Laboratory diagnosis of SARS-coronavirus infectieons
Laboratory diagnosis of SARS-coronavirus infectieons
Laboratory diagnosis of SARS-coronavirus infectieons

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
disease focus<br />
S ARS<br />
<strong>Laboratory</strong> <strong>diagnosis</strong> <strong>of</strong> <strong>SARS</strong><strong>coronavirus</strong><br />
infections<br />
by Karen Sonnenberg<br />
as published in CLI September 2004<br />
<strong>SARS</strong>-<strong>coronavirus</strong> (<strong>SARS</strong>-CoV) is the infectious agent responsible for the recent epidemic outbreak <strong>of</strong> severe acute respiratory<br />
syndrome (<strong>SARS</strong>). In an impressively short time after the discovery <strong>of</strong> the virus, molecular and serological tests were<br />
developed. <strong>Laboratory</strong> <strong>diagnosis</strong> using these tests became extremely important in identifying or confirming infections with<br />
<strong>SARS</strong>-CoV. PCR-based tests have been shown to be powerful tools for detecting <strong>SARS</strong>-CoV early after disease onset, whereas<br />
from day 10 after the onset <strong>of</strong> symptoms, the detection <strong>of</strong> specific antibodies is the preferred diagnostic approach.<br />
The first cases <strong>of</strong> <strong>SARS</strong> appeared in southern China in November 2002. In<br />
March 2003 the causative agent <strong>of</strong> this disease was identified as a novel<br />
<strong>coronavirus</strong>. Since its first reported occurrence in humans, the virus has<br />
infected more than 8000 people and caused more than 750 deaths. Between<br />
February 2003 and June 2003 cases <strong>of</strong> the disease were predominantly<br />
reported in Asia, but were also reported in North America and Europe.<br />
<strong>SARS</strong>-CoV is spread mainly by close person-to-person contact, for example,<br />
through respiratory secretions from coughing or sneezing. The virus<br />
can also spread from surfaces or objects contaminated with infectious<br />
droplets. The incubation period for <strong>SARS</strong> is typically 2-7 days, after which<br />
patients develop high fever (>38°C) and respiratory symptoms, mainly<br />
pneumonia. About 10 to 20 percent <strong>of</strong> patients have diarrhoea. Other<br />
symptoms are headache, an overall feeling <strong>of</strong> discomfort and body aches.<br />
The overall mortality from <strong>SARS</strong> is around 10%, with levels as high as 50%<br />
in the over-65 age group. Currently there is no specific and effective therapy<br />
or method <strong>of</strong> prevention for <strong>SARS</strong>.<br />
The initial <strong>diagnosis</strong> <strong>of</strong> <strong>SARS</strong> was based on clinical and epidemiological<br />
criteria. During the initial outbreak, molecular and serological tests for<br />
detecting infections with the <strong>SARS</strong>-CoV were developed. Direct or indirect<br />
identification <strong>of</strong> the virus by these diagnostic tests has become an important<br />
means <strong>of</strong> diagnosing the disease, <strong>of</strong> understanding the pathways <strong>of</strong><br />
transmission, and <strong>of</strong> studying <strong>SARS</strong> epidemiology.<br />
<strong>SARS</strong> case definitions<br />
<strong>SARS</strong> cases are classified as suspect or probable based on clinical, epidemiological<br />
