Kallmann Syndromes MR Findings - Neuroradiology
Kallmann Syndromes MR Findings - Neuroradiology
Kallmann Syndromes MR Findings - Neuroradiology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
l<br />
<strong>Kallmann</strong> <strong>Syndromes</strong> <strong>MR</strong> <strong>Findings</strong><br />
John R. Knorr,r Ronald L. Ragland,t Rosalind S. Brown,2 and Nicholas Gelberl<br />
PORPOSE: To evaluate patients with known hypogonadotropic hypogonadism, some with known<br />
anosmia, for defective rhlnocephalon development that resulted in olfactory tract abnormalities,<br />
an affliction known as <strong>Kallmann</strong> syndrome. METHODS: Six patients who clinically had hypogonadotropic<br />
hypogonadism were examined by <strong>MR</strong>. Thin coronal images of the interior frontal region<br />
were used to determine presence or absence of olfactory tract and to evaluate the olfactory sulci.<br />
RESOLTS: Olfactory tracts were not seen in three of the six cases; two of which had hypoplastic<br />
olfactory sulci. CONCL0SIONS: Tl-weighted <strong>MR</strong> examination of the lnferior frontal region in the<br />
coronal plane can help determine whether a patient with hypogonadotropic hypogonadism, with<br />
or without clinically evident anosmia, is afflicted with <strong>Kallmann</strong> syndrome.<br />
Index terms: <strong>Kallmann</strong> syndrome; Nervous system, disease; Olfactory lobe; Brain, magnetic<br />
resonance; Brain, growth and development<br />
AJNR 14:845-851, Jul/Aug 1993<br />
Kallman syndrome is a form of congenital<br />
hypogonadotropic hypogonadism with accompanying<br />
hyposomia or anosmia (1). lts reported<br />
incidence is on the order of 1 in 10,000 men and<br />
1 in 50,000 women (2). This disease is believed<br />
to be due to defective rhinocephalon development,<br />
which results in hypoplasia or absence of<br />
olfactory tract development (3). We used magnetic<br />
resonance (<strong>MR</strong>) imaging to visualize the<br />
olfactory tracts and to evaluate the olfactory sulci<br />
in patients with this abnormality.<br />
Materials and Methods<br />
We examined six patients who appeared clinically to<br />
have hypogonadotropic hypogonadism and anosmia, and<br />
had a family history of <strong>Kallmann</strong> syndrome. The standard<br />
examination included sagittal Tl-weighted and axial double-echo<br />
T2-weighted images (for example, conventional<br />
spin-echo ICSEI 400/11 (repetition time/echo time) and<br />
2500/30 and 80, respectively). However, an additional<br />
sequence was performed on each patient to evaluate the<br />
Received Aug. 12, 1992; revision requested Sept. 17; final revision<br />
received Jan. 19, 1993 and accepted Jan.26.<br />
Departments of Radiologyt and Pediatric Endocrinology,2 (Jniversity<br />
of /rlassachusetts lledical Center, Worcester, lvlA 01655.<br />
Address reprint requests to: John R. Knorr, D.O., Department of<br />
Radiology, University of Massachusetts Mdical Center, 55 Lake Avenue<br />
North, Worcester, MA 01655<br />
AJNR 1 4:845-85 l, July/Aus I 993 0 I 95-6 I 08 /93 / 1 404-0845<br />
@ American Society of <strong>Neuroradiology</strong><br />
845<br />
olfactory sulcus region further and to determine the presence<br />
of the olfactory tract. Three-millimeter section thickness<br />
with Tl-weighted technique (for example CSE 800/<br />
12) images were obtained through the frontal lobe region<br />
(see Fig. 1). Scans were performed on a 1.5-T system. The<br />
images were evaluated by two neuropdiologists for the<br />
appearance of the olfactory sulci as well as visualization of<br />
the olfactory tracts (see Fig. 1). The coronal plane was<br />
chosen for evaluation because the structures of interest are<br />
well seen in this plane, and volume averaging, even with<br />
3-mm section thickness, could not obscure them. As the<br />
authors were unaware of a standard of depth for the<br />
olfactory sulci, olfactory sqlcus depth was compared with<br />
that of other sulci visualized in the same patient.<br />
Results<br />
The clinical and radiologic findings are displayed<br />
in Table 1.<br />
Case 1<br />
The patient presented at age 16 years with<br />
short stature and delayed puberty. He was the<br />
product of a difficult delivery and clinically had<br />
severe neonatal asphyxia. He also had severe<br />
hydrops and hyperbilirubinemia, presumed to be<br />
due to Rh incompatibility, requiring three exchange<br />
transfusions. As a child, he had delayed<br />
milestones, such as not walking or talking until 2<br />
years of age, although it was not immediately<br />
clear whether this was related to his neonatal<br />
illnesses.
