Management of Dental Patients on Warfarin Therapy ... - Exodonti.info
Management of Dental Patients on Warfarin Therapy ... - Exodonti.info
Management of Dental Patients on Warfarin Therapy ... - Exodonti.info

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
▲<br />
M E D I C I N E I N MEDICINE D E N T I S T RIN Y DENTISTRY<br />
Abstract: The surgical management <str<strong>on</strong>g>of</str<strong>on</strong>g> patients <strong>on</strong> anticoagulant therapy is <str<strong>on</strong>g>of</str<strong>on</strong>g>ten<br />
poorly understood in all fields <str<strong>on</strong>g>of</str<strong>on</strong>g> medicine (not just dentistry).<br />
Until now there has been no uniform approach to managing these patients and<br />
much <str<strong>on</strong>g>of</str<strong>on</strong>g> the advice routinely given by medical practiti<strong>on</strong>ers and haematologists has<br />
fallen behind the recent evidence.<br />
Many medical c<strong>on</strong>diti<strong>on</strong>s from atrial fibrillati<strong>on</strong> to prosthetic heart valves<br />
predispose patients to venous thrombosis and pulm<strong>on</strong>ary embolism (Table 1). In order<br />
to prevent these complicati<strong>on</strong>s, these patients are normally placed <strong>on</strong> an<br />
anticoagulant. By far the most comm<strong>on</strong> <strong>on</strong>e in use is <strong>Warfarin</strong>, which is a derivative <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
4 hydroxycoumarin.<br />
Dent Update 2004; 31: 379–384<br />
Clinical Relevance: This article will attempt to review the current literature and<br />
focus <strong>on</strong> developing guidelines c<strong>on</strong>cerning the management <str<strong>on</strong>g>of</str<strong>on</strong>g> patients <strong>on</strong> <strong>Warfarin</strong><br />
while carrying out procedures found in the primary care setting.<br />
W<br />
<str<strong>on</strong>g>Management</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>Dental</str<strong>on</strong>g> <str<strong>on</strong>g>Patients</str<strong>on</strong>g><br />
<strong>on</strong> <strong>Warfarin</strong> <strong>Therapy</strong> in a Primary<br />
Care Setting<br />
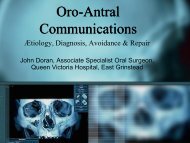
arfarin works by acting as an<br />
inhibitor <str<strong>on</strong>g>of</str<strong>on</strong>g> vitamin K. Vitamin K<br />
is required by blood coagulati<strong>on</strong> factors II,<br />
VII, IX, X and protein C (which are<br />
produced by the liver) for their activati<strong>on</strong><br />
from pr<str<strong>on</strong>g>of</str<strong>on</strong>g>actors to their active form as<br />
shown in the equati<strong>on</strong> (Figure 1).<br />
So it can be seen that factor VII is<br />
affected first and this increases a test<br />
called the prothrombin time (PT).<br />
The prothrombin time is carried out by<br />
adding calcium and thromboplastin to a<br />
citrated sample <str<strong>on</strong>g>of</str<strong>on</strong>g> the patient’s blood.<br />
Thromboplastin is a phospholipid extract<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> tissue (brain, lung, placenta). This can<br />
be <str<strong>on</strong>g>of</str<strong>on</strong>g> human origin (as used in the UK) or<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> animal extracti<strong>on</strong>, e.g. rabbit (as used<br />
more comm<strong>on</strong>ly in the USA). Different<br />
Vikram Chugani, BDS, MFDS RCS(Edin.),<br />
GDP (Berks.), formerly SHO in Restorative<br />
Dentistry, Leeds <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Institute.<br />
VIKRAM CHUGANI<br />
sources have different sensitivities<br />
leading to different laboratories providing<br />
different PT values (measured in sec<strong>on</strong>ds)<br />
for the same patient’s sample, depending<br />
<strong>on</strong> what type <str<strong>on</strong>g>of</str<strong>on</strong>g> thromboplastin is used. In<br />
