


Coronary Restenosis
Coronary Restenosis
Coronary Restenosis
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
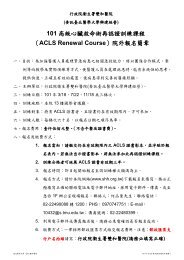
Chao-Chien Chang et al.form the neointimal tissue remain the main target ifrestenosis is to be challenged.Intracellular signaling of vascular smoothmuscle cells after vascular InjuryIn the past few years, many investigators have focusedtheir attention on the relative importance of singlereceptors in the complex mechanism of vascular smoothmuscle cell (VSMC) growth control after vascular injury.7 However, it is unlikely that the inhibition of only asingle receptor would be clinically relevant to the preventionof in-stent restenosis. Therefore, in the last fewyears, Indolfi et al. have studied mainly the commonpathways that multiple receptors employ to transmitmitogenic signals from the membrane to the nucleus inVSMCs after arterial injury, in particular, the role ofthe ras-raf-mitogen-activated protein kinase (MAPK)pathway and the cyclicadenosine monophosphate(cAMP)- dependent signaling in activated VSMCs(Figure 3). 7,17Ras-raf-MAPK signaling of smooth muscle cellsafter vascular injuryRas proteins are key transducers of mitogenic signalsfrom plasma membrane to the nucleus in many celltypes. Several mutants of ras (such as N17 H-ras andL61, S186 H-ras) act in a dominant negative manner toblock normal ras activation. N17 H-ras has reduced affinityfor guanosine triphosphate (GTP) and is defective(A) Growth factors(B) HormonesFigure 3. Schematic diagram of the main intracellular pathways regulating vascular smooth muscle cell proliferation. 18-20 Two main signalingpathways from the membrane to the nucleus are discussed. On the extracellular side of the plasma membrane are shown (A) growth factors bindingtyrosine kinase (TK) receptors and (B) hormones that bind seven-loop receptors that signal to the heterotrimeric G proteins. Grb-2: growth factorreceptor bound-2; SOS: Son of Sevenless; GTP: guanosine triphosphate; MEKK or MAPKKK: mitogen-activated protein kinase kinase kinase;MAPKK/MEK: mitogen activated protein kinase kinase; SEK: Stress activated protein kinase kinase; SAPK: Stress activated protein kinase; cAMP:cyclic adenosine monophosphate; AC: adenylate cyclase; PKA: protein kinase A; CREB: cAMP-responsive element binding protein.Acta Cardiol Sin 2005;21:17789 180
<strong>Coronary</strong> <strong>Restenosis</strong>, Pathophysiology and Molecular Mechanism of <strong>Restenosis</strong>in the final step of the exchange process, displacement ofguanine-exchange factor (GEF) by GTP, and sequesteringof GEFs into dead-end complexes. 7 This mutant hasbeen used to remove GEF activity from cells so that activationof endogenous ras proteins cannot occur. Indolfiet al. investigated the role of ras proteins in the vascularresponse to arterial injury in vivo by inactivating cellularras function in rats in which the common carotid arterywas subjected to balloon injury. 18 In animals treated withNl7 H-ras, a significant reduction of neointimal formation(-55%) was observed 14 days after balloon injurycompared with animals treated with RSV-LacZ. 18 A similareffect on neointimal formation after vascular injurywas observed with the inhibition of MAPKKinase by adominant inhibitor mutant gene. 19Activation of cAMP–protein kinase A signaling inhibitsneointimal formation after balloon injurycAMP is involved in the regulation of a variety ofcellular functions, such as cell proliferation and differentiation.Hormone-activated receptors increase the intracellularcAMP by inactivating the subunit of the trimericG-protein complex (Gs), which stimulates adenylatecyclase (Figure 3). To evaluate the effects of cAMP onVSMC proliferation, Indolfi et al. treated cultures of thesecells in vitro with different concentrations of 8-Br-cAMPand analyzed cell growth at different treatment periods. 20They found cAMP markedly inhibited VSMC proliferation.At the time of balloon injury, they locally delivered8-Br-cAMP. In the 8-Br-cAMP group, a significant reductionof neointima (-54%) was observed 14 days aftervascular injury compared with the control group. 20 An inhibitionof neointimal formation after vascular injury alsowas observed in other experiments, 21 in which systemicadministration of 8-Cl-cAMP reduced protein kinase A(PKA) RI-subunit expression and upregulated PKARII-subunit expression.Cyclin-dependent kinase complexesThe cell cycle is a key regulator of the describedintracellular signals and has direct effects on multiplecell processes, including VSMC proliferation and cellmigration. 