Conflict Resolution Course Guidance Manual - Wirral University ...
Conflict Resolution Course Guidance Manual - Wirral University ...
Conflict Resolution Course Guidance Manual - Wirral University ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Clinical Education & Development Team<br />
Aggression Management Training<br />
National NHS Syllabus<br />
<strong>Conflict</strong> <strong>Resolution</strong> <strong>Course</strong> <strong>Guidance</strong><br />
<strong>Manual</strong>
FORWARD<br />
In April 2004 the National Health Service (NHS) launched the biggest training initiative in its history,<br />
with the aim of providing a minimum standard of training for all frontline staff (those who have contact<br />
with patients and the general public) in the recognition, prevention and management of violence,<br />
aggression and challenging behaviour.<br />
Awareness training in conflict resolution will be delivered across the NHS to approximately seven<br />
hundred thousand staff.<br />
This conflict resolution training (CRT) course has been developed in order to assist NHS staff when<br />
dealing with incidents that may have a potential for violence and aggression.<br />
It is important that NHS staff have provisions in place for a safe and secure working environment, in<br />
order to maintain excellence in standards for both personal and patient care.<br />
CRT provides staff with recognition signs and prevention measures that relate to the escalation and<br />
potential for violence and aggression.<br />
INTRODUCTION<br />
<strong>Wirral</strong> <strong>University</strong> Teaching Hospital (WUTH) NHS Foundation Trust’s Division of HR/OD have<br />
provided this Workbook which is now your property to keep, as such it has been designed to both<br />
compliment and assist in today’s National Syllabus <strong>Course</strong> on <strong>Conflict</strong> <strong>Resolution</strong>.<br />
Today’s course is to provide you with an understanding of the nature of workplace conflict, and the<br />
environmental and human factors that contribute to or influence it. Furthermore, the course will<br />
provide an understanding of the impacts and effects of workplace conflict on individual attitudes,<br />
behaviours and group performance both in and outside the workplace environment.<br />
You will learn how are communication patterns and responses to conflict influence our ability to<br />
resolve conflict and assist others. Through the use of communication models and the application of<br />
contemporary approaches to addressing workplace conflict you will experience how others may<br />
influence how we understand and act, and therefore ultimately how we deal with conflict.<br />
Areas are provided throughout the Workbook for you to make your own notes, should you wish to do<br />
so.<br />
The workbook contains valuable information, which you should use throughout your National Health<br />
Service career in order to assist you within your chosen workplace, in dealing with patients, visitors<br />
and also colleagues.<br />
<strong>Wirral</strong> <strong>University</strong> Teaching Hospital NHS Foundation Trust<br />
Aggression Management Training<br />
Clinical Education and Development Team<br />
Clinical Excellence<br />
HR/OD<br />
2
COURSE OBJECTIVES<br />
1. DEFINE THE COMMON CAUSES OF CONFLICT<br />
2. DESCRIBE THE TWO FORMS OF COMMUNICATION<br />
3. PROVIDE EXAMPLES OF HOW COMMUNICATION CAN BREAKDOWN<br />
4. EXPLAIN HOW COMMUNICATION MODELS CAN ASSIST IN CONFLICT RESOLUTION<br />
5. DESCRIBE PATTERNS OF BEHAVIOUR THAT MAY BE ENCOUNTERED DURING INTERARACTION<br />
6. GIVE EXAMPLES OF IMPACT FACTORS<br />
7. PROVIDE EXAMPLES OF WARNING AND DANGER SIGNS<br />
8. DESCRIBE THE USE OF A REACTIONARY GAP WHEN DEALING WITH CONFLICT<br />
9. DESCRIBE REASONABLE AND PROPORTIANATE FORCE APPLICABLE TO CONFLICT RESOLUTION<br />
10. DESCRIBE DIFFERENT METHODS FOR DEALING WITH POSSIBLE SITUATIONS OF CONFLICT<br />
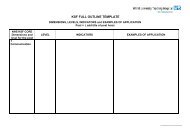
