a Medicaid resubmission, enter the code <strong>and</strong> original<br />
reference number.<br />
23 Prior Authorization Number If applicable, enter <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> Senior Care Options’<br />
preregistration number.<br />
24a Date(s) of Service • Enter the dates for each procedure in MMDDYY format, omitting<br />
any punctuation.<br />
• Itemize each date of service.<br />
• Do not use a date range.<br />
24b Place of Service Enter the appropriate place of service code.<br />
24c EMG Check this item if the service was rendered in a hospital or emergency<br />
room.<br />
24d Procedures, Services, or Supplies Enter valid CPT/HCPCS procedure codes <strong>and</strong> any modifiers.<br />
24e Diagnosis Pointer • As shown in Box #21, enter up to four ICD-9-CM diagnosis codes<br />
to relate the date of service <strong>and</strong> the procedures performed to the<br />
appropriate diagnosis.<br />
• If multiple services were performed, enter the diagnosis codes<br />
warranting each service.<br />
24f $ Charges Enter the charge for each listed service.<br />
24g Days or Units Enter the days or units of service rendered for the procedures reported<br />
in Box # 24d.<br />
24h EPSDT Family <strong>Plan</strong> Check this box if early <strong>and</strong> periodic screening, diagnosis <strong>and</strong><br />
treatment, or family planning services were used.<br />
24i ID Qual Check this box if the service was rendered in a hospital emergency<br />
room.<br />
NOTE: If this box is checked, the place of service code in Field #<br />
24b should match.<br />
24j Rendering Provider ID # If the rendering provider is not the billing provider, enter the<br />
rendering provider’s NPI number.<br />
25 Federal Tax ID Number Enter the physician/supplier’s federal tax ID, employer ID number, or<br />
Social Security number.<br />
26 Patient's Account Number • Enter the patient's account number assigned by the<br />
physician's/supplier's accounting system.<br />
• This is an optional field to enhance patient identification by the<br />
physician or supplier.<br />
27 Accept Assignment • Check YES or NO to indicate whether the physician accepts<br />
assignment for the claim.<br />
• By accepting assignment, the physician agrees to accept the<br />
amount paid by Medicare or CHAMPUS as payment in full for the<br />
encounter.<br />
<strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> 15