22 VSMCs within the media of adult arteriesnormally are quiescent, proliferate at low rates, and existin the G0 phase of the cell cycle. Upon stimulation bygrowth factors or after arterial injury, VSMCs exit thequiescent stage G0 and progress through the G1 andG1/S transitions of the cell cycle. G1 progression is regulatedby the assembly and phosphorylation of G1 cyclincyclin-dependentkinase (CDK) complexes, predominantlycyclin D-CDK and cyclin E-CDK-2 in VSMCs. 23Endogenous inhibitors of the cyclin-CDK complexes aretermed the CDK inhibitors (CKIs). Two groups of CKIsare dominant in cardiovascular biology: the CDK inhibitorprotein (CIP/KIP) family, which includes p21 Cip1 andp27 Kip1 , and the INK4 family, which includes p16 Ink4a . 23Cells in the late S or G2/M phase do not migrate. Thereis a window of opportunity in the G1-to-G1/S transitionduring which VSMCs are able to migrate in response tomitogenic stimuli. Therefore, proteins such as the CKIsthat regulate G1 cell cycle progression are likely candidatesto regulate the initiation of migration as well. Theprotein p27 Kip1 is one important candidate, given that itis tightly regulated by mitogens. p27 Kip1 is an importantregulator of the mammalian cell cycle. 23 An increase inp27 Kip1 causes proliferating cells to exit from the cell cycle,whereas a decrease in p27 Kip1 is required for quiescentcells to resume cell division. 24 Low levels of p27 Kip1 areassociated with excessive cell proliferation in pathologicconditions such as inflammation and restenosis. 25 Highlevels of p27 Kip1 are observed in conditions of diminishedcell proliferation, such as in the late stages ofarterial wound repair in atherosclerosis and restenosis. 26Notably, Indolfi et al. demonstrated that A-kinase anchorprotein (AKAP), downstream molecules of the cAMP-PKA cascade, inhibits VSMC proliferation in vivo by increasingp27 Kip1 protein levels. 27RISK FACTORSIndependent risk factors for restenosis are a recenthistory of angina pectoris and a previous myocardial infarction.Other predictors of restenosis include stenosisof longer length, 28 chronic total occlusions, 29 and angiographicallyidentifiable thrombus. 30 Disease in saphenousvein grafts 31 and in small native vessels (less than 3.0mm) 32 is associated with higher rates of restenosis. Oneof the leading predictors of angiographic stenosis afterangioplasty is postprocedural diameter. 1 Structural riskfactors, such as a large degree of luminal narrowing beforeangioplasty, a small diameter of the referencesegment, a symmetric lesion, an extensive area of plaque,and residual stenosis, have been identified. 33-35 After181 Acta Cardiol Sin 2005;21:17789
Chao-Chien Chang et al.adjustment for other risk factors, such as diabetes mellitusand proximal lesions in the left anterior descending coronaryartery, there is only a slight difference in the rateof restenosis between first and successive coronaryangioplasties. 28,34 Genetic factors may also be involved,including polymorphisms for the D/D genotype of theangiotensin-converting enzyme (ACE) receptor, 36 glycoproteinreceptor IIIa PIA1/PIA2, 37 4G/5G promoter ofthe plasminogen activator inhibitor 1, 38 and haptoglobin2/2. 39 Additionally, a clinical presentation with unstableangina enhances the likelihood of restenosis afterangioplasty. 40 Plasminogen activator inhibitor 1, urokinaseplasminogen activator, and tissue factor havealso been demonstrated to be risk factors. 41,42TREATMENTShortly after the phenomenon of restenosis was recognized,investigators sought to develop devices thatcould more completely debulk the plaque burden at thetime of intervention. The rationale was to maximize thepostprocedural vessel diameter, thereby reducing therates of restenosis. One such device was the directionalcoronary atherectomy catheter, developed in the early1980s, which allows shaving and extraction of plaquefrom the diseased vessel wall. Comparisons of directionalcoronary atherectomy and standard angioplasty forthe treatment of de novo lesions have shown similarrates of restenosis between the two procedures. 1The coronary stent was designed to reduce restenosis.It has been demonstrated by IVUS that there are two majorcomponents which contribute to restenosis followingsuccessful PTCA. 43 One is the vascular remodeling whichoccurs by recoiling of the outer vessel wall, and the otherone is intimal hyperplasia. 