Neonatal Jaundice - Associates in Newborn Medicine
Neonatal Jaundice - Associates in Newborn Medicine
Neonatal Jaundice - Associates in Newborn Medicine

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
neonatology<br />
neonatal jaundice<br />
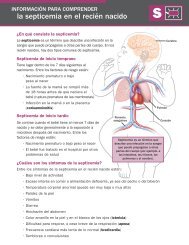
Table 3. Criteria for Diagnos<strong>in</strong>g<br />
ABO Hemolytic Disease as the<br />
Cause of <strong>Neonatal</strong><br />
Hyperbilirub<strong>in</strong>emia<br />
Mother group O, <strong>in</strong>fant group A or B<br />
AND<br />
● Positive DAT<br />
● <strong>Jaundice</strong> appear<strong>in</strong>g with<strong>in</strong> 12 to 24 h after birth<br />
● Microspherocytes on blood smear<br />
● Negative DAT but homozygous for Gilbert<br />
syndrome<br />
Repr<strong>in</strong>ted with permission from Maisels MJ. <strong>Jaundice</strong>. In: MacDonald<br />
MG, Seshia MMK, Mullett MD, eds. Neonatology: Pathophysiology and<br />
Management of the <strong>Newborn</strong>. Philadelphia, Pa: Lipp<strong>in</strong>cott Co;<br />
2005:768–846.<br />
<strong>in</strong>crease <strong>in</strong> TSB concentrations with<strong>in</strong> the first 24 hours,<br />
but the TSB subsequently decl<strong>in</strong>es, <strong>in</strong> many <strong>in</strong>fants,<br />
often without any <strong>in</strong>tervention. ABO hemolytic disease is<br />
a relatively common cause of early hyperbilirub<strong>in</strong>emia<br />
(before the <strong>in</strong>fant leaves the nursery), but it is a relatively<br />
rare cause of hyperbilirub<strong>in</strong>emia <strong>in</strong> <strong>in</strong>fants who have been<br />
discharged and readmitted. The criteria for diagnos<strong>in</strong>g<br />
ABO hemolytic disease as the cause of neonatal hyperbilirub<strong>in</strong>emia<br />
are listed <strong>in</strong> Table 3. Recently, it has been<br />
shown that DAT-negative, ABO-<strong>in</strong>compatible <strong>in</strong>fants<br />
who also have Gilbert syndrome are at risk for hyperbilirub<strong>in</strong>emia.<br />
This may expla<strong>in</strong> the occasional ABO<strong>in</strong>compatible<br />
<strong>in</strong>fant who has a negative DAT and nevertheless<br />
develops early hyperbilirub<strong>in</strong>emia.<br />
Glucose-6-phosphate Dehydrogenase (G-6PD)<br />
Deficiency<br />
G-6PD deficiency is the most common and cl<strong>in</strong>ically<br />
significant red cell enzyme defect, affect<strong>in</strong>g as many as<br />
4,500,000 newborns worldwide each year. Although<br />
known for its prevalence <strong>in</strong> the populations of the Mediterranean,<br />
Middle East, Arabian Pen<strong>in</strong>sula, southeast<br />
Asia, and Africa, G-6PD has been transformed by immigration<br />
and <strong>in</strong>termarriage <strong>in</strong>to a global problem. Nevertheless,<br />
most pediatricians <strong>in</strong> the United States do not<br />
th<strong>in</strong>k of G-6PD deficiency when confronted with a jaundiced<br />
<strong>in</strong>fant. This possibility should be considered,<br />
though, particularly when see<strong>in</strong>g African-American <strong>in</strong>fants.<br />
Although African-American newborns, as a group,<br />
tend to have lower TSB concentrations than do caucasian<br />
newborns, G-6PD deficiency is found <strong>in</strong> 11% to 13% of<br />
African-American newborns. This translates to 32,000 to<br />
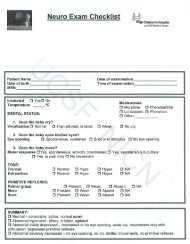
Table 4. Major Cl<strong>in</strong>ical Features<br />
of Acute Bilirub<strong>in</strong><br />
Encephalopathy<br />
Initial Phase<br />
● Slight stupor (“lethargic,” “sleepy”)<br />
● Slight hypotonia, paucity of movement<br />
● Poor suck<strong>in</strong>g, slightly high-pitched cry<br />
Intermediate Phase<br />
● Moderate stupor—irritable<br />
● Tone variable, usually <strong>in</strong>creased; some have<br />
retrocollis-opisthotonos<br />
● M<strong>in</strong>imal feed<strong>in</strong>g, high-pitched cry<br />
Advanced Phase<br />
● Deep stupor to coma<br />
● Tone usually <strong>in</strong>creased; some have retrocollisopisthotonos<br />
● No feed<strong>in</strong>g, shrill cry<br />
Repr<strong>in</strong>ted with permission from Maisels MJ. <strong>Jaundice</strong>. In: MacDonald<br />
MG, Seshia MMK, Mullett MD, eds. Neonatology: Pathophysiology and<br />
Management of the <strong>Newborn</strong>. Philadelphia, Pa: Lipp<strong>in</strong>cott Co;<br />
2005:768–846.<br />
39,000 African-American male G-6PD-deficient hemizygous<br />
newborns born annually <strong>in</strong> the United States. As<br />
many as 30% of <strong>in</strong>fants <strong>in</strong> the United States who have<br />
kernicterus have been found to be G-6PD-deficient.<br />
The G-6PD gene is located on the X chromosome,<br />
and hemizygous males have the full enzyme deficiency,<br />
although female heterozygotes are also at risk for hyperbilirub<strong>in</strong>emia.<br />
G-6PD-deficient neonates have an <strong>in</strong>crease<br />
<strong>in</strong> heme turnover, although overt evidence of<br />
hemolysis often is not present. In addition, affected<br />
<strong>in</strong>fants have an impaired ability to conjugate bilirub<strong>in</strong>.<br />
Bilirub<strong>in</strong> Encephalopathy<br />
In the case described at the beg<strong>in</strong>n<strong>in</strong>g of this article, the<br />
<strong>in</strong>fant developed extreme hyperbilirub<strong>in</strong>emia and the<br />
classic signs of acute bilirub<strong>in</strong> encephalopathy (Table 4).<br />
He also developed the typical features of chronic bilirub<strong>in</strong><br />
encephalopathy or kernicterus (Table 5).<br />
How Could This Have Been Prevented<br />
The <strong>in</strong>fant <strong>in</strong> the case report had many of the factors that<br />
<strong>in</strong>crease the risk of severe hyperbilirub<strong>in</strong>emia (Table 6).<br />
A key recommendation <strong>in</strong> the American Academy of<br />
Pediatrics (AAP) cl<strong>in</strong>ical practice guidel<strong>in</strong>e (Table 7) is<br />
that every <strong>in</strong>fant be assessed for the risk of subsequent<br />
severe hyperbilirub<strong>in</strong>emia before discharge, particularly<br />
446 Pediatrics <strong>in</strong> Review Vol.27 No.12 December 2006<br />
Downloaded from http://peds<strong>in</strong>review.aappublications.org by J Michael Coleman on June 4, 2010