846<br />
KNORR<br />
AJNR: 14, JuIy/August 1993<br />
',Li' ;'<br />
,.;ti::;.:: '<br />
" ..1.<br />
rL q'r:<br />
i;<br />
iil<br />
.J<br />
AB<br />
Hrnt'ez<br />
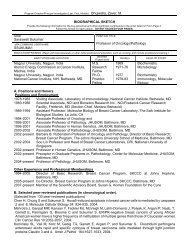
Fig. 1. A, Anatomic drawing of external view of the inferior frontal region.<br />
8, Anatomic drawing of coronal section.<br />
C, Normal coronal T1-weighted (SE 800/12) <strong>MR</strong> image.<br />
The left olfactory bulb has been retracted in the drawing (A, small arrow). The<br />
olfactory tract (large arrow) is seen on each image. The medial olfactory stria (curved<br />
arrowl and lateral olfactory stria (/ong arrow\ are seen in A.<br />
On presentation, his height was below the fifth<br />
percentile, and weight was between the tenth and<br />
twenty-fifth percentiles. His penis was small, and<br />
his scrotum undervirilized. He remained cryptorchid,<br />
although small testes (5 mm) were thought<br />
palpable in the inguinal canals. He was unable to<br />
perceive the odor of peppermint or lemon oil.<br />
The patient was placed on monthly testosterone<br />
and synthetic thyroid hormone therapy and<br />
achieved full puberty after 4 years.<br />
An <strong>MR</strong> examination of the brain was tailored<br />
to the inferior frontal lobes (Fig. 2). Hypoplastic<br />
and small olfactory sulci were noted. The olfactory<br />
tracts and bulbs were not seen. The pituitary<br />
gland was normal.<br />
Case 2<br />
The patient presented at 18 years of age with<br />
short stature and delayed puberty. His family<br />
history was notable for a maternal grandmother<br />
who had anosmia, which she thought due to<br />
chronic "sore throat." A maternal great uncle<br />
never developed puberty and had no children.<br />
A maternal aunt had a son with retardation, hypogonadism,<br />
anosmia, and an undefined renal<br />
affliction. Another maternal aunt bore a son<br />
with cryptorchism, hypogonadism, and mental<br />
retardation.<br />
The patient's height and weight were below<br />
the fifth percentile for his age. His penis was
AJNR: 14, July/August 1993<br />
The olfactory sulcus lateral to the gyrus rectus<br />
of the brain was absent unilaterally in one patient<br />
(Fig. 2) with <strong>Kallmann</strong> syndrome and bilaterally<br />
(Fig. 3) in the other patient. In the seven volunteers,<br />
the gyrus rectus-olfactory sulcus regions<br />
were readily identifiable and well formed.<br />
Quantitative analysis of the temporal lobes of<br />
the patients with <strong>Kallmann</strong> syndrome demonstrated<br />
no significant difference in the temporal<br />
lobe volume (228 + 5.6 cc) compared with that<br />
in the healthy patients (233.47 + 36.5 cc). These<br />
findings were duplicated in the hippocampal volumes<br />
(27.0 + 0.9 cc vs 29.27 t 4.0 cc).<br />
Intraobserver error for defining temporal lobe<br />
volumes was 3Vo in one observer and 45% in<br />
the second reviewer, For the olfactory bulbs and<br />
tracts, the intraobserver variability was 10% and<br />
KALLMANN SYNDROME 841<br />
23% for the two reviewers. Interobserver variance<br />
was3Vo for temporallobe volumes, butwas3}Vo<br />
for olfactory bulbs and tracts. This is not unexpected<br />
with such small volumed structures as the<br />
bulbs and tracts.<br />
No signal intensity abnormalities were visualized<br />
in the temporal lobes or hippocampi in the<br />
<strong>Kallmann</strong> syndrome patients.<br />
Discussion<br />
<strong>Kallmann</strong> described a familial occunence of<br />
patients who failed to reach sexual maturity and<br />
had a lack of the sense of smell (1). Testicular<br />
biopsies have subsequently shown an arrest of<br />
spermatogenesis with fibrotic infiltration (5). The<br />
patients are completely anosmic by olfactory<br />
Fig.2. A-D, Patient with <strong>Kallmann</strong> syndrome demonstrates absence of the olfactory bulbs and tracts with a flattened gyrus rectus<br />
1Oy and no olfactory sulcus on the right side, but a normal-appearing gyrus rectus on the left side. (Figures proceed from anterior to<br />
Posterior from A to 4 5OO/14.)