and laboratory criteria [1] defined by the World Health<br />
Organisation (WHO) [Figure 2]. A suspected case <strong>of</strong> <strong>SARS</strong> that is positive<br />
for <strong>SARS</strong> <strong>coronavirus</strong> by one or more assays [Table 1] is classified as a<br />
probable case.<br />
<strong>Laboratory</strong> methods for confirmation <strong>of</strong> suspected cases: PCR for<br />
<strong>SARS</strong>-CoV<br />
The polymerase chain reaction (PCR) allows direct detection <strong>of</strong> <strong>SARS</strong>-CoV<br />
genetic material in various patient specimens, such as blood, stool, respiratory<br />
secretions or body tissues. Positive PCR results are very specific and<br />
mean that there is genetic material (RNA) <strong>of</strong> the <strong>SARS</strong>-CoV in the sample.<br />
This does not necessarily mean that the active virus is present, or that it is<br />
present in a quantity great enough to infect another person.<br />
Negative PCR results cannot exclude the presence <strong>of</strong> the <strong>SARS</strong>-CoV in a<br />
patient. Besides the possibility <strong>of</strong> obtaining false-negative test results, specimens<br />
may not have been collected at a time when sufficient virus or its<br />
genetic material was present. The sensitivity <strong>of</strong> PCR tests for <strong>SARS</strong> depends<br />
both on the type <strong>of</strong> specimen and the time <strong>of</strong> testing during the course <strong>of</strong><br />
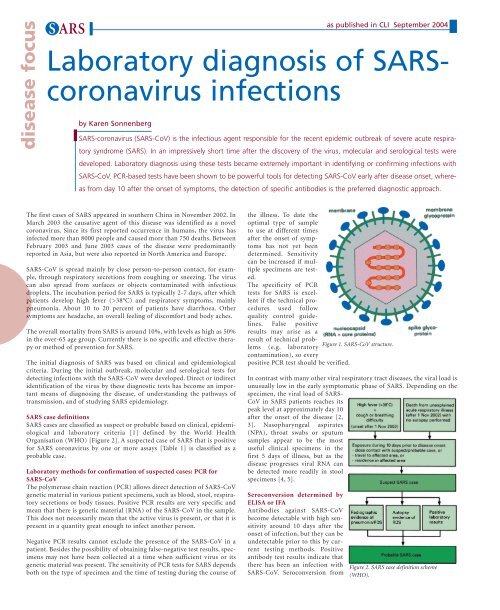
the illness. To date the<br />
optimal type <strong>of</strong> sample<br />
to use at different times<br />
after the onset <strong>of</strong> symptoms<br />
has not yet been<br />
determined. Sensitivity<br />
can be increased if multiple<br />
specimens are tested.<br />
The specificity <strong>of</strong> PCR<br />
tests for <strong>SARS</strong> is excellent<br />
if the technical procedures<br />
used follow<br />
quality control guidelines.<br />
False positive<br />
results may arise as a<br />
result <strong>of</strong> technical problems<br />
(e.g. laboratory<br />
Figure 1. <strong>SARS</strong>-CoV structure.<br />
contamination), so every<br />
positive PCR test should be verified.<br />
In contrast with many other viral respiratory tract diseases, the viral load is<br />
unusually low in the early symptomatic phase <strong>of</strong> <strong>SARS</strong>. Depending on the<br />
specimen, the viral load <strong>of</strong> <strong>SARS</strong>-<br />
CoV in <strong>SARS</strong> patients reaches its<br />
peak level at approximately day 10<br />
after the onset <strong>of</strong> the disease [2,<br />
3]. Nasopharyngeal aspirates<br />
(NPA), throat swabs or sputum<br />
samples appear to be the most<br />
useful clinical specimens in the<br />
first 5 days <strong>of</strong> illness, but as the<br />
disease progresses viral RNA can<br />
be detected more readily in stool<br />
specimens [4, 5].<br />
Seroconversion determined by<br />
ELISA or IFA<br />
Antibodies against <strong>SARS</strong>-CoV<br />
become detectable with high sensitivity<br />
around 10 days after the<br />
onset <strong>of</strong> infection, but they can be<br />
undetectable prior to this by current<br />
testing methods. Positive<br />
antibody test results indicate that<br />
there has been an infection with<br />
<strong>SARS</strong>-CoV. Seroconversion from<br />
Figure 2. <strong>SARS</strong> case definition scheme<br />
(WHO).
