CHAPTER 8 - BCSD Static Server - Bakersfield City School District
CHAPTER 8 - BCSD Static Server - Bakersfield City School District
CHAPTER 8 - BCSD Static Server - Bakersfield City School District

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
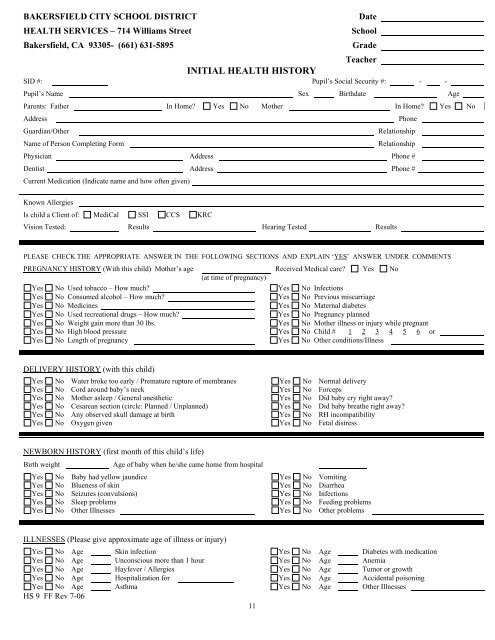
BAKERSFIELD CITY SCHOOL DISTRICT<br />
HEALTH SERVICES – 714 Williams Street<br />
<strong>Bakersfield</strong>, CA 93305- (661) 631-5895<br />
Date<br />
<strong>School</strong><br />
Grade<br />
Teacher<br />
INITIAL HEALTH HISTORY<br />
SID #: Pupil’s Social Security #: - -<br />
Pupil’s Name Sex Birthdate Age<br />
Parents: Father In Home Yes No Mother In Home Yes No<br />
Address<br />
Guardian/Other<br />
Name of Person Completing Form<br />
Phone<br />
Relationship<br />
Relationship<br />
Physician Address Phone #<br />
Dentist Address Phone #<br />
Current Medication (Indicate name and how often given)<br />
Known Allergies<br />
Is child a Client of: MediCal SSI CCS KRC<br />
Vision Tested: Results Hearing Tested Results<br />
PLEASE CHECK THE APPROPRIATE ANSWER IN THE FOLLOWING SECTIONS AND EXPLAIN ‘YES’ ANSWER UNDER COMMENTS<br />
PREGNANCY HISTORY (With this child) Mother’s age Received Medical care Yes No<br />
(at time of pregnancy)<br />
Yes No Used tobacco – How much Yes No Infections<br />
Yes No Consumed alcohol – How much Yes No Previous miscarriage<br />
Yes No Medicines Yes No Maternal diabetes<br />
Yes No Used recreational drugs – How much Yes No Pregnancy planned<br />
Yes No Weight gain more than 30 lbs. Yes No Mother illness or injury while pregnant<br />
Yes No High blood pressure Yes No Child # 1 2 3 4 5 6 or<br />
Yes No Length of pregnancy Yes No Other conditions/Illness<br />
DELIVERY HISTORY (with this child)<br />
Yes No Water broke too early / Premature rupture of membranes Yes No Normal delivery<br />
Yes No Cord around baby’s neck Yes No Forceps<br />
Yes No Mother asleep / General anesthetic Yes No Did baby cry right away<br />
Yes No Cesarean section (circle: Planned / Unplanned) Yes No Did baby breathe right away<br />
Yes No Any observed skull damage at birth Yes No RH incompatibility<br />
Yes No Oxygen given Yes No Fetal distress<br />
NEWBORN HISTORY (first month of this child’s life)<br />
Birth weight<br />
Age of baby when he/she came home from hospital<br />
Yes No Baby had yellow jaundice Yes No Vomiting<br />
Yes No Blueness of skin Yes No Diarrhea<br />
Yes No Seizures (convulsions) Yes No Infections<br />
Yes No Sleep problems Yes No Feeding problems<br />
Yes No Other Illnesses Yes No Other problems<br />
ILLNESSES (Please give approximate age of illness or injury)<br />
Yes No Age Skin infection Yes No Age Diabetes with medication<br />
Yes No Age Unconscious more than 1 hour Yes No Age Anemia<br />
Yes No Age Hayfever / Allergies Yes No Age Tumor or growth<br />
Yes No Age Hospitalization for Yes No Age Accidental poisoning<br />
Yes No Age Asthma Yes No Age Other Illnesses<br />
HS 9 FF Rev 7-06<br />
11