842 YOOSEM<br />
14, July/August<br />
Fig. 3. A-C, Second patient with <strong>Kallmann</strong> syndrome demonstrates<br />
aplasia of the olfactory bulbs and tracts bilaterally on<br />
these short repetition time images. The olfactory sulcus is not<br />
well formed. Motion artifact limits image quality. (Figures proceed<br />
from anterior to posterior from A to C;500/14.\<br />
testing, but have normal intranasal examinations.<br />
Short fourth metacarpal bones have also been<br />
reported in <strong>Kallmann</strong> syndrome (5). Histopathologically,<br />
the pituitary glands are reported to be<br />
normal although the hypothalamus may be hypoplastic<br />
(4).<br />
The present study demonstrates the utility of<br />
high-resolution surface-coil <strong>MR</strong> in evaluating patients<br />
with congenital anosmia. <strong>MR</strong> showed aplasia<br />
of the olfactory bulbs and tracts in both cases<br />
of <strong>Kallmann</strong> syndrome and showed normal olfactory<br />
structutes in control volunteers. The olfactory<br />
nerve can be readily studied with <strong>MR</strong> and<br />
can yield a complete analysis of the anatomy<br />
governing olfaction.<br />
Klingmuller et al evaluated the olfactory sulci<br />
on axial <strong>MR</strong> images of the brain in four patients<br />
with <strong>Kallmann</strong> syndrome (B). They found that<br />
there was absence or hypoplasia of the olfactory<br />
sulci of the frontal lobes, as seen on axial <strong>MR</strong>.<br />
However, they did not evaluate the patients' olfactory<br />
bulbs or tracts, possibly because of the<br />
low spatial resolution of the <strong>MR</strong> scanner. A surface<br />
coil was not employed to visualize the olfactory<br />
bulbs and tracts.<br />
Suzuki et al were the first to describe the<br />
visualization of the olfactory bulbs and tracts on<br />
<strong>MR</strong> scans (3). They found that with 256 x 256<br />
matrix scanning, visualization of the olfactory<br />
bulb was possible in 70 of 80 instances (87.5%).<br />
However with 256 X 128 matrix scanning, only<br />
34 of 50 (68%) olfactory bulbs were visualized.<br />
The authors recommended coronalscanning with<br />
large matrix size and decreased intersection gap<br />
to visualize the olfactory bulbs optimally. The<br />
authors suggested that this protocol could be<br />
used to evaluate patients with <strong>Kallmann</strong> syndrome.<br />
The olfactory system and the first cranialnerve<br />
have received little attention in the radiologic<br />
literature. Schellinger et al described their experience<br />
with computed tomography in evaluating<br />
patients with smell and taste disorders (9). They<br />
found that encephalomalacic change in the low<br />
frontal/gyrus rectus region and the temporal<br />
lobes was the most common finding in patients<br />
with olfactory deficits. These changes were most<br />
common in patients with posttraumatic (53% of<br />
patients) hyposmia. The yield by computed to-
AJNR: 1,4, July/August 1993<br />
KALLMANN SYNDROME 843<br />
mography in patients with congenital causes was<br />
very low.<br />
The olfactory nerve has been largely ignored<br />
in imaging literature despite the association of<br />
numerous neurologic diseases with smell dysfunction,<br />
including Alzheimer disease, Parkinson<br />
disease, schizophrenia, Huntington chorea, and<br />
Korsakoff syndrome (10). Although there are a<br />
number of causes of anosmia, including posttraumatic,<br />
postinflammatory, degenerative disorders,<br />
neoplasms (olfactory groove meningiomas, olfactory<br />
neuroblastomas), and congenital etiologies<br />
(11), total aplasia of the olfactory bulbs and tracts<br />
is typically associated with <strong>Kallmann</strong> syndrome.<br />
There are other congenital disorders associated<br />
with decreased olfaction (12, 13), including holoprosencephaly,<br />
Down syndrome, Turner syndrome,<br />
and Riley-Day syndrome; however, complete<br />
absence of the olfactory bulbs and tracts<br />
has been well-documented only in <strong>Kallmann</strong> syndrome.<br />
These lists of disease entities associated<br />
with smell dysfunction are only partial; as smell<br />
and taste testing has become more widespread,<br />
the prevalence of lesions associated with hyposmia<br />
has increased. Smell is one of the least<br />
studied senses.<br />