order to combat this, the World Health<br />
Organizati<strong>on</strong> (WHO) recommended that a<br />
standardized PT test be c<strong>on</strong>ducted using<br />
the Internati<strong>on</strong>al Normalized Ratio (INR).<br />
Pr<str<strong>on</strong>g>of</str<strong>on</strong>g>actors <str<strong>on</strong>g>of</str<strong>on</strong>g> II,VII,IX,X<br />
Vitamin K<br />
▲<br />
This was d<strong>on</strong>e by comparing the patient’s<br />
PT with the mean normal PT <str<strong>on</strong>g>of</str<strong>on</strong>g> a group <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
healthy patients taken by using the<br />
thromboplastin used by that particular<br />
laboratory. This result was then given as a<br />
ratio. This then eliminates the varying<br />
sensitivities <str<strong>on</strong>g>of</str<strong>on</strong>g> thromboplastins used by<br />
different laboratories.<br />
INR =<br />
PT<br />
Mean normal PT<br />
The higher the INR value the greater the<br />
level <str<strong>on</strong>g>of</str<strong>on</strong>g> anticoagulati<strong>on</strong>.<br />
So it can be seen that c<strong>on</strong>tinuous<br />
anticoagulant therapy is a life-saving<br />
treatment, but may put patients at greater<br />
risk <str<strong>on</strong>g>of</str<strong>on</strong>g> experiencing haemorrhage after any<br />
procedure producing bleeding; in<br />
dentistry this ranges from simple scaling<br />
to cranio-facial surgery.<br />
Many studies have compared bleeding<br />
complicati<strong>on</strong>s in patients who have had<br />
their anticoagulati<strong>on</strong> altered to those<br />
whose regime was left unchanged. The<br />
majority found that, where the following<br />
good local measures were used, there is<br />
no significant difference in the amount <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
Activated factors II,VII,IX,X<br />
Vitamin K epoxide<br />
<strong>Warfarin</strong> works <strong>on</strong> the factors with the shortest half life first and those with the<br />
l<strong>on</strong>gest half life last. The half lives <str<strong>on</strong>g>of</str<strong>on</strong>g> the above factors are as shown:<br />
VII – 6 hours<br />
IX – 24 hours<br />
X – 40 hours<br />
II – 60 hours<br />
Figure 1. Blood coagulati<strong>on</strong> factors affected by <strong>Warfarin</strong>.<br />
▲<br />
<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Update – September 2004 379
MEDICINE IN DENTISTRY<br />
Indicati<strong>on</strong>s UK INR Target<br />
Pulm<strong>on</strong>ary embolus 2.5<br />
Deep vein thrombosis 2.5<br />
Atrial fibrillati<strong>on</strong> 2.5<br />
Recurrence <str<strong>on</strong>g>of</str<strong>on</strong>g> embolism after stopping <strong>Warfarin</strong> 2.5<br />
Recurrence <str<strong>on</strong>g>of</str<strong>on</strong>g> embolism during <strong>Warfarin</strong> therapy 3.5<br />
Mechanical heart valves 3.5<br />
Antiphospholipid syndrome 3.5<br />
Table 1. Types <str<strong>on</strong>g>of</str<strong>on</strong>g> medical c<strong>on</strong>diti<strong>on</strong>s that require <strong>Warfarin</strong> therapy. 1<br />
unc<strong>on</strong>trolled haemorrhage: 2,3,4,5<br />
l Pressure with gauze;<br />
l Period<strong>on</strong>tal packing;<br />
l Suckdown splint/immediate denture<br />
placement;<br />
l Suturing;<br />
l Haemostatic scaffolding, e.g. oxidized<br />
cellulose;<br />
l Tranexamic mouthwash – not in<br />
primary care; 6<br />
l Local anaesthetic with<br />
vasoc<strong>on</strong>strictor;<br />
Even those studies 7,8,9 that did measure a<br />
small but significant increase in<br />
postoperative bleeding complicati<strong>on</strong>s<br />
found that these were easily c<strong>on</strong>trolled by<br />
repeat applicati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> local measures.<br />
All these studies c<strong>on</strong>cluded if the INR<br />
was within the therapeutic range, i.e.
