


Neonatal Marfan Syndrome â A Case Report
Neonatal Marfan Syndrome â A Case Report
Neonatal Marfan Syndrome â A Case Report

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Case</strong> <strong>Report</strong><br />
Acta Cardiol Sin 2004;20:1715<br />
<strong>Neonatal</strong> <strong>Marfan</strong> <strong>Syndrome</strong> — A <strong>Case</strong> <strong>Report</strong><br />
Hsien-Yu Shih, Wan-Shiung Liu and Te-Jen Chen<br />
<strong>Neonatal</strong> <strong>Marfan</strong> syndrome is a rare congenital abnormality with atypical features of <strong>Marfan</strong> syndrome at an early<br />
stage. Although, neonatal <strong>Marfan</strong> syndrome is part of <strong>Marfan</strong> syndrome, its higher morbidity and mortality rate<br />
within young children period are different from those of classic <strong>Marfan</strong> syndrome noted in older patients. Several<br />
diversities of family history, cardiovascular system and cause of death are pointed out from recent studies.<br />
Key Words:<br />
<strong>Neonatal</strong> <strong>Marfan</strong> syndrome Congenital abnormality Classic <strong>Marfan</strong> syndrome<br />
INTRODUCTION<br />
CASE REPORT<br />
<strong>Marfan</strong> syndrome is rarely diagnosed early in neonatal<br />
or young age. <strong>Neonatal</strong> <strong>Marfan</strong> syndrome is a<br />
congenital abnormality with atypical features of <strong>Marfan</strong><br />
syndrome at an early stage, and it presents the appearances<br />
of tall stature, thin body build, long arms, legs,<br />
fingers and toes like <strong>Marfan</strong> syndrome. From genetic<br />
studies, <strong>Marfan</strong> syndrome is a heritable disorder with<br />
family history on chromosome 15, but spontaneous mutation<br />
tendency without family history was found in<br />
neonatal <strong>Marfan</strong> syndrome. More severe cardiovascular<br />
complications and poor prognosis were noted from neonatal<br />
<strong>Marfan</strong> syndrome. Higher morbidity and mortality<br />
rates during young age were also pointed out than classic<br />
<strong>Marfan</strong> syndrome.<br />
Early diagnosis and realization of differences between<br />
neonatal <strong>Marfan</strong> syndrome and classic <strong>Marfan</strong><br />
could help physicians to treat such kind of patients and<br />
explain to the family. We report a case of neonatal <strong>Marfan</strong><br />
syndrome and summarize this disease.<br />
Received: June 12, 2003 Accepted: February 18, 2004<br />
Department of Pediatrics, Chi-Mei Foundation Hospital, Tainan,<br />
Taiwan.<br />
Address correspondence and reprint requests to: Dr. Wan-Shiung Liu,<br />
Department of Pediatrics, Chi-Mei Foundation Hospital, No. 901,<br />
Chung-Hwa Road, Young-Kang City, Tainan 710, Taiwan.<br />
Tel: 886-6-281-2811 ext. 5592; Fax: 886-6-231-0604;<br />
E-mail: lleoteo@yahoo.com.tw<br />
The patient was a one-day-old male neonate who was<br />
born after 40 weeks gestation via normal delivery in our<br />
hospital. His birth body weight was 3272 grams and the<br />
Apgar scores were 7 and 9 at 1 and 5 minutes, respectively.<br />
No disease during the pregnant period of the<br />
mother was noted, nor was any inheritable family disease<br />
noted among the parents. The parents of the neonate were<br />
generally normal-figure appearance (father: age: 33 years<br />
old, body height: 176 cm; body weight: 68 kg; mother:<br />
age: 32 years old, body height: 156 cm; body weight: 53<br />
kg), and without any ocular or cardiovascular disease.<br />
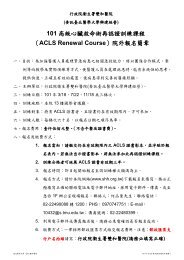
Several bizarre appearances of the neonate were<br />
noted, including: dolicocephaly, arachnodactyly (Figure<br />
1A), pigeon chest (Figure 1B), cyanosis, generalized<br />
pale appearance, rigidity and contracture of bilateral elbows,<br />
knees, and shoulder joints. Also, Gr. II/VI systolic<br />
murmur over left lower sternal border was found during<br />
acoustic examination.<br />
Cardiomegaly and pulmonary venous congestion<br />
were also detected from chest roentgenography. There<br />
were several abnormal findings from cardiac echo: 1. aortic<br />
root were dilatated in the ascending aorta; 2. patent<br />
ductus arteriosus with bi-directional shunt; 3. atrial septum<br />
defect with bi-directional shunt; 4. mitral valve regurgitation<br />