44 <strong>Coronary</strong> stenting has beenshown to prevent vascular remodeling and to hinder vascularre-narrowing by allowing more room for intimalhyperplasia. Newer stents were designed taking these factorsinto consideration; they were designed for betterscaffolding and less intimal prolapse. In the BElgianNEtherlands Stent (BENESTENT) 45 and Stent <strong>Restenosis</strong>(STRESS) trials, 46 patients with de novo lesions were randomlyassigned to either angioplasty or stenting. Stentingwas associated with a lower rate of restenosis as comparedwith placebo in both the BENESTENT (22% vs.32%) and STRESS trials (31.6% vs. 42%). This beneficialeffect has been confirmed in other randomized trials,Acta Cardiol Sin 2005;21:17789 182
<strong>Coronary</strong> <strong>Restenosis</strong>, Pathophysiology and Molecular Mechanism of <strong>Restenosis</strong>Figure 4. Cell cyclein which restenosis rates were reduced by 25% to 50%as compared with angioplasty alone. 1 The benefits ofstenting are attributed to larger lumen gain, eliminationof vessel recoil, and prevention of negative remodeling.1 Unfortunately, neointimal hyperplasia remains aproblem after stenting. 47 The most recent advances inthe treatment of restenosis include intracoronary radiation(brachytherapy) and drug-coated stents (Table1)(Figure 4).BrachytherapyIn animals, intracoronary radiation reduces neointimalproliferation after angioplasty, presumably by decreasingsmooth muscle cell mitosis and by inducing apoptosis. 48Investigators have used both beta and gamma radiationfor this purpose.Beta particles are emitted electrons from a radioactiveisotope. The most extensively studied isotopeshave been phosphorus 32 ( 32 P) and strontium 90. In theProliferation Reduction with Vascular Energy Trial(PREVENT), patients with native or restenotic lesionswho had been treated with stenting or balloon angioplastywere randomly assigned to intervention with placebo or16-gray, 20-gray, or 24-gray radiotherapy (intracoronary32 P). 49 Radiotherapy reduced the restenosis at the targetsite as compared with placebo (8% vs. 39%, p=0.01).The angiographic and clinical benefits, however, werelimited by restenosis adjacent to the target site (14% inthe treated group vs. 11% in the placebo group) and bylate thrombotic events in the treated group. More recently,in the Stents and Radiation Trial (START), 50patients with in-stent restenosis were randomly assignedto brachytherapy or placebo after receiving mechanicaltreatment (primarily angioplasty) for in-stent restenosis.<strong>Restenosis</strong> within the entire segment treated with radiationwas reduced in 45% of controls and 29% of treatedpatients at 8 months (p =0.001). Because of this trial,the FDA has approved beta radiation for the treatment ofin-stent restenosis.In the Intimal Hyperplasia Inhibition With BetaInstent (INHIBIT) trial, 51 patients with in-stent restenosiswho had been treated with repeat percutaneous interventionwere randomly assigned to beta radiation or placebo.Angiographic restenosis was lower in the radiation group(26%) than in the placebo group (52%, p < 0.0001). In atrial of escalating doses of beta radiation after angioplasty183 Acta Cardiol Sin 2005;21:17789
Chao-Chien Chang et al.alone for de novo lesions, restenosis occurred in 4% ofpatients who had been treated with the highest radiationdose. 52 Conversely, the preliminary results from the randomizedBETA-CATH trial did not show beta radiationto be beneficial as a primary intervention strategy in denovo lesions. 53 The study randomly assigned 1455 patientswho had been treated with angioplasty, with orwithout stenting, to beta radiation or placebo. At 8months, restenosis rates in the analysis segment (treatedsegment plus 5 mm on both sides) did not differ significantlybetween radiation and placebo groups (31% vs.36%, p=0.3).Gamma radiation entails photon emission by radioisotopessuch as iridium 182, which has shown efficacyin reducing restenosis in the Scripps <strong>Coronary</strong> Radiationto Inhibit Proliferation Post Stenting (SCRIPPS) trial, 54the Washington Radiation for In-Stent <strong>Restenosis</strong> Trial(WRIST), 55 WRIST PLUS, 56 and Gamma-1 trial. 57 TheFDA approved gamma radiation for the treatment ofin-stent restenosis based on the Gamma-1 trial results. 