MEDICINE IN DENTISTRY<br />
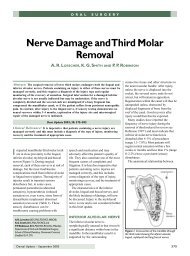
Assessment<br />
Chance <str<strong>on</strong>g>of</str<strong>on</strong>g> excess haemorrhage due to procedure<br />
Complicated medical history<br />
Complicating medicati<strong>on</strong><br />
reacti<strong>on</strong> with c<strong>on</strong>current use <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>Warfarin</strong><br />
affecting <strong>on</strong>ly certain individuals. <str<strong>on</strong>g>Patients</str<strong>on</strong>g><br />
should be advised to be aware <str<strong>on</strong>g>of</str<strong>on</strong>g> any<br />
signs <str<strong>on</strong>g>of</str<strong>on</strong>g> excessive haemorrhage.<br />
in handling any excessive haemorrhage.<br />
This is advised owing to unpredictability<br />
in extent <str<strong>on</strong>g>of</str<strong>on</strong>g> bleeding these patients may<br />
experience.<br />
These patients can be grouped into:<br />
l Those whose medical history<br />
increases the likelihood <str<strong>on</strong>g>of</str<strong>on</strong>g> bleeding:<br />
– liver disease;<br />
– obstructive jaundice.<br />
Both <str<strong>on</strong>g>of</str<strong>on</strong>g> these impair vitamin K<br />
metabolism and so potentiate the<br />
anticoagulati<strong>on</strong> effects <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>Warfarin</strong>.<br />
l Those whose c<strong>on</strong>comitant medicati<strong>on</strong><br />
makes the effects <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>Warfarin</strong><br />
unpredictable (Table 2).<br />
COMMON MEDICATION<br />
PRESCRIBED IN DENTISTRY<br />
AND ITS INTERACTION<br />
WITH WARFARIN 17,18<br />
Penicillins<br />
Yes<br />
Liaise with patient’s<br />
haematologist<br />
Too complicated<br />
for primary care<br />
setting. Refer to<br />
appropriate<br />
specialty<br />
Both dentist and<br />
haematologist happy for<br />
treatment within primary<br />
care setting<br />
Interacti<strong>on</strong> between penicillin and<br />
Yes<br />
Liaise with coagulati<strong>on</strong> clinic to<br />
schedule routine INR check for<br />
within 24 hours <str<strong>on</strong>g>of</str<strong>on</strong>g> dental<br />
treatment<br />
INR within acceptable range<br />
for procedure<br />
Commence with<br />
treatment<br />
Figure 2. <str<strong>on</strong>g>Management</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> patients taking <strong>Warfarin</strong> in a primary care setting.<br />
No<br />
No<br />
Seek advice <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
haematologist<br />
<strong>Warfarin</strong> are anecdotal 17 and rare.<br />
C<strong>on</strong>sidering the high frequency <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
prescribing <str<strong>on</strong>g>of</str<strong>on</strong>g> these two drugs, their<br />
presence in situati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> polypharmacy<br />
must be large, and yet the reports <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
reacti<strong>on</strong>s are rare. However, practiti<strong>on</strong>ers<br />
should ask their patients to be vigilant in<br />
case <str<strong>on</strong>g>of</str<strong>on</strong>g> any signs <str<strong>on</strong>g>of</str<strong>on</strong>g> unusual haemorrhage.<br />
Azoles, e.g. Metr<strong>on</strong>idazole,<br />
Fluc<strong>on</strong>azole, Ketac<strong>on</strong>azole<br />
This group <str<strong>on</strong>g>of</str<strong>on</strong>g> antifungals/antibacterials<br />
can cause a marked increase in the INR <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
a patient taking <strong>Warfarin</strong>. This can occur<br />
because azoles have been found to<br />
interfere with various steps in the<br />
metabolism <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>Warfarin</strong>. They should be<br />