CONTENTS<br />
1. LEGAL DEFINITIONS OF CONFLICT<br />
• DEFINITIONS OF VIOLENCE, AGGRESSION, CHALLENGING BEHAVIOUR<br />
AND ZERO TOLERANCE<br />
• COMMON LAW<br />
• THE CRIMINAL LAW ACT 1974<br />
• THE NHS ZERO TOLERANCE CAMPAIGN<br />
• THE NHS COUNTER FRAUD SECURITY MANAGEMENT SERVICE<br />
• THE HUMAN RIGHTS ACT 1998<br />
2. COMMUNICATION<br />
• COMPONENTS OF COMMUNICATION<br />
• HOW WE COMMUNICATE<br />
• IDENTIFYING NON VERBAL COMMUNICATION<br />
(PICTURES AND CAPTIONS TO ASSIST COURSE CANDIDATES)<br />
3. COMMUNICATION MODELS<br />
• BETARIS BOX<br />
• FIVE STEP APPEAL<br />
• LEAPS<br />
• CUDSA<br />
4. REASONS FOR COMMUNICATION FAILURE<br />
• TRANSMITTER TO RECEIVER INTERFERENCE<br />
(MODEL FOR CANDIDATES TO PROVIDE REASONS TO WHY COMMUNICATION MAY FAIL)<br />
• CULTURAL DIVERSITY<br />
• PROXEMICS (DISTANCES)<br />
• CONFLICT<br />
• PERCEPTIONS (WHO’S TO BLAME)<br />
3
5. THE CONFLICT RESOLUTION MODEL<br />
• PATTERNS OF BEHAVIOUR<br />
• IMPACT FACTORS<br />
• WARNING SIGNS<br />
• DANGER SIGNS<br />
• THE REACYIONARY GAP<br />
• REASONABLE RESPONSE OPTIONS<br />
6. SCENARIOS<br />
7. CONCLUSION<br />
8. REFERENCES AND FURTHER READING<br />
9. ACKNOWLEDGEMENT<br />
VIOLENCE - Defined as an physical act<br />
Notes<br />
LEGAL DEFINITIONS OF CONFLICT<br />
AGGRESSION - Defined as an expressed emotion<br />
Notes<br />
CHALLENGING BEHAVIOUR - Any situation that denies access to or use of normal<br />
everyday available facilities<br />
Notes<br />
ZERO TOLERANCE – non-acceptance of any form of verbal abuse, racial abuse,<br />
threatening behaviour or use of violence and or aggression.<br />
Notes<br />
4
COMMON LAW – CRIMINAL LAW<br />
COMMON LAW:<br />
Common Law is each and every individual person’s right to protect him or her from being<br />
attacked and also to act in the defence of others.<br />
In order to be seen as lawful, any force that is used in defence of an attack must be reasonable to the<br />
circumstances and proportionate to the actual or perceived threat.<br />
Circumstances may justify a person striking first in defence of an attack.<br />
Common Law also recognises people’s acceptance and use of force against each other as say a<br />
sporting contest rather than a crime.<br />
Common Law is therefore interpreted according to the following guidelines:<br />
• If force is used it must be reasonable in the circumstances.<br />
• Any force that is used must also be proportionate to the threat.<br />
• Force may be justified in the prevention of serious evil.<br />
• Force can be used in defence of self or others.<br />
Notes<br />
SECTION THREE – CRIMINAL LAW ACT 1967:<br />
“A person may use such force as is reasonable in the circumstances in the prevention of crime, or in<br />
the effecting or assisting in the lawful arrest of offenders or suspected offenders or person’s<br />
unlawfully at large”<br />
Legislation on the reasonable use of force is the key facts that will be decided in each individual case<br />
were force has been used for lawful reason.<br />
Notes:<br />
5
THE NHS ZERO TOLERANCE CAMPAIGN<br />
In October of 1999 the Minister of State for Health launched the NHS Zero Tolerance<br />
Campaign in order to provide NHS staff with the knowledge and training in dealing with<br />
violence and aggression, and also to provide a multi – agency approach to dealing with<br />
offenders.<br />
Notes:<br />
THE NHS COUNTER FRAUD SECURITY MANAGEMENT SERVICE<br />
In January 2003 the House of Commons ordered a report on Protecting NHS Hospital Staff.<br />
The National Audit Office were commissioned to carry out the report, The N.A.O. produced the report<br />
on the 24 th March 2003.<br />
It states:<br />
“From April 2003, the new Counter Fraud and Security Management Service, which was established<br />
as a Special Health Authority in January 2003, will take over responsibility for all policy and<br />
operational matters relating to the management of security in the NHS including leading the work on<br />