57In this investigation, 252 patients with instent restenosiswere randomly assigned to either a placebo “hot wire” oran iridium 192 “hot wire” after undergoing angioplasty,atherectomy, or laser angioplasty. At 6 months, the incidenceof restenosis was 55% in the placebo group and32% in the treated group.These results indicate that brachytherapy is beneficial,albeit with several limitations. The procedure isexpensive, inconvenient, and requires the services of aradiation oncologist. Also, use of gamma radiation requiresthat personnel leave the room during the 20minutes of radiation exposure. The increased incidenceof late thrombosis and myocardial infarction is a majorconcern. In the Gamma-1 trial, for example, there was atrend toward late thrombosis (5% vs. 0.8%, p=0.07)and myocardial infarction (10% vs. 4.2%, p=0.09) inthe treated group when compared with the placebogroup. All of the late thrombosis events occurred in stentrecipients. Specifically, 6% of patients who receivednew stents at the time of intervention had late thrombosisas opposed to none of the nonstented patients.Similarly, late thrombosis occurred in 10% of treated patientsin PREVENT, 3% of treated patients in theINHIBIT trial, and 6% in the BETA-CATH trial. Prolongedantiplatelet therapy might ameliorate theseadverse effects. In the nonrandomized WRIST PLUS,late thrombosis was reported in only 3% of patients whohad undergone prolonged antiplatelet therapy (6 monthsof clopidogrel in addition to aspirin), 56 similar to the placebohistorical control group from WRIST. Longertherapy with clopidogrel (12 months) did not reduce theincidence of late thrombosis, but decreased the number ofmajor cardiac events and rate of repeat revascularization. 58Finally, follow-up duration of these patients has beenshort, and it is unclear whether untoward effects of radiation,including the potential for fibrosis and oncogenesis,might emerge.Drug-coated stentsThe most promising prospect for reducing restenosishas been the recent development of drug-coated stents.Several drugs are being tested for local delivery througheluting stents, including estradiol and paclitaxel. Themost extensively studied, to date, is sirolimus (rapamycin).Sirolimus is an immunosuppressive drug that is traditionallyused to prevent organ transplant rejection.Within the last 10 years, animal experiments have demonstratedits efficacy in reducing restenosis, and recentlyhuman clinical trials have been completed. In the RandomizedDouble-Blind Study with the Sirolimus-ElutingBX Velocity Balloon-Expandable Stent in the Treatmentof Patients with De Novo Native <strong>Coronary</strong> Lesions(RAVEL), patients were randomly given a sirolimuselutingstent or placebo. 59 The restenosis rate at 6 monthswas 0% in the sirolimus group compared with 26% inthe placebo group (p < 0.001). In the subgroup of diabeticpatients, none of the patients with drug-coatedstents had restenosis compared with 42% of those withbare metal stents (p < 0.002). Preliminary results wererecently presented for the Sirolimus-coated BX VelocityBalloon-expandable Stent in the Treatment of Patientswith De Novo <strong>Coronary</strong> Artery Lesions (SIRIUS) trial. 60In this trial, 1058 patients were randomly given asirolimus-coated stent or a bare stent. At angiographicfollow-up at 8 months, in-segment restenosis (stent plus5-mm proximal and distal borders) occurred in 9% ofsirolimus-coated stent patients compared with 36% ofcontrol group patients (p < 0.001). Adverse effects didnot differ between two groups, including stent thrombosis(0.6% in the sirolimus group vs. 1.1% in the placebogroup) and aneurysm formation (0.6% in the sirolimusgroup vs. 1.1% in the placebo group). Recently, paclitaxel-Acta Cardiol Sin 2005;21:17789 184
<strong>Coronary</strong> <strong>Restenosis</strong>, Pathophysiology and Molecular Mechanism of <strong>Restenosis</strong>coated stents have also shown benefit in reducingrestenosis. In a randomized study involving patients assignedto low-dose paclitaxel-coated stents, high-dosepaclitaxel-coated stents, or placebo, 61 restenosis occurredin 27% of patients in the control group, 12% in thelow-dose group, and 4% in the high-dose group at 4- to6-month follow-up. After nine months follow-up, therate of angiographic restenosis was reduced from 26.6%to 7.9% with the paclitaxel-eluting stent (relative risk,0.30; 95% confidence interval, 0.19 to 0.46; p < 0.001).The nine-month composite rates of death from cardiaccauses or myocardial infarction (4.7% and 4.3%, respectively)and stent thrombosis (0.6% and 0.8%, respectively)were similar in the group that received a paclitaxelelutingstent and the group that received a bare-metalstent. 