avoided if at all possible. If they must be<br />
prescribed, the c<strong>on</strong>sultant haematologist<br />
should be <strong>info</strong>rmed so that a closer level<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> m<strong>on</strong>itoring can be instituted.<br />
Erythromycin<br />
Erythromycin causes an unpredictable<br />
Clindamycin<br />
With Clindamycin there is no evidence <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
any interacti<strong>on</strong>.<br />
Note: Prol<strong>on</strong>ged microbial therapy can<br />
alter the gut flora, especially those<br />
microbes resp<strong>on</strong>sible for vitamin K<br />
absorpti<strong>on</strong> and hence an increased chance<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> haemorrhage. There is, however, no<br />
evidence that single dose antibiotic cover<br />
regimes, as stated in the BNF, cause<br />
significant change in patients’ INR. 17<br />
NSAIDs, e.g. Dicl<str<strong>on</strong>g>of</str<strong>on</strong>g>enac,<br />
Ibupr<str<strong>on</strong>g>of</str<strong>on</strong>g>en, Naproxen,<br />
Ketapr<str<strong>on</strong>g>of</str<strong>on</strong>g>en<br />
NSAIDs may cause gastric irritati<strong>on</strong>,<br />
reversibly interfere with platelet adhesi<strong>on</strong><br />
and are thought to potentiate the<br />
anticoagulant effect <str<strong>on</strong>g>of</str<strong>on</strong>g> <strong>Warfarin</strong>.<br />
Paracetamol<br />
There is no evidence <str<strong>on</strong>g>of</str<strong>on</strong>g> interacti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
paracetamol with <strong>Warfarin</strong>.<br />
PRACTICAL MANAGEMENT<br />
Most patients carry a yellow record<br />
book <str<strong>on</strong>g>of</str<strong>on</strong>g> their INR readings. These are<br />
usually taken at between every two<br />
Potentiating<br />
l Fluc<strong>on</strong>azole<br />
l Ketac<strong>on</strong>azole<br />
l Metr<strong>on</strong>idazole<br />
l NSAIDs<br />
l Corticosteroids<br />
l Cephalosporins<br />
l Chloral hydrate<br />
l Penicillins<br />
l Erythromycins<br />
l Diflunisal<br />
l Salicylates<br />
l Proppoxyphene<br />
l Tetracyclines<br />
Opposing<br />
l Ascorbic acid<br />
l Barbiturates<br />
l Dicloxacillin sodium<br />
l Naficillin<br />
Table 2. Medicati<strong>on</strong> which may affect a<br />
patient’s INR. 14,18<br />
<str<strong>on</strong>g>Dental</str<strong>on</strong>g> Update – September 2004 381
MEDICINE IN DENTISTRY<br />
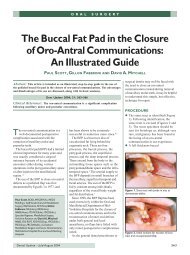
Table 3. Safety evaluati<strong>on</strong> chart for carrying out procedures <strong>on</strong> anticoagulated patients. Note: IR = Insufficient good quality research.<br />
weeks and every six weeks. Examining<br />
this record will give you the following<br />
<strong>info</strong>rmati<strong>on</strong>:<br />
l How <str<strong>on</strong>g>of</str<strong>on</strong>g>ten they have their INR<br />
checked;<br />
l How stable their INR is;<br />
l An idea <str<strong>on</strong>g>of</str<strong>on</strong>g> the patient’s normal<br />
value.<br />
If a procedure that may lead to<br />
haemorrhage is to be performed, then it<br />
is important that an INR value is<br />
obtained not more than 24 hours from<br />
commencement <str<strong>on</strong>g>of</str<strong>on</strong>g> the procedure 3,5,19<br />
This can be d<strong>on</strong>e by liaising with the<br />
anticoagulati<strong>on</strong> clinic and scheduling<br />
the appointment to fall less than 24<br />
hours after the scheduled INR check or<br />
vice versa.<br />
The 24-hour rule gives a sufficient<br />
window to obtain the results but not so<br />
l<strong>on</strong>g that any significant changes in the<br />
value are likely to have taken place<br />
(assuming that n<strong>on</strong>e <str<strong>on</strong>g>of</str<strong>on</strong>g> the earlier risk<br />