reducing violence and aggression against NHS staff”<br />
The C.F.S.M.S. policy guidelines state that all NHS Trusts should:<br />
“Take a more strategic approach to induction and other Aggression Management training, based on<br />
an annual training need analysis for all clinical and support staff”<br />
Notes:<br />
6
THE HUMAN RIGHTS ACT 1998<br />
Human Rights describe workplace violence as:<br />
“Any incident where staff are abused, threatened or assaulted in circumstances related to their<br />
work”<br />
“This can involve an explicit (direct) or implicit (unspoken) challenge to a person’s safety, well-being<br />
or health”<br />
Notes:<br />
COMPONENTS OF COMMUNICATION<br />
7%<br />
NVC's<br />
Vocals<br />
Spoken Word<br />
8%<br />
55%<br />
NOTES:<br />
7
COMMUNICATION<br />
COMMUNICATION<br />
NON – VERBAL<br />
(BODY LANGUAGE)<br />
VERBAL<br />
(SPOKEN)<br />
NON - VERBAL COMMUNICATION (NVC)<br />
Signals that each person sends through use of body language that is interpreted above spoken<br />
words by one another<br />
Notes:<br />
IDENTIFYING NON – VERBAL COMMUNICATION<br />
I’m not angry<br />
or aggressive<br />
Comments:<br />
I’m listening<br />
and I agree<br />
Comments:<br />
8
I’m interested,<br />
I want to help<br />
Comments:<br />
I’m fine I’m<br />
not worried<br />
Comments:<br />
BETARIS BOX<br />
MY My ATTITUDE Attitude My<br />
YOUR BEHAVIOUR<br />
MY BEHAVIOUR<br />
YOUR ATTITUDE<br />
Your attitude or emotions if perceived by another to be hostile will be displayed in your behaviour.<br />
This will affect the attitude or emotions of the person you are communicating with, the affect will be<br />
noticeable through their behaviour.<br />
This will then further affect your attitude and behaviour and so on.<br />
You must recognise this cycle and take responsibility for breaking it in order to move forward with<br />
communication.<br />
Notes:<br />
9
FIVE STEP APPEAL<br />
A mediation system that can be used when a person’s resistance persists or increases during<br />
communication<br />
STEP ONE - SIMPLE APPEAL<br />
Notes:<br />
STEP TWO - REASONED APPEAL<br />
Notes:<br />
STEP THREE – PERSONAL APPEAL<br />
Notes:<br />
STEP FOUR - PRACTICAL APPEAL<br />
Notes:<br />
STEP FIVE – FINAL APPEAL<br />
Notes:<br />
10
LEAPS<br />
When applied in an appropriate manner the LEAPS communication model will provide a useful and<br />
professional aid to resolving differing situations of conflict within the working environment.<br />
Notes:<br />
L<br />
Notes:<br />
E<br />
Notes:<br />
A<br />
Notes:<br />
P<br />
Notes:<br />
S<br />
11
CUDSA<br />
CUDSA is a communication model that has been specifically designed for dealing with conflict<br />
Notes<br />
C<br />
Notes<br />
U<br />
Notes<br />
D<br />
Notes<br />
S<br />
Notes<br />
A<br />
12
REASONS FOR COMMUNICATION FAILURE<br />
BODY POSTURE-Aggressive Stance, Facial Expression<br />
VOICE- Tone, Volume<br />
COMMUNICATION- Lack of Information (waiting times), Technical Terminology, Language<br />
Differences, Stereotyping<br />
ENVIRONMENT- Boredom – TV, Magazines, Literature, Under High Levels of Stress, Background<br />
Noise, Exposed to Strange Environments, Affected by Alcohol/Drugs, Experiencing Pain. An<br />
Enjoyment for Confrontation, Subject to Rapid Mood Swings, A History of Mental Disorder.<br />
The itemised list is not exhaustive and each individual situation may present differing problems when<br />
attempting to effect communication.<br />
Understanding what situations may lead to communication failure will assist in the prevention of the<br />
recognised causes of potential conflict.<br />
Notes:<br />
TRANSMITTER TO RECEIVER INTERFERENCE<br />
During verbal or non- – verbal communication interference can take place between the person who<br />
receives the message, and the person who is sending or transmitting the message.<br />
MESSAGE<br />
TRANSMITTER<br />
RECEIVER<br />
MESSAGE<br />