62Healing-enhancing stentsVascular endothelial growth factor-eluting stentsDespite promising results with local delivery of thevascular endothelial growth factor (VEGF) to the site ofvascular injury, a recently conducted experimental studyof VEGF-eluting stents failed to demonstrate a beneficialeffect on endothelization or on intimal hyperplasia. TheseVEGF-eluting stents did not accelerate endothelization orinhibit restenosis, but they did reduce the stent thrombosisrate, which may make them less thrombogenic. 63 Acceleratedendothelialization by local delivery of endothelialspecificgrowth factors could constitute an attractive alternativeto direct antiproliferative strategies.Estradiol-eluting stentsEstradiol may improve vascular healing, reducesmooth muscle cell (SMC) migration and proliferation,and promote local angiogenesis. Several animal and humanstudies have demonstrated a protective effect ofestrogen on coronary circulation. 64 Estrogen appearsnot only to have a beneficial effect on lipids but alsostimulates NO production by endothelial cells (ECs), aswell as inhibits the expression of the proto-oncogenec-myc, which is implicated in the development ofintimal hyperplasia. 65 Estradiol may also contribute tovascular healing and prevent restenosis by improvingre-endothelization (estrogen receptor alpha-activation)and by decreasing SMC migration and proliferation (estrogenreceptor beta-activation). 66 This explains why17-beta-estradiol-eluting stents are associated with reducedneointimal formation without affecting endothelialregeneration with potential benefit in the preventionand treatment of in-stent restenosis. 64 Recent data haveshown that estradiol-eluting phosphorylcholine-coatedstents that were implanted in porcine coronary arteriesreduced neointimal hyperplasia by 40% compared withcontrol stents. The Estrogen And Stent To Eliminate<strong>Restenosis</strong> (EASTER) study was a single-center feasibilitystudy testing 17-beta-estradiol-eluting BiodivYsio(Abbott, Abbott Park, Illinois) stents in 30 patients withde novo coronary lesions. Stents were loaded on-site byimmersion in a solution of estradiol. Late loss was 0.32mm in lesion and 0.57 mm in stent. Neointimal hyperplasia,detected using IVUS, was 23.5%. At six months,there were no deaths or stent thromboses, and only onepatient underwent repeat revascularization. A secondphase of the EASTER study has recently concluded,and results are not available.Stents attracting endothelial cells (ECs)Stents may be used to attract circulating ECs. Rstents (Orbus Medical Technologies, Fort Lauderdale,Florida) coated with antibodies to CD34 receptors onprogenitor circulating ECs have been implanted in pigcoronary arteries. These non drug-eluting stents wouldultimately promote the elution of biologically active substancesthrough a functioning endothelium monolayer.The effects of these novel stents on restenosis remain tobe demonstrated. Kutryk et al. 67 proposed the seeding ofintravascular stents by the xenotransplantation of geneticallymodified ECs, which were capable of modifyingthe pathophysiologic response to vessel wall damage andprovide controllable levels of active compounds. Thefeasibility and potential of this method has been demonstratedin animal studies. There are also preliminarydata 68 suggesting that endoluminal seeding of syngeneicSMCs can be effective in reducing intimal hyperplasia ina restenosis animal model and in arterial allografts.CONCLUSIONGiven the prevalence of coronary artery disease andthe widespread dissemination of technology and expertise,the number of percutaneous coronary interventionswill continue to increase aggressively. Interventional cardiologistswill treat more patients, including those with185 Acta Cardiol Sin 2005;21:17789
Chao-Chien Chang et al.comorbid conditions that may complicate percutaneoustreatment, such as diabetes, multivessel disease, andchronic total occlusion. Therefore, expanding our understandingof restenosis and treatment options becomesmore pressing. Although many patients can benefit frompercutaneous intervention, many can also suffer from itslimitations, with restenosis causing recurrent angina,ischemic events, and repeat interventions.For these patients, there are other treatment options.Intracoronary radiation, despite its limitations, has beenshown to be effective in ameliorating restenosis. Thecurrent data regarding drug-coated stents are promising.Ultimately, these advances offer great hope for markedlylower rates