S ARS<br />
as published in CLI September 2004<br />
<strong>Laboratory</strong> methods<br />
A. Confirmed positive<br />
PCR for <strong>SARS</strong>-CoV<br />
B. Seroconversion by<br />
ELISA or IFA<br />
C. Virus isolation<br />
WHO recommendations on interpretation <strong>of</strong> laboratory results<br />
At least two different clinical specimens (e.g. nasopharyngeal<br />
and stool)<br />
OR<br />
the same clinical specimen collected on two or more days<br />
during the course <strong>of</strong> the illness (e.g. two or more nasopharyngeal<br />
aspirates)<br />
OR<br />
two different assays or repeat PCR using the original clinical<br />
sample on each occasion <strong>of</strong> testing<br />
Negative antibody test on acute serum followed by positive<br />
antibody test on convalescent serum<br />
OR<br />
four-fold or greater rise in antibody titre between acute and<br />
convalescent phase sera tested in parallel<br />
Isolation in cell culture <strong>of</strong> <strong>SARS</strong>-CoV from any specimen<br />
AND<br />
PCR confirmation using a validated method<br />
Table 1. <strong>Laboratory</strong> methods for confirmation <strong>of</strong> suspected cases.<br />
negative to positive, or a four-fold rise in antibody titre in the serum <strong>of</strong> a<br />
convalescent patient compared with that patient’s serum during acute illness,<br />
denotes a recent infection. A negative serological result 21 days after<br />
onset <strong>of</strong> symptoms indicates absence <strong>of</strong> <strong>SARS</strong>-CoV infection. Cross-reactions<br />
with antibodies to other agents (including the human <strong>coronavirus</strong>es<br />
HCoV-229E and HCoV-OC43) are not known. Several serological studies<br />
with <strong>SARS</strong> patient sera using immun<strong>of</strong>luorescence tests (IIFT) and/or<br />
ELISA showed sensitivities between 92 and 99% [3, 4, 6, 7]. A comparison<br />
<strong>of</strong> IIFT, ELISA and PCR [Figure 5] showed that PCR predominantly<br />
enables fresh infections to be identified. In later stages <strong>of</strong> the illness (∼10<br />
days after onset) antibody determination using IIFT or ELISA is the most<br />
reliable method for identifying infections with <strong>SARS</strong>-CoV.<br />
Virus isolation<br />
The presence <strong>of</strong> the infectious virus can be detected by inoculating suitable<br />
cell cultures (e.g. Vero cells) with patient specimens (e.g. respiratory<br />
secretions, blood or stool) and propagating the virus in vitro. Cell culture<br />
is a very demanding test. Once isolated, the virus must be identified as<br />
<strong>SARS</strong>-CoV using further tests (predominantly nucleic acid-based).<br />
Positive results indicate the presence <strong>of</strong> living <strong>SARS</strong>-CoV in the sample.<br />
Negative cell culture results do not necessarily exclude <strong>SARS</strong>, as discussed<br />
previously.<br />
Differential <strong>diagnosis</strong><br />
According to the WHO <strong>SARS</strong> case definition, a case should be excluded if<br />
an alternative <strong>diagnosis</strong> can fully explain the illness. For example, influenza<br />
viruses, parainfluenza viruses, Chlamydia pneumoniae, Mycoplasma<br />
pneumoniae and Legionella pneumophila can also cause atypical pneumonia.<br />
Positive laboratory test results for these agents may serve as exclusion<br />
criteria.<br />
Figure 5. Comparison <strong>of</strong> Euroimmun IIFT, ELISA and PCR results from 34 sera <strong>of</strong> <strong>SARS</strong><br />
