CHAPTER 8 - BCSD Static Server - Bakersfield City School District
CHAPTER 8 - BCSD Static Server - Bakersfield City School District
CHAPTER 8 - BCSD Static Server - Bakersfield City School District

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
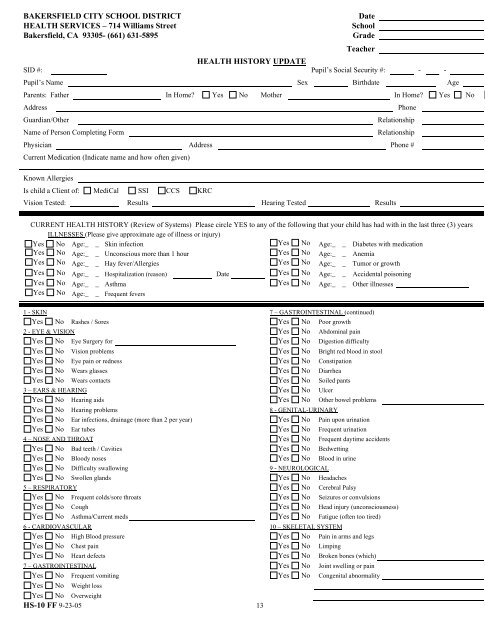
BAKERSFIELD CITY SCHOOL DISTRICT<br />
HEALTH SERVICES – 714 Williams Street<br />
<strong>Bakersfield</strong>, CA 93305- (661) 631-5895<br />
Date<br />
<strong>School</strong><br />
Grade<br />
Teacher<br />
HEALTH HISTORY UPDATE<br />
SID #: Pupil’s Social Security #: - -<br />
Pupil’s Name Sex Birthdate Age<br />
Parents: Father In Home Yes No Mother In Home Yes No<br />
Address<br />
Guardian/Other<br />
Name of Person Completing Form<br />
Phone<br />
Relationship<br />
Relationship<br />
Physician Address Phone #<br />
Current Medication (Indicate name and how often given)<br />
Known Allergies<br />
Is child a Client of: MediCal SSI CCS KRC<br />
Vision Tested: Results Hearing Tested Results<br />
CURRENT HEALTH HISTORY (Review of Systems) Please circle YES to any of the following that your child has had with in the last three (3) years<br />
ILLNESSES (Please give approximate age of illness or injury)<br />
Yes No Age:_ _ Skin infection Yes No Age:_ _ Diabetes with medication<br />
Yes No Age:_ _ Unconscious more than 1 hour Yes No Age:_ _ Anemia<br />
Yes No Age:_ _ Hay fever/Allergies Yes No Age:_ _ Tumor or growth<br />
Yes No Age:_ _ Hospitalization (reason) Date Yes No Age:_ _ Accidental poisoning<br />
Yes No Age:_ _ Asthma Yes No Age:_ _ Other illnesses<br />
Yes No Age:_ _ Frequent fevers<br />
1 - SKIN 7 – GASTROINTESTINAL (continued)<br />
Yes No Rashes / Sores Yes No Poor growth<br />
2 - EYE & VISION Yes No Abdominal pain<br />
Yes No Eye Surgery for Yes No Digestion difficulty<br />
Yes No Vision problems Yes No Bright red blood in stool<br />
Yes No Eye pain or redness Yes No Constipation<br />
Yes No Wears glasses Yes No Diarrhea<br />
Yes No Wears contacts Yes No Soiled pants<br />
3 – EARS & HEARING Yes No Ulcer<br />
Yes No Hearing aids Yes No Other bowel problems<br />
Yes No Hearing problems 8 - GENITAL-URINARY<br />
Yes No Ear infections, drainage (more than 2 per year) Yes No Pain upon urination<br />
Yes No Ear tubes Yes No Frequent urination<br />
4 – NOSE AND THROAT Yes No Frequent daytime accidents<br />
Yes No Bad teeth / Cavities Yes No Bedwetting<br />
Yes No Bloody noses Yes No Blood in urine<br />
Yes No Difficulty swallowing 9 - NEUROLOGICAL<br />
Yes No Swollen glands Yes No Headaches<br />
5 – RESPIRATORY Yes No Cerebral Palsy<br />
Yes No Frequent colds/sore throats Yes No Seizures or convulsions<br />
Yes No Cough Yes No Head injury (unconsciousness)<br />
Yes No Asthma/Current meds Yes No Fatigue (often too tired)<br />
6 - CARDIOVASCULAR 10 – SKELETAL SYSTEM<br />
Yes No High Blood pressure Yes No Pain in arms and legs<br />
Yes No Chest pain Yes No Limping<br />
Yes No Heart defects Yes No Broken bones (which)<br />
7 – GASTROINTESTINAL Yes No Joint swelling or pain<br />
Yes No Frequent vomiting Yes No Congenital abnormality<br />
Yes No Weight loss<br />
Yes No Overweight<br />
HS-10 FF 9-23-05 13