of restenosis and a new era in interventionalcardiology.REFERENCES1. Bauters C, Isner JM. The biology of restenosis. In: Topol EJ, Ed.Textbook of Cardiovascular Medicine. Philadelphia, Pennsylvania:Lippincott-Raven; 1998:2465-90.2. Gruntzig AR. Transluminal dilation of coronary artery stenosis.Lancet 1978;1:263.3. Holmes DR, Vlietstra RE, Smith HC, et al. <strong>Restenosis</strong> afterpercutaneous transluminal coronary angioplasty (PTCA): a reportfrom the PTCA registry of the National Heart, Lung, and BloodInstitute. Am J Cardiol 1984;53(suppl C):77-81.4. Cohen EA, Sykora K, Kimball BP, et al. Clinical outcome ofpatients more than one year following randomization in theCanadian <strong>Coronary</strong> Atherectomy Trial. Can J Cardiol 1997;13:825-30.5. Cummins FE, Nonweiler JM, Ninneman RW. Percutaneousexcimer laser coronary angioplasty: results of one center in amulti-center investigation. J Clin Laser Med Surg 1992;10:171-5.6. Levin TN, Holloway S, Feldman T. Acute and late clinicaloutcome after rotational atherectomy for complex coronarydisease. Cathet Cardiovasc Diagn 1998;45:122-30.7. Indolfi C, Coppola C, Torella D, et al. Gene therapy for restenosisafter balloon angioplasty and stenting. Cardiol Rev 1999;7:324-31.8. Indolfi C, Torella D, Coppola C, et al. Rat carotid artery dilationby PTCA balloon catheter induces neointimal formation inpresence of IEL rupture. Am J Physiol 2002;283:H760-H767.9. Farb A, Sangiorgi G, Carter AJ, et al. Pathology of acute andchronic coronary stenting in humans. Circulation 1999;99:44-52.10. Glagov S, Weisenberg E, Zarins CK, et al. Compensatory enlargementof human atherosclerotic coronary arteries. N Engl JMed 1987;316:1371-5.11. Mintz GS, Popma JJ, Pichard AD, et al. Arterial remodeling aftercoronary angioplasty: a serial intravascular ultrasound study.Circulation 1996;94:35-43.12. Miano JM, Vlasic N, Tota RR, Stemerman MB. Localization ofFos and Jun proteins in rat aortic smooth muscle cells aftervascular injury. Am J Pathol 1993;142:715-24.13. Riessen R, Wight TN, Pastore C, et al. Distribution of hyaluronanduring extracellular matrix remodeling in human restenoticarteries and balloon-injured rat carotid arteries. Circulation1996;93:1141-7.14. Ward MR, Tsao PS, Agrotis A, et al. Low blood flow afterangioplasty augments mechanisms of restenosis: inward vesselremodeling, cell migration, and activity of genes regulatingmigration. Arterioscler Thromb Vasc Biol 2001;21:208-13.15. Wilcox JN, Waksman R, King SB, Scott NA. The role of theadventitia in the arterial response to angioplasty: the effect ofintravascular radiation. Int J Radiat Oncol Biol Phys 1996;36:789-96.16. Pickering JG, Ford CM, Chow LH. Evidence for rapid accumulationand persistently disordered architecture of fibrillarcollagen in human coronary restenosis lesions. Am J Cardiol1996;78:633-7.17. Indolfi C, Chiariello M, Avvedimento EV. Selective gene therapyof proliferative disorders: sense and antisense. Nat Med 1996;6:634-5.18. Indolfi C, Avvedimento EV, Rapacciuolo A, et al. Inhibition ofcellular RAS prevents smooth muscle cell proliferation aftervascular injury in vivo. Nat Med 1995;6:541-5.19. Indolfi C, Avvedimento EV, Rapacciuolo A, et al. In vivo genetransfer: prevention of neointimal formation by inhibition ofmitogen-activated protein kinase kinase. Basic Res Cardiol 1997;92:378-84.20. Indolfi C, Avvedimento EV, Di Lorenzo E, et al. Activation ofcAMP–PKA signaling in vivo inhibits smooth muscle cellproliferation induced by vascular injury. Nat Med 1997;3:775-7.21. Indolfi C, Di Lorenzo E, Rapacciuolo A, et al. 8-Chloro-cAMPinhibits smooth muscle cell proliferation in vitro and neointimalformation induced by balloon injury in vivo. J Am Coll Cardiol2000;36:288-93.22. Boehm M, Nabel EG. Cell cycle and cell migration: new pieces tothe puzzle. Circulation 2001;103:2879-81.23. Nabel EG. CDKs and CKIs: molecular targets for tissue remodelling.Nat Rev Drug Discov 2002;1:587-98.24. Boehm M, Yoshimoto T, Crook MF, et al. A growth factordependentnuclear kinase phosphorylates p27(Kip1) and regulatescell cycle progression. EMBO J 2002;21:3390-401.25. Ophascharoensuk A, Fero ML, Hughes J, et al. The cyclindependentkinase inhibitor p27Kip1 safeguards against inflammatoryinjury. Nat Med 1998;4:575-80.26. Tanner FC, Boehm M, Akyurek LM, et al. Differential effects ofthe cyclin-dependent kinase inhibitors p27(Kip1), p21(Cip1), andp16(Ink4) on vascular smooth muscle cell proliferation. Circulation2000;101:2022-5.27. Indolfi C, Stabile E, Coppola C, et al. Membrane-bound proteinActa Cardiol Sin 2005;21:17789 186
