NCC Pediatrics Continuity Clinic Curriculum: Atopic Dermatitis ...
NCC Pediatrics Continuity Clinic Curriculum: Atopic Dermatitis ...
NCC Pediatrics Continuity Clinic Curriculum: Atopic Dermatitis ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Atopic</strong> <strong>Dermatitis</strong> Cases<br />
Case 1:<br />
Colton is a 15 month old male infant who presents for a routine well visit. He is the only child of<br />
well-educated parents who live in the suburbs. His height and weight have been stable at the 50 th<br />
percentile. He was breastfed for the first year of his life and continues to breastfeed at night. He<br />
was introduced to solid foods at 6 months of age and has fully transitioned to table foods. His<br />
mother boasts that he has “never had a runny nose in his life” and that she uses hand sanitizer<br />
“all the time, of course”. Her only concern is for a red, dry, itchy rash that keeps recurring on his<br />
cheeks, arms, and legs. She has not noticed any triggers.<br />
Based on history, what are protective and predisposing factors for Colton developing AD<br />
• Protective: exclusive breastfeeding for at least the first 4<br />
months of life; introduction of solid foods after 4 months of life.<br />
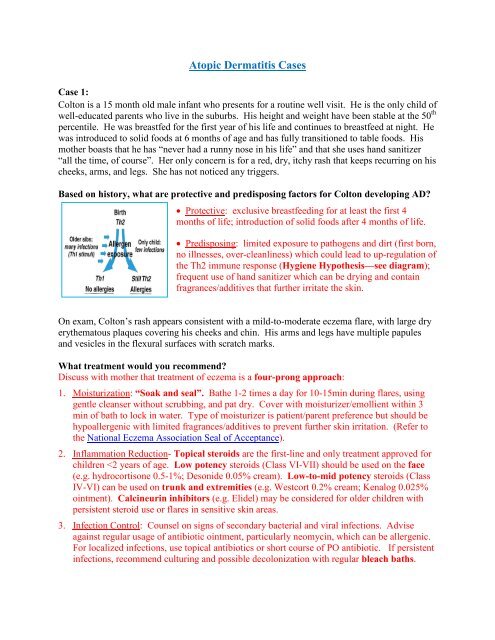
• Predisposing: limited exposure to pathogens and dirt (first born,<br />
no illnesses, over-cleanliness) which could lead to up-regulation of<br />
the Th2 immune response (Hygiene Hypothesis—see diagram);<br />
frequent use of hand sanitizer which can be drying and contain<br />
fragrances/additives that further irritate the skin.<br />
On exam, Colton’s rash appears consistent with a mild-to-moderate eczema flare, with large dry<br />
erythematous plaques covering his cheeks and chin. His arms and legs have multiple papules<br />
and vesicles in the flexural surfaces with scratch marks.<br />
What treatment would you recommend<br />
Discuss with mother that treatment of eczema is a four-prong approach:<br />
1. Moisturization: “Soak and seal”. Bathe 1-2 times a day for 10-15min during flares, using<br />
gentle cleanser without scrubbing, and pat dry. Cover with moisturizer/emollient within 3<br />
min of bath to lock in water. Type of moisturizer is patient/parent preference but should be<br />
hypoallergenic with limited fragrances/additives to prevent further skin irritation. (Refer to<br />
the National Eczema Association Seal of Acceptance).<br />
2. Inflammation Reduction- Topical steroids are the first-line and only treatment approved for<br />
children