patients.<br />
Every laboratory confirmation<br />
<strong>of</strong> <strong>SARS</strong> should<br />
be undertaken in a<br />
national or regional reference<br />
laboratory and<br />
reported to the WHO.<br />
The WHO encourages<br />
each country to designate<br />
a laboratory at national<br />
level for the investigation<br />
and shipment <strong>of</strong> specimens<br />
from possible <strong>SARS</strong> Figure 3. PCR amplification <strong>of</strong> <strong>SARS</strong>-CoV nucleic acids.<br />
patients. Furthermore, members <strong>of</strong> the WHO network laboratories [8] have<br />
agreed to test samples <strong>of</strong> suspected or probable <strong>SARS</strong> patients from countries<br />
which may not have the laboratory capacity (PCR technology and biosafety<br />
level 3). Guidelines for the safe handling <strong>of</strong> <strong>SARS</strong> specimens are also<br />
described on the WHO web site [9].<br />
References<br />
1. World Health Organisation. Case definitions for surveillance <strong>of</strong> severe acute respiratory<br />
syndrome (<strong>SARS</strong>). www.who.int/csr/sars/casedefinition/en<br />
2. Peiris JS, Chu CM, Cheng<br />
VC, et al. Clinical progression<br />
and viral load in a community<br />
outbreak <strong>of</strong> <strong>coronavirus</strong>-associated<br />
<strong>SARS</strong><br />
pneumonia: a prospective<br />
study. Lancet 2003; 361:<br />
1767-72<br />
3. Tang P, Louie M,<br />
Richardson SE, Smieja M,<br />
Simor AE, Jamieson F, et al.<br />
Interpretation <strong>of</strong> diagnostic<br />
laboratory tests for severe<br />
acute respiratory syndrome:<br />
the Toronto experience.<br />
CMAJ 2004; 170(1): 47-54.<br />
4. Chan KH, Poon LL, Cheng<br />
VC, Guan Y, Hung IF, Kong J,<br />
Yam LY, Seto WH, Yuen KY<br />
and Peiris JS. Detection <strong>of</strong><br />
<strong>SARS</strong> <strong>coronavirus</strong> in patients<br />
with suspected <strong>SARS</strong>. Emerg<br />
Infect Dis 2004; 10(2): 294-9<br />
5. World Health Organisation. Use <strong>of</strong> laboratory methods for <strong>SARS</strong> <strong>diagnosis</strong>.<br />
www.who.int/csr/sars/labmethods/en<br />
6. Poon LL, Wong OK, Luk W, Yuen KY, Peiris JS and Guan Y. Rapid <strong>diagnosis</strong> <strong>of</strong> a<br />
<strong>coronavirus</strong> associated with severe acute respiratory syndrome (<strong>SARS</strong>). Clin Chem<br />
2003; 49: 953-5<br />
7. Rainer TH, Cameron PA, Smit D, Ong KL, Hung AN, Nin DC, et al. Evaluation <strong>of</strong><br />
WHO criteria for identifying patients with severe acute respiratory syndrome out <strong>of</strong><br />
hospital: prospective observational study. BMJ 2003; 326: 1354-8<br />
8. World Health Organisation. WHO collaborative multi-centre research project on<br />
Severe Acute Respiratory Syndrome (<strong>SARS</strong>) <strong>diagnosis</strong>. www.who.int/csr/sars/project/en<br />
9. World Health Organisation. WHO post-outbreak biosafety guidelines for handling<br />
<strong>of</strong> <strong>SARS</strong>-CoV specimens and cultures.<br />
www.who.int/csr/sars/biosafety2003_12_18/en<br />
The author<br />
Karen Sonnenberg, M Eng.<br />
EUROIMMUN AG<br />
Seekamp 31<br />
23560 Luebeck, Germany<br />
Phone: +49 451 5855 535<br />
Fax: +49 451 5855 591<br />
E-mail: k.sonnenberg@euroimmun.de<br />
Figure 4. Euroimmun IIFT: antibodies against <strong>SARS</strong>-<br />
CoV.
S ARS<br />
http://www.euroimmun.com<br />
CLI September 2004<br />
8