<strong>Coronary</strong> <strong>Restenosis</strong>, Pathophysiology and Molecular Mechanism of <strong>Restenosis</strong>kinase A inhibits smooth muscle cell proliferation in vitro and invivo by amplifying c-AMP-PKA signals. Circ Res 2001;88:319-24.28. Kuntz RE, Gibson CM, Nobuyoshi M, Baim DS. Generalizedmodel of restenosis after conventional balloon angioplasty,stenting and directional atherectomy. J Am Coll Cardiol 1993;21:15-25.29. Safian RD, McCabe CH, Sipperly ME, et al. Initial success andlong term follow-up of percutaneous transluminal coronaryangioplasty in chronic total occlusions versus conventionalstenoses. Am J Cardiol 1988;61:23G-28G.30. Violaris AG, Melkert R, Herrman JP, Serruys PW. Role ofangiographically identifiable thrombus on long-term luminalrenarrowing after coronary angioplasty: a quantitative angiographicanalysis. Circulation 1996;93:889-97.31. Platko WP, Hollman J, Whitlow PL, Franco I. Percutaneoustransluminal angioplasty of saphenous vein graft stenosis: longtermfollow-up. J Am Coll Cardiol 1989;14:1645-50.32. Akiyama T, Moussa I, Reimers B, et al. Angiographic and clinicaloutcome following coronary stenting of small vessels: a comparisonwith coronary stenting of large vessels. J Am Coll Cardiol 1998;32:1610-8.33. Hirshfeld JW Jr, Schwartz JS, Jugo R, et al. <strong>Restenosis</strong> aftercoronary angioplasty: a multivariate statistical model to relatelesion and procedure variables to restenosis. J Am Coll Cardiol1991;18:647-56.34. Schwartz RS, Holmes DR Jr, Topol EJ. The restenosis paradigmrevisited: an alternative proposal for cellular mechanisms. JAmColl Cardiol 1992;20:1284-93.35. Bourassa MG, Lesperance J, Eastwood C, et al. Clinical,physiologic, anatomic and procedural factors predictive ofrestenosis after percutaneous transluminal coronary angioplasty.J Am Coll Cardiol 1991;18:368-76.36. Ribichini F, Steffenino G, Dellavalle A, et al. Plasma activity andinsertion/deletion polymorphism of angiotensin I-convertingenzyme: a major risk factor and a marker of risk for coronary stentrestenosis. Circulation 1998;97:147-54.37. Di Castelnuovo A, de Gaetano G, Donati MB, Iacoviello L.Platelet glycoprotein receptor IIIa polymorphism PIA1/PIA2and coronary risk: a meta-analysis. Thromb Haemost 2001;85:626-33.38. Ortlepp JR, Hoffmann R, Killian A, et al. The 4G/5G promoterpolymorphism of the plasminogen activator inhibitor-1 gene andlate lumen loss after coronary stent placement in smoking andnonsmoking patients. Clin Cardiol 2001;24:585-91.39. Roguin A, Hochberg I, Nikolsky E, et al. Haptoglobin phenotypeas a predictor of restenosis after percutaneous transluminalcoronary angioplasty. Am J Cardiol 2001;87:330-2.40. Myler RK, Shaw RE, Stertzer SH, et al. Recurrence after coronaryangioplasty. Cathet Cardiovasc Diagn 1987;13:77-86.41. Strauss BH, Lau HK, Bowman KA, et al. Plasma urokinaseantigen and plasminogen activator inhibitor-1 antigen levelspredict angiographic coronary restenosis. Circulation 1999;100:1616-22.42. Mizuno O, Ikeda U, Hojo Y, et al. Tissue factor expression incoronary circulation as a prognostic factor for late restenosis aftercoronary angioplasty. Cardiology 2001;95:84-9.43. Gorge G, Ge J, Erbel R. Role of intravascular ultrasound in theevaluation of mechanisms of coronary interventions and restenosis.Am J Cardiol 1998;81:91-5.44. Arakawa K, Isoda K, Sugiyabu Y, et al. Intimal proliferation afterstenting reflected by increased stent-to-vessel cross-sectionalarea ratio: serial intravascular ultrasound study. J Cardiol 1998;32:379-89.45. Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison ofballoon-expandable-stent implantation with balloon angioplastyin patients with coronary artery disease. N Engl J Med 1994;331:489-95.46. Fischman DL, Leon MB, Baim DS, et al. A randomized comparisonof coronary stent placement and balloon angioplasty inthe treatment of coronary artery disease. N Engl J Med 1994;331:496-501.47. Gordon PC, Gibson CM, Cohen DJ, et al. Mechanisms ofrestenosis and redilation within coronary stents: quantitativeangiographic assessment. J Am Coll Cardiol 1993;21:1166-74.48. Scott NA, Crocker IR, Yin Q, et al. Inhibition of vascular cellgrowth by X-ray irradiation: comparison with gamma radiationand mechanism of action. Int J Radiat Oncol Biol Phys 2001;50:485-93.49. Raizner AE, Oesterle SN, Waksman R, et al. Inhibition ofrestenosis with beta-emitting radiotherapy: report of