(MR)(++), tricuspid valve regurgitation (TR)(++),<br />
pulmonary valve regurgitation (PR)(++), aortic valve regurgitation<br />
(AR)(++), and congestive heart failure.<br />
After consulting geneticist, the neonatal <strong>Marfan</strong> syn-<br />
171 Acta Cardiol Sin 2004;20:1715
Hsien-Yu Shih et al.<br />
Figure 1. Clinical pictures of the patient on day 1 of birth: (A)<br />
Arachnodactyly: The fingers of right hand present longer and thinner.<br />
(B) Chest lateral view of patient. Pigeon chest (sternal convexity<br />
obvious) was noted.<br />
Figure 2. Parasternal long axis view of echocardiography: (A) Day<br />
1: Aortic root dilatation was noted. (the letters “AO” marked area) (B)<br />
Day 51: Aortic root dilatation appeared worse.<br />
drome was impressed. The karyotype of the neonate was<br />
46XY. There was no unusual finding pointed out in bilateral<br />
eyes of the patient after consultation of ophthalmologist.<br />
We treated the patient with diuretics and ACE inhibitor<br />
at the same time due to the detection of congestive<br />
heart failure. The conditions of congestive heart failure<br />
seem not ameliorated, and digoxin was prescribed to<br />
prevent the state becoming worse. However, dilatation<br />
of aorta, MR, TR, AR and congestive heart failure got<br />
worse progressively (Figures 2 A, B) and unfortunately,<br />
the patient expired due to severe congestive heart failure<br />
on the 52nd day after admission.<br />
DISCUSSION<br />
<strong>Marfan</strong> syndrome (MFS), first described in a 5-yearold<br />
child by the French pediatrician Antoine <strong>Marfan</strong> in<br />
1896, 1 is a dominantly inherited connective tissue disease<br />
with a wide range of phenotype severity in the<br />
skeletal, ocular and cardiovascular systems. The prevalence<br />
of MFS has been estimated to be approximately 4<br />
to 6 per 100,000 population in the United States, 2 and<br />
equally common in males and females.<br />
MFS is a heritable disorder where abnormalities of<br />
fibrillin protein are encoded by the fibrillin-1 gene<br />
(FBN1), a large gene composed of 65 exons on chromosome<br />
15q15-q21.3. 3 The “neonatal <strong>Marfan</strong> syndrome” or<br />
“ infantile <strong>Marfan</strong> syndrome” is a part of MFS whose<br />
atypical features of cardiovascular system with long,<br />
thin spindly physique can be detected at an early stage, 4<br />
but the neonatal MFS presents diverseness from older<br />
<strong>Marfan</strong> syndrome (or “classic <strong>Marfan</strong> syndrome”). It is<br />
likely a new mutation, not the family-inherited type from<br />
Acta Cardiol Sin 2004;20:1715 172
<strong>Neonatal</strong> <strong>Marfan</strong> <strong>Syndrome</strong><br />
Table 1. Comparison between neonatal <strong>Marfan</strong> syndrome and classic <strong>Marfan</strong> syndrome<br />
<strong>Neonatal</strong> <strong>Marfan</strong> syndrome<br />
Classic <strong>Marfan</strong> syndrome<br />
Clinical characteristics<br />
Age at death 1,6,11 Less than 2 years 32 16 years<br />
Main cause of death 11 CHF associated with MR and TR Aortic dissection or rupture<br />
Family history of <strong>Marfan</strong> syndrome 1,4,11 Negative in 70-100% Negative in only about 20-30%<br />
Joint contractures 1,4,6 47-64% Uncommon<br />
Cardiovascular characteristics 1,11<br />
MVP 73-100% 60 to 90%<br />
MR (moderate to severe) 89% 13%<br />
Aortic dilation 80-100% 60-85%<br />
AR 11% 73%<br />
TR 67% Uncommon<br />
PR 22% Uncommon<br />
CHF = congestive heart failure; MVP = mitral valve prolapse; AR = aortic regurgitation; TR = tricuspid regurgitation;<br />
MR = mitral regurgitation; PR = pulmonary regurgitation.<br />
the literature. 1<br />
The skeletal manifestations of MFS include tall stature,<br />
thin body build, long arms and legs (dolichostenomelia),<br />
long fingers and toes (arachnodactyly), hyperextensibility,<br />
pectus deformity, scoliosis, joint contractures, and narrow,<br />
high-arched palate. <strong>Neonatal</strong> MFS presents more joint<br />
contracture (67%) than classic MFS. In follow-up, neonatal<br />
MFS also have considerable morbidity due to scoliosis<br />
(32%) and easily dislocatable joint (36%). 1<br />
The majority of cardiovascular abnormalities of patients<br />