factors has been instigated).<br />
Extracti<strong>on</strong>s<br />
Minor oral surgical procedures can be<br />
carried out without alterati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the<br />
<strong>Warfarin</strong> dose, as l<strong>on</strong>g as the INR is less<br />
than four. These include simple<br />
extracti<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> 1–3 teeth and surgical<br />
removal <str<strong>on</strong>g>of</str<strong>on</strong>g> teeth. Good local measures<br />
should be used throughout. 2,3,4,5,7,9<br />
Gingival surgery<br />
Localized gingivoplasties with good<br />
local measures are probably acceptable<br />
within the therapeutic range up to an INR<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> 4. 19,20<br />
Quadrant gingivectomies should be<br />
d<strong>on</strong>e in stages, a small secti<strong>on</strong> being<br />
attempted first to assess the haemorrhage<br />
risk. 20<br />
Sub-gingival scaling<br />
Care should be exercised to avoid<br />
382 <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Update – September 2004
MEDICINE IN DENTISTRY<br />
excessive s<str<strong>on</strong>g>of</str<strong>on</strong>g>t tissue trauma when<br />
carrying out sub-gingival scaling. 20<br />
Regi<strong>on</strong>al nerve blocks<br />
Regi<strong>on</strong>al nerve blocks should be<br />
avoided wherever possible and<br />
replaced with suitable alternatives.<br />
For example, intraligamentary<br />
injecti<strong>on</strong>s to replace ID blocks.<br />
Pulp Extirpati<strong>on</strong><br />
Pulp extirpati<strong>on</strong> is unlikely to cause<br />
significant haemorrhage compared to<br />
n<strong>on</strong>-anticoagulated patients. 19,20<br />
In order to provide a framework for<br />
the management <str<strong>on</strong>g>of</str<strong>on</strong>g> these patients, a<br />
protocol has been devised in the form<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> a step-by-step flow diagram and a<br />
table by Herman et al., 19 which crossreferences<br />
INR values with comm<strong>on</strong><br />
dental treatments encountered in the<br />
primary dental care setting, has been<br />
adapted (Figure 2 and Table 3).<br />
CONCLUSION<br />
Most <str<strong>on</strong>g>of</str<strong>on</strong>g> the recent literature regarding<br />
<strong>Warfarin</strong> and dental surgery is in<br />
agreement that, with good local<br />
measures, routine oral surgical<br />
procedures can be undertaken without<br />
the need for alterati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the INR,<br />
when it is within the therapeutic range.<br />
There is still much scope for further<br />
studies into procedures found within<br />
the restorative sphere, although <strong>on</strong><br />
the whole these are less invasive and<br />
carry a lower risk <str<strong>on</strong>g>of</str<strong>on</strong>g> haemorrhage than<br />
those experienced by our oral surgery<br />
colleagues.<br />
Many patients, who could be<br />
treated safely and far more<br />
c<strong>on</strong>veniently in the primary care<br />
setting, are referred into the hospital<br />
system for treatment by a range <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
dental specialists. Indeed, many<br />
patients say this is where they would<br />
prefer to be treated. It is the hope <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
the author that this article has<br />
provided the necessary background<br />
<strong>info</strong>rmati<strong>on</strong> and an easy to follow set<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> guidelines to provide the care these<br />
patients require.<br />
ACKNOWLEDGEMENT<br />
I would like to thank Dr Brian Nattress for his guidance<br />
and support <strong>on</strong> this project and Gerald O’Sullivan,<br />