Use the box below to list the various forms of interference that may prevent a transmitter message<br />
from being correctly received:<br />
Notes:<br />
13
CULTURAL DIVERSITY<br />
The diversity within cultures is noticeable through the use of body language perceptions. Some<br />
cultures will avoid direct eye contact as an individual sign of respect, while other cultures may<br />
perceive this action as conflicting with anything verbal and therefore see the person as untruthful.<br />
In some cultures the invasion of an individual’s personal space by a stranger would be viewed as a<br />
totally inappropriate action, while other cultures would find it totally acceptable.<br />
In greeting a person some cultures will place a kiss on the cheek followed by an embrace of the<br />
person, while in other cultures a nod of the head or handshake would be viewed as appropriate.<br />
Body language can therefore be perceived as different from that which is actually spoken or intended<br />
to be said.<br />
Use the box to provide examples:<br />
Notes:<br />
PROXEMICS - DISTANCES<br />
Distances are used to allow us time to think and react, in certain conditions it would be natural for us<br />
to allow some people closer, while we will keep others at a distance.<br />
Performing your role within the working environment can be the exception to the above rule as<br />
conditions dictate that we maintain close proximity in order to provide quality care or carry out a<br />
necessary procedure.<br />
INTIMATE ZONE<br />
CLOSE FAMILY - PARTNER<br />
LESS THAN 18 INCHES<br />
PERSONAL ZONE<br />
FRIENDS AND COLLEAGUES<br />
18 INCHES TO 4 FOOT<br />
SOCIAL ZONE<br />
ALL OTHER PEOPLE<br />
4 FOOT TO 12 FOOT<br />
14
Notes:<br />
CONFLICT<br />
It must be stressed that there is no singular 'right response' for any given situation. The decisions of<br />
each and every person at an incident are governed by their individual perception at that time, as each<br />
person may perceive the person's behaviour in a different way.<br />
Because of the differing factors in relation to the behaviour of the person, each involved individual<br />
may perceive the risk or threat to be either higher or lower than that of colleagues. The differing<br />
physical abilities of each person involved in an incident will also have an impact on individual actions.<br />
Therefore, the same set of circumstances may be met in many different individually perceived ways.<br />
The aspects of communication that we have so far covered provide recognition of the different<br />
elements of conflict and the knowledge required in order to avoid escalation of conflict, however,<br />
when communication appears to be failing a person should consider other appropriate response<br />
options within personal limitations and requirements.<br />
Provide a list of other appropriate response options:<br />
Notes:<br />
PERCEPTIONS - WHO'S TO BLAME<br />
Anne had been involved for three months with the voluntary drug support team, although Anne was<br />
new to the work and unqualified she enjoyed it and wanted to be well regarded by the rest of the<br />
team. The team was allocated to cover a large run down housing estate where unemployment,<br />
violence, and drug abuse were common problems.<br />
Tom, an experienced voluntary worker had himself been brought up in a similar disadvantaged<br />
housing estate. Tom prided himself on his ability to 'tough out' even the most difficult, confrontational<br />
situations, having been a team leader since the project had started he always encouraged his team<br />
to adopt the same attitude as himself when dealing with confrontation.<br />
Phil was a known long-term drug user. His behaviour had, over the years led to his removal from a<br />
number of GP' lists, given his use of violence and intimidation to get his own way. Following another<br />
recent incident over a drugs prescription, Phil was again in danger of being struck off from a surgery<br />