with MFS are associated with the ascending aorta,<br />
aortic valve, and the mitral valve, of which the most<br />
common are aortic root dilatation, aortic regurgitation,<br />
and mitral valve prolapse. 5<br />
The cardiovascular abnormalities in neonatal MFS<br />
differ somewhat from those seen in older patients.<br />
Multivalvular abnormalities are the major frequent cardiac<br />
pathology in children compared to aortic complications in<br />
adults. In these neonates, there are significant mitral,<br />
tricuspid, and pulmonary regurgitations noted, whereas<br />
among adult patients aortic root dilatation, aortic regurgitation,<br />
and aortic dissection are predominate. 5,6 In addition,<br />
children with MFS have tendency of obvious heart failure.<br />
Cardiovascular problems are responsible for at least<br />
80% of deaths in MFS. 7 The main cause and mean age at<br />
death are different between neonatal and classic MFS.<br />
Congestive heart failure with mitral and tricuspid regurgitation<br />
is the main reason of death in neonatal MFS<br />
within the first year of life, but aortic dissection or rupture<br />
is the major cause of death of classic MFS during<br />
33.5 years of life 8,9 (Table 1). The neonatal MFS life<br />
span is less than 2 years, due to the reason of severity of<br />
cardiovascular problems.<br />
<strong>Neonatal</strong> MFS has higher morbidity and mortality<br />
rate within young age than classic MFS, therefore, the<br />
pediatric cardiologist should explain the complications<br />
to the families, and some degree of psychosocial support<br />
may be needed.<br />
REFERENCES<br />
1. Morse RP, Rockenmacher S, Pyeritz RE, et al. Diagnosis and<br />
management of infantile <strong>Marfan</strong> syndrome. Pediatrics. 1990;86:<br />
888-95.<br />
2. Pyertiz RE, McKusick VA. The <strong>Marfan</strong> syndrome: diagnosis and<br />
management. N Engl J Med 1979;300:727-77.<br />
3. Dietz HC, Pyeritz RE, Hall BD, et al. The <strong>Marfan</strong> syndrome<br />
locus: confirmation of assignment to chromosome 15 and<br />
identification of tightly linked markers at 15q15-q21.3. Genomics<br />
1991;9:355-61.<br />
4. Jonathon R Gray, Sarah J Davies. <strong>Marfan</strong> syndrome. J Med Genet<br />
1996;33:403-8.<br />
5. Roman MJ, Devereux RB, Kramer-Fox R, et al. Comparsion of<br />
cardiovascular and skeletal features of primary mitral valve<br />
prolapse and the <strong>Marfan</strong> syndrome. Am J Cardiol 1989;63: 317-21.<br />
6. Marsalese DL, Moodie DS, Vacante M, et al. <strong>Marfan</strong>’s syndrome:<br />
natural history and long-term follow-up of cardiovascular<br />
involvement. J Am Coll Cardiol 1989;14:422-8.<br />
7. Murdock JL, Walker BA, Halpern BL, et al. Life expectancy and<br />
causes of death in the <strong>Marfan</strong> syndrome. N Engl J Med 1972;286:<br />
804-8.<br />
8. Phornphutkul C, Rosenthal A, Nadas AS. Cardiac manifestations<br />
173 Acta Cardiol Sin 2004;20:1715
Hsien-Yu Shih et al.<br />
of <strong>Marfan</strong> syndrome in infancy and childhood. Circulation<br />
1973;47:587-95.<br />
9. Towbin JA. Genetic syndromes and clinic molecular genetics. In:<br />
Garson A Jr, Bricker JT, Fisher DJ, et al. The Science and Practice<br />
of Pediatric Cardiology. 2nd ed. Baltimore: Williams & Wilkins,<br />
1998:2627-99.<br />
Acta Cardiol Sin 2004;20:1715 174
<strong>Case</strong> <strong>Report</strong><br />
Acta Cardiol Sin 2004;20:171−5<br />
新 生 兒 <strong>Marfan</strong> 症 候 群 — 病 例 報 告<br />
施 憲 佑 劉 萬 雄 陳 德 人<br />
台 南 縣 財 團 法 人 奇 美 醫 院 小 兒 心 臟 科<br />
新 生 兒 <strong>Marfan</strong> 症 候 群 為 一 種 染 色 體 先 天 性 異 常 的 疾 病 。 在 新 生 兒 時 期 即 表 現 <strong>Marfan</strong> 症 候<br />
群 的 病 徵 是 相 當 罕 見 。 雖 然 新 生 兒 <strong>Marfan</strong> 症 候 群 是 屬 於 <strong>Marfan</strong> 症 候 群 的 一 部 份 , 但 是 其<br />
所 特 有 的 高 死 亡 率 和 高 罹 病 率 特 徵 卻 不 同 於 一 般 典 型 <strong>Marfan</strong> 症 候 群 。 從 近 期 文 獻 中 顯 示 ,<br />
新 生 兒 <strong>Marfan</strong> 症 候 群 在 心 臟 血 管 系 統 及 家 族 遺 傳 與 一 般 典 型 的 <strong>Marfan</strong> 症 候 群 有 著 許 多 顯<br />
著 的 不 同 點 。 因 此 , 藉 由 本 文 中 罕 見 的 病 例 以 及 文 獻 回 顧 來 比 較 兩 者 的 不 同 。<br />
關 鍵 詞 : 新 生 兒 <strong>Marfan</strong> 症 候 群 、 先 天 性 異 常 、 典 型 <strong>Marfan</strong> 症 候 群 。<br />
175










![Full Text [Download PDF]](https://img.yumpu.com/22999153/1/190x260/full-text-download-pdf.jpg?quality=85)