my first boss, whose standards and infectious<br />
enthusiasm for dentistry still guide me.<br />
REFERENCES<br />
1. Guideline therapeutic target INRs for patients <strong>on</strong><br />
<strong>Warfarin</strong>. Br J Haematol 1998; 101: 374–387.<br />
2. Devani P, Lavery KM, Howell CJT. <str<strong>on</strong>g>Dental</str<strong>on</strong>g><br />
extracti<strong>on</strong>s in patients <strong>on</strong> warfarin: is alterati<strong>on</strong><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> anticoagulant regime necessary. Br J Maxill<str<strong>on</strong>g>of</str<strong>on</strong>g>ac<br />
Surg 1998; 36: 107–111.<br />
3. Ramstrom G, Sindet-Pedersen S, Hall G et al.<br />
Preventi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> post surgical bleeding in oral<br />
surgery using tranexamic acid, without<br />
modificati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> oral anticoagulant. J Oral<br />
Maxill<str<strong>on</strong>g>of</str<strong>on</strong>g>ac Surg 1993; 51: 1211–1216.<br />
4. Blinder D, Manor Y, Martinowitz U et al. <str<strong>on</strong>g>Dental</str<strong>on</strong>g><br />
extracti<strong>on</strong>s in patients maintained <strong>on</strong> c<strong>on</strong>tinued<br />
oral anticoagulant. Oral Surg Oral Med Oral Pathol<br />
Oral Radiol Endod<strong>on</strong>tol 1999; 88: 137–140.<br />
5. Borea G, Mantebugnoli L, Capuzzi P et al.<br />
Tranexamic acid as a mouthwash in anticoagulant<br />
treated patients undergoing oral surgery. An<br />
alternative method to disc<strong>on</strong>tinuing anticoagulant<br />
therapy. Oral Surg Oral Med Oral Pathol 1993; 75:<br />
29–31.<br />
6. Northwest Medicines Informati<strong>on</strong> Centre.<br />
Surgical <str<strong>on</strong>g>Management</str<strong>on</strong>g><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> the Primary Care<br />
Patient <strong>on</strong> <strong>Warfarin</strong>,<br />
July 2001.<br />
7. Bailey BMW,<br />
Fordyce AM.<br />
Complicati<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
dental extracti<strong>on</strong>s in<br />
patients receiving<br />
warfarin<br />
anticoagulant<br />
therapy: a c<strong>on</strong>trolled<br />
clinical trial. Br Dent J<br />
1983; 155: 308–310.<br />
8. Weibert RT. Oral<br />
anticoagulant therapy<br />
in patients<br />
undergoing dental<br />
surgery. Clin<br />
Pharmacol 1992; 11:<br />
857–864.<br />
9. Wahl MJ. Myths <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
dental surgery inpatients<br />
receiving<br />
anticoagulant therapy.<br />
J Am Dent Assoc<br />
2000; 131: 77–81.<br />
10. Roser SM,<br />
Rosenbloom B.<br />
C<strong>on</strong>tinued<br />
anticoagulant in oral<br />
surgery procedures.<br />
Oral Surg Oral Med<br />
Oral Pathol 1975; 40:<br />
448–457.<br />
11. Madura JA,<br />
Rookstool M,<br />
Wease G. The<br />
management <str<strong>on</strong>g>of</str<strong>on</strong>g> patients <strong>on</strong> chr<strong>on</strong>ic coumadin<br />
therapy undergoing subsequent surgical<br />
procedures. Am Surg 1994; 60: 542–546.<br />
12. Johns<strong>on</strong> WT, Leary JM. <str<strong>on</strong>g>Management</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> dental<br />
patients with bleeding disorders: review and<br />
update. Oral Surg Oral Med Oral Pathol 1988; 66:<br />
297–303.<br />
13. D<strong>on</strong><str<strong>on</strong>g>of</str<strong>on</strong>g>f RB. Massachussetts General Hospital<br />
Manual <str<strong>on</strong>g>of</str<strong>on</strong>g> Oral and Maxill<str<strong>on</strong>g>of</str<strong>on</strong>g>acial Surgery. St Louis:<br />
CV Mosby, 1987; pp. 100–102, 152.<br />
14. Seward GR, Harris M, McGowan DA. Killey’s and<br />
Kay’s Outline <str<strong>on</strong>g>of</str<strong>on</strong>g> Oral Surgery, Part 1. Bristol:<br />