practice by the GP.<br />
15
Worried about his imminent lack of support, Jane, the Community Psychiatric Nurse, who covered<br />
the practice, wrote a brief note referring him to the Drug Support Team.<br />
Upon receiving the note, Tom asked Anne to take the referral.<br />
Prior to making a home visit, Anne casually mentioned the referral to her colleague Steve, Who<br />
incidentally knew the family well, laughing; Steve suggested that she might find the visit a 'lively one!'<br />
Having no information, which suggested particular difficulties and not wanting to appear anxious or<br />
over concerned, Anne said nothing.<br />
During the interview Phil became evasive about many aspects of his social history.<br />
Concerned to undertake a competent first assessment, Anne persisted in her questioning although<br />
Phil was clearly becoming agitated.<br />
As Anne continued to question Phil, he became increasingly verbally abusive until, losing control<br />
completely he picked up a large glass ashtray, and with considerable force struck Anne across the<br />
face with it.<br />
WHO IS TO BLAME <br />
THE CONFLICT RESOLUTION MODEL<br />
PERSON’S<br />
BEHAVIOUR<br />
IMPACT<br />
FACTORS<br />
REASONABLE<br />
RESPONSE<br />
OPTIONS<br />
RESPONSE<br />
OPTIONS<br />
16
PATTERNS OF BEHAVIOUR<br />
This is a list showing a scale of possible behaviours that may be encountered during conflict.<br />
A. Compliant behaviour<br />
‣ The person is confrontational but complies with requests.<br />
B. Verbal with gestures<br />
‣ The person refuses to comply verbally or by their body language.<br />
C. Passive behaviour<br />
‣ The person sits or stands and will not move.<br />
D. Active behaviour<br />
‣ The person pulls or pushes but makes no attempt to strike out.<br />
E. Aggressive behaviour<br />
‣ The person physically attacks the member of staff.<br />
F. Serious or Aggravated behaviour<br />
‣ The person commits an assault, which presents the possibility of serious injury or death.<br />
‣ This resistance may include the use of weapons.<br />
‣ The person offending may exhibit these behaviours in a progressive pattern.<br />
‣ It is not unusual for a person to jump several stages in the scale if the occasion demands it.<br />
‣<br />
Notes:<br />
IMPACT FACTORS<br />
The following is a list of possible Impact Factors:<br />
• Relative sex, age, size of member of staff and person<br />
• Relative strength of member of staff and person<br />
• Relative skill level of member of staff and person<br />
• Exhaustion or Injury<br />
• Number of people involved<br />
17
• Special knowledge<br />
• Alcohol or Drugs<br />
• Mental state<br />
• Weapons<br />
• Perceived imminent danger<br />
• Being in a position of perceived disadvantage<br />
• Perception on obtaining help or assistance<br />
Notes:<br />
WARNING SIGNS<br />
As a general rule people who are going to attack another person engage in actions known as<br />
'Ritualised Combat'.<br />
This may be because they fear being injured themselves.<br />
Identifying these non-verbal signals may give staff a significant advantage.<br />
They are:<br />
♦ Direct prolonged eye contact<br />
♦ Changed facial colour<br />
♦ Head held back<br />
♦ Maximises height by standing tall<br />
♦ Kicking the ground<br />
♦ Exaggerated movements near you especially with the hands<br />
♦ Accelerated breathing rate<br />
♦ Abrupt stopping and starting of nervous behaviour such as tapping of fingers<br />
THIS IS NOT AN EXHAUSTIVE LIST.<br />
In addition to the above behaviour the person may indicate that they perceive a particular member of<br />
staff as being the problem, they will then direct any aggression toward that person.<br />
This is known as 'Personal Identification' or personalisation of anger.<br />
When this personal identification takes place it is usually a strong indication that the person may be<br />
approaching the point of violence.<br />