the ProliferationReduction with Vascular Energy Trial (PREVENT).Circulation 2000;102:951-8.50. Popma JJ, Suntharalingam M, Lansky AJ, et al. Randomized trialof 90Sr/90Y betaradiation versus placebo control for treatment ofin-stent restenosis. Circulation 2002;106:1090-6.51. Waksman R, Raizner AE, Yeung AC, et al. Use of localizedintracoronary beta radiation in treatment of in-stent restenosis: theINHIBIT randomized controlled trial. Lancet 2002;359:551-7.52. Verin V, Popowski Y, de Bruyne B, et al. Endoluminal betaradiationtherapy for the prevention of coronary restenosis afterballoon angioplasty. The Dose-Finding Study Group. N Engl JMed 2001;344:243-9.53. Teirstein PS, Kuntz RE. New frontiers in interventional cardiology:intravascular radiation to prevent restenosis. Circulation 2001;104:2620-6.54. Teirstein PS, Massullo V, Jani S, et al. Three-year clinical andangiographic follow-up after intracoronary radiation. Circulation2000;101:360-5.55. Waksman R, White RL, Chan RC, et al. Intracoronary gammaradiationtherapy after angioplasty inhibits recurrence in patientswith in-stent restenosis. Circulation 2001;101:2165-71.56. Waksman R, Ajani AE, White RL, et al. Prolonged antiplatelettherapy to prevent late thrombosis after intracoronary gammaradiationin patients with in-stent restenosis: WashingtonRadiation for In-Stent <strong>Restenosis</strong> Trial plus 6 months of187 Acta Cardiol Sin 2005;21:17789
Chao-Chien Chang et al.clopidogrel (WRIST PLUS). Circulation 2001;103:2332-5.57. Leon MB, Teirstein PS, Moses JW, et al. Localized intracoronarygamma-radiation therapy to inhibit the recurrence of restenosisafter stenting. N Engl J Med 2001;344:250-6.58. Waksman R, Ajani AE, Pinnow E, et al. Twelve versus sixmonths of clopidogrel to reduce major cardiac events in patientsundergoing gamma-radiation therapy for in-stent restenosis:Washington Radiation for In-Stent restenosis Trial (WRIST) 12versus WRIST PLUS. Circulation 2002;106:776-8.59. Morice M-C, Serruys PW, Sousa JE, et al. A randomizedcomparison of a sirolimus-eluting stent with a standard stent forcoronary revascularization. N Engl J Med 2002;347:561-6.60. Sousa JE, Serruys PW, Costa MA. New frontiers in cardiology:Drug-eluting stents: Part I. Circulation 2003;107:2274-9.61. Park S-J, Shim WH, Ho DS, et al. A paclitaxel-eluting stent forthe prevention of coronary restenosis. N Engl J Med 2003;348:1537-45.62. Gregg WS, Stephen GE, David AC, et al. A polymer-based,paclitaxel-eluting stent in patients with coronary artery disease. NEngl J Med 2004;350:221-31.63. Swanson N, Hogrefe K, Javed Q, et al. Vascular endothelial growthfactor (VEGF)-eluting stents: in vivo effects on thrombosis,endothelization and intimal hyperplasia. J Invasive Cardiol 2003;15:688-92.64. New G, Moses JW, Roubin GS, et al. Estrogen-eluting,phosphorylcholine-coated stent implantation is associated withreduced neointimal formation but no delay in vascular repair in aporcine coronary model. Cathet Cardiovasc Intervent 2002;57:266-71.65. Krishnankutty S, Chiu T, Mullen W, et al. Mechanisms ofestrogen induced vasodilation: in vivo studies in canine coronaryconductance and resistance arteries. J Am Coll Cardiol 1995;26:807-14.66. Geraldes P, Sirois MG, Tanguay JF. Specific contribution ofestrogen receptors on mitogen-activated protein kinase pathwaysand vascular cell activation. Circ Res 2003;93:399-405.67. Kutryk MJ, vanDortmont LM, deCrom RP, et al. Seeding ofintravascular stents by the xenotransplantation of geneticallymodified endothelial cells. Semin Interv Cardiol 1998;3:217-20.68. Gomes D, Louedec L, Plissonnier D, et al. Endoluminal smoothmuscle cell seeding limits intimal hyperplasia. J Vasc Surg2001;34:707-15.Acta Cardiol Sin 2005;21:17789 188
Review ArticleActa Cardiol Sin 2005;21:177−89冠 狀 動 脈 血 管 再 狹 窄張 釗 監 王 榮 添台 北 市 國 泰 綜 合 醫 院 心 臟 內 科冠 狀 動 脈 疾 病 的 介 入 性 療 法 中 , 血 管 支 架 置 放 術 比 傳 統 的 氣 球 擴 張 術 有 較 令 人 滿 意 的結 果 , 已 有 多 篇 的 文 獻 證 實 。 隨 著 使 用 率 的 增 加 , 血 管 支 架 置 放 後 所 遭 遇 的 難 題 , 如 血 管再 狹 窄 , 是 心 臟 科 醫 師 所 要 面 臨 的 一 大 問 題 。 血 管 再 狹 窄 的 問 題 , 尤 其 在 有 糖 尿 病 或 者multivessel 的 冠 狀 動 脈 疾 病 患 者 最 為 嚴 重 , 往 往 限 制 血 管 成 型 術 的 好 處 。 最 近 , 美 國 食 品和 藥 品 管 理 局 (FDA) 批 准 brachytherapy 和 drug-eluting stents 作 為 在 stent 的 再 狹 窄 問 題 上之 可 行 的 治 療 選 擇 。 本 篇 文 章 將 探 討 血 管 再 狹 窄 問 題 的 病 理 生 理 學 和 分 子 機 轉 , 並 回 顧 當今 與 將 來 的 治 療 選 擇 。關 鍵 詞 : 冠 狀 動 脈 血 管 再 狹 窄 、 血 管 再 狹 窄 問 題 的 病 理 生 理 學 和 分 子 機 轉 。189










![Full Text [Download PDF]](https://img.yumpu.com/22999153/1/190x260/full-text-download-pdf.jpg?quality=85)