Wright, 1987:pp. 355–357.<br />
15. Mulligan R, Weitzel KG. Pretreatment<br />
management <str<strong>on</strong>g>of</str<strong>on</strong>g> the patient receiving<br />
anticoagulant drugs. J Am Dent Assoc 1988; 117:<br />
479–483.<br />
16. Wahl MJ, Howell J. Altering anticoagulati<strong>on</strong><br />
therapy: a survey <str<strong>on</strong>g>of</str<strong>on</strong>g> physicians. J Am Dent Assoc<br />
1996; 127: 625–638.<br />
17. Stockley IH. Drug interacti<strong>on</strong>s 5th editi<strong>on</strong>.<br />
L<strong>on</strong>d<strong>on</strong>: Pharmaceutical Press, 1999.<br />
18. <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Practiti<strong>on</strong>ers Formulary 2000–2002.<br />
L<strong>on</strong>d<strong>on</strong>: Pharmaceutical Press, 2000.<br />
19. Herman WW, Kanzelman JL, Sutley SH. Current<br />
perspectives <strong>on</strong> dental patients receiving<br />
coumarin anticoagulant therapy. J Am Dent Assoc<br />
1997; 128: 327–335.<br />
20. Chugani V, Nattress BR. Collati<strong>on</strong> and evaluati<strong>on</strong><br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> email questi<strong>on</strong>naires from x no. <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
c<strong>on</strong>sultants involved in special care dentistry and<br />
period<strong>on</strong>tology 2002.<br />
FACULTY OF DENTAL SURGERY<br />
THE ROYAL COLLEGE OF<br />
SURGEONS OF ENGLAND<br />
C<strong>on</strong>tracting with PCTs what’s in it for me<br />
On<br />
Friday 26 November 2004 in L<strong>on</strong>d<strong>on</strong><br />
& will be repeated <strong>on</strong><br />
Friday 3 December 2004 in Leeds<br />
On 1 st <str<strong>on</strong>g>of</str<strong>on</strong>g> April 2005, the Primary Care Trusts (PCTs) will take over the commissi<strong>on</strong>ing<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> all <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Services. This will include all General <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Practiti<strong>on</strong>ers and Specialist<br />
Practiti<strong>on</strong>ers. There will be a pr<str<strong>on</strong>g>of</str<strong>on</strong>g>ound effect up<strong>on</strong> how dental care is delivered, and<br />
paid for!<br />
The changes will also have significant implicati<strong>on</strong>s for Community <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Officers<br />
and the Sec<strong>on</strong>dary Care Services. It has been said that the changes are probably the<br />
most radical since the incepti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> the NHS in 1948.<br />
As the change-over date rapidly approaches, the aim <str<strong>on</strong>g>of</str<strong>on</strong>g> this Study Day is to update<br />
delegates <strong>on</strong> the latest developments from “those in the know”. This meeting will<br />
also provide the background <strong>info</strong>rmati<strong>on</strong> needed to negotiate the best possible local<br />
c<strong>on</strong>tract for you.<br />
The study day <strong>on</strong> Friday 3 December 2004<br />
will be held at the Weetwood Hall in Leeds<br />
This meeting will attract 5 credits for CPD and<br />
has also been approved for CPD Allowance.<br />
For an applicati<strong>on</strong> form and further details please c<strong>on</strong>tact:<br />
Mrs Mumtaz Rehman/ Miss Pearl Jansen<br />
Royal College <str<strong>on</strong>g>of</str<strong>on</strong>g> Surge<strong>on</strong>s <str<strong>on</strong>g>of</str<strong>on</strong>g> England<br />
35-43 Lincoln’s Inn Fields, L<strong>on</strong>d<strong>on</strong> WC2A 3PN<br />
Tel: 020 7869 6814/6819 Fax: 020 7869 6816<br />
E-mail mrehman@rcseng.ac.uk or pjansen@rcseng.ac.uk<br />
www.rcseng.ac.uk/dental//fds<br />
384 <str<strong>on</strong>g>Dental</str<strong>on</strong>g> Update – September 2004