At this point staff should manage and maintain the 'Reactionary Gap'.<br />
The 'reactionary gap' is the distance from the extremity of the member of staff's reach to the extremity<br />
of the person's reach<br />
18
DANGER SIGNS<br />
As the word danger implies the signs listed here have a much higher impact potential than the<br />
warning signs.<br />
WHEN THESE SIGNS OCCUR, ATTACK MAY BE IMMINENT, THEREFORE POSITIVE ACTION<br />
IS CRUCIAL IN ORDER TO AVOID OR REDUCE THE RISK OF INJURY.<br />
Neglecting or ignoring these signs MAY place a person at a serious disadvantage.<br />
They are:<br />
Fists clenching/unclenching<br />
Changed facial colour<br />
Lips tightening over teeth<br />
Head dropping forward to protect throat<br />
Eyebrows dropping to protect eyes<br />
Hands moving to above the waist<br />
Shoulders tensing<br />
Stance changing to side on or fighting stance<br />
Glancing at intended target areas<br />
Lowering of entire body before launching an attack<br />
THERE MAY BE OTHER SIGNS.<br />
On witnessing these signs staff may opt for the following positive option:<br />
‣ Disengaging in order to establish an effective reactionary gap.<br />
The option may have both positive and negative aspects and the choice must be made on your<br />
individual perceptions of the most appropriate response, taking into account all of the circumstances.<br />
Notes:<br />
REACTIONARY GAP<br />
The distance we should use when dealing with conflict.<br />
The distance between the extremity of your reach and the extremity of an aggressor’s reach<br />
Notes:<br />
19
REASONABLE RESPONSE OPTION<br />
Maintain self-control and:<br />
Signal non aggressions<br />
Request behaviour to stop<br />
Be assertive<br />
Use tactical communication<br />
Remind the aggressor what they have to lose<br />
Use diversionary techniques<br />
Hands On - as a last resort<br />
Notes:<br />
SCENARIOS<br />
The aspects of communication that we have so far covered provide recognition of the different<br />
elements of conflict and the knowledge required in order to avoid escalation of conflict, however,<br />
when communication appears to be failing a person should consider other appropriate response<br />
options within personal limitations and requirements.<br />
Provide a list of other appropriate response options:<br />
Notes:<br />
SECONDARY CARE NHS ACUTE TRUSTS<br />
A patient arrives by ambulance to Accident and Emergency and is placed in a cubicle for treatment to<br />
take place, when a group of friends arrive and demand to see him; they surround a member of staff<br />
and begin shouting.<br />
Notes:<br />
20
Upon arriving for duty, you see two male youths outside the entrance you must use to get to Accident<br />
and Emergency.<br />
As you get closer you notice that both males are bleeding from facial injuries, and that one male is<br />
verbally abusing people as they try to get past him into the department.<br />
Notes:<br />
A patient who has waited two hours to see a doctor has approached a colleague and wants to know<br />
how much longer he will have to wait.<br />
The patient claims that he is being victimised, and deliberately left to wait by your colleague due to an<br />
earlier encounter in which the conversation became heated, your colleague is offended by the<br />
patient’s attitude and reacts by aggressively arguing back.<br />
Notes:<br />
A concerned father has gone to park his car after dropping both his wife and ill daughter off at the<br />
entrance to Accident and Emergency.<br />
Mother and daughter are told to take a seat in the waiting area and do so; they are immediately<br />
harassed by a group of three teenage males.<br />
The father arrives, angry to see his wife and daughter upset he say’s that if know one will do anything<br />
about it then he will and threatens the teenagers with violence, they immediately respond by taunting<br />
him.<br />
Notes:<br />
AMBULANCE TRUSTS<br />
You arrive at a road traffic accident and having checked all those involved, you start to treat an<br />
elderly female who is sat in the driving seat of one of the vehicles involved.<br />
A younger female demands that you stop what you are doing and that you see to her friend in<br />
another vehicle, she then attacks the elderly driver shouting that it was her fault in the first place.<br />
Notes:<br />
21
A GP has called you to an elderly couple’s house to take a patient to hospital.<br />
The husband is crying and refuses to listen to the doctor’s explanation that his wife needs urgent<br />
medical care.<br />
The husband stands between you and the patient with a raised walking stick and demands that you<br />
leave.<br />
Note:<br />
You arrive outside a nightclub following an anonymous phone call, to find a man with severe head<br />
injuries, a group of drunken friends don’t see the serious of his condition and claim he just needs to<br />
sleep of the beer that he has drank.<br />
One friend seems prepared to listen, but the others refuse to allow you to take him to hospital and tell<br />
you to leave, your colleague goes to the ambulance and calls control.<br />
The group surrounds you and become offensive and verbally aggressive.<br />
Notes<br />
Having just escorted a patient into hospital, you are returning alone to your vehicle at the main<br />
entrance when you see a female searching inside the parked ambulance.<br />
As you approach she turns to face you and you see she is holding a knife, she demands to know<br />
where the drugs are kept and threatens self harm if you don’t tell her.<br />
Notes:<br />
CONCLUSION<br />
‣ We have looked at how to recognise the different ways in which people may communicate.<br />
‣ We have learnt how to recognise different warning and danger signals and what they mean.<br />
‣ We have learnt about different communication models and methods to know when to use<br />
them.<br />
‣ We have looked at the importance of how different impact factors can affect behaviour.<br />
22
‣ We have studied distances and how they should be applied when dealing with conflict.<br />
‣ We have discussed the law as it applies to reasonable and proportionate force.<br />
‣ We have learnt to recognise that no two incident will be the same and will therefore be viewed<br />
differently by each person involved.<br />
WUTH NHS Foundation Trust thank you for your participation in today’s course, and sincerely hope<br />
that you benefit from all the elements of what has been examined regarding conflict resolution.<br />
Should you have any comments regarding this course or wish to participate in further aggression<br />
management training, please contact:<br />
Joe McLaughlin LSMS<br />
Aggression Management Training<br />
Clinical Education and Development Team<br />
Clinical Excellence<br />
Division of HR/OD<br />
Clinical Skills Centre<br />
Arrowe Park Hospital<br />
Upton<br />
Ext. 2779. Bleep 4471<br />
REFERENCES AND FURTHER READING<br />
• Criminal Law Act 1967 - Section 3: (1)<br />
• Molan’s “Criminal/Common Law” - 10 Edition (1996/97)<br />
• Baillie, D. “Practice” – Human Rights Act 1998<br />
• CFSMS “A professional approach to managing security in the NHS”<br />
• NAO “A safer place to work”<br />
• Centrex Trainers Development Programme<br />
• Argyle, M. “Bodily Communication” - Methuen (1975)<br />
• Birdwhistell, R.L. “Human Communication”<br />
• Clayton, P. “Body Language at Work” – Hamlyn (2002)<br />
• Hall, E.T. “Silent Language and Proxemics” – Doubleday (1954)<br />
• Axtell, R. “Gestures: Do’s and Taboos of Body Language” – John Wiley<br />
•<br />
ACKNOWLEDGEMENT<br />
On behalf of <strong>Wirral</strong> <strong>University</strong> Teaching Hospital NHS Foundation Trust the course instructor both<br />
acknowledges and thanks Christopher McCarthy from Merseyside Police for all his respected advice<br />
and gratefully received assistance with the personal development of aggression management<br />
training.<br />
Joe McLaughlin<br />
23