Pathologically, absence of the olfactory bulbs<br />
and tracts has been described with <strong>Kallmann</strong><br />
syndrome; however, there may be a variable<br />
degree of rudimentary olfactory apParatus Present<br />
(4, 5). Since the olfactory system projects<br />
fibers to the amygdala and hippocampus, we<br />
analyzed the temporal lobe for volumetric<br />
changes. Theoretically, without stimuli from the<br />
olfactory apparatus peripherally, hypoplasia of<br />
the hippocamPus or temporal lobes might be<br />
expected. In fact, we found this not to be true,<br />
although a larger sample size may be needed to<br />
establish this point definitively. The hippocampi<br />
and temporal lobe volumes were analogous to<br />
those of control Patients.<br />
With a surface coil placed over the bridge of<br />
the nose and contiguous thin sections with large<br />
matrix sizes, the olfactory bulbs and tracts should<br />
always be seen in healthy patients. The absence<br />
thereof in association with congenital anosmia<br />
and hypothalamic hypogonadism supports the<br />
diagnosis of <strong>Kallmann</strong> syndrome.<br />
References<br />
1. <strong>Kallmann</strong> FT, Schoenfeld WA, Barrera SE. The genetic asPects of<br />
primary eunuchoidism. Am J Mental Deficits 1944;48:2O3-208<br />
2. Meitinger T, Heye B, Petit C, et al. Definitive localization of X-linked<br />
<strong>Kallmann</strong> syndrome to Xp22.3: close linkage to the hypervariable<br />
repeat sequence CRI-S232. Am J Hum Genet 199O;47:664-669<br />
3. Suzuki M, Takashima T, Kadoya lv\, Takahashi S, Miyayama S, Taira<br />
S. <strong>MR</strong> imaging of olfactory bulbs and tracts. AJNR: Am J Neurorcdiol<br />
1989;10:955-957<br />
4. De Morsier Q, Gauthier C. Ln dysplasie olfacto-genitale. Bathol Biol<br />
1963;11:7267-7272<br />
5. Males JL, Townsend JL, Schneider RA' Hypogonadotrophic hypogonadism<br />
with anosmia-<strong>Kallmann</strong>'s syndrome. Arch Intern lvled<br />
'1973:137:507-507<br />
6. Doty RL, Shaman P, Dann M. Development of the University of<br />
Pennsylvania Smell ldentification Test: a standardized microencapsulated<br />
test of olfactory function (monogr). Physiol Behav<br />
1984:32:489-5O2<br />
7. Raya SP, Udupa JK, Warrett WA. A PC-based #D imaging system:<br />
algorithms, software, and hardware considerations. Comp l4ed Imaging<br />
Qrc Ph i c s 1990 ; 74 :353-37 O<br />
8. Klingmuller D, Dewes W, Krahe T, Brecht C' Schweikert H0. Magnetic<br />
resonance imaging of the brain in Patients with anosmia and hypothalamic<br />
hypogonadism (<strong>Kallmann</strong>'s syndrome). J Clin Endocrinol<br />
hleta b 7987 i65 :587 -584<br />
9. Schellinger D, Henkin RT, Smirniotopoulos JG. CT of the brain in<br />
taste and smell dysfunction. AJNR: Am J Neurorcdiol 1983;4:752'<br />
t)4<br />
10. Doty RL. Olfactory dysfunction in neurodegenerative disorders' In:<br />
Cetchell TV, Doty RL, Bartoshuk LM, Snow JB, eds. Smell and taste<br />
in heatth and disease. New Yorkr Raven, 1991:35-751<br />
11. Deems DA, Doty RL, Settle RG, et al. Smell and taste disorders; a<br />
study of 750 patients from the University of Pennsylvania Smell and<br />
Taste Center. Arch Otolaryngot Head Neck Surg 1991;717:5't9-528<br />
12. Warner MD, Peabody CA, Berger PA. Olfactory deficits and Down's<br />
syndrome. Biol Psychiatry 1988;23:833-836<br />
13. Probst FP. The prosencephalies' Berlin: Springer-Verlag, 7979:46
AJNR: 14, July/August 1993<br />
KALLMANN SYNDROME 851<br />
in normal patients, visualization of the olfactory<br />
tracts. Hypoplasia of the olfactory sulci or nonvisualization<br />
of the olfactory tracts along with the<br />
clinical findings of hypogonadotropic hypogonadism,<br />
anosmia, or heredity (family history of <strong>Kallmann</strong><br />
syndrome) is consistent with the presence<br />
of <strong>Kallmann</strong> syndrome.<br />
Acknowledgments<br />
Anatomic illustrations by Laura Perry, MD. Special<br />
thanks for manuscript preparation to Kathy Delongchamp.<br />
References<br />
1. Kaltmann FJ, Schoenfeld WA, Barrera SE' The genetic asPects of<br />
primary eunuchoidism. Am J l4ent Defic 7944;48:203-270<br />
2. Jones JR, Kemmann E. Olfacto-genitaldysplasia in the female. Obstet<br />
G yn ecol An n 797 6 ;5 :443-445<br />
3. Maestre de San Juan A. Teratologia: falta total de los nervios<br />
olfactorios con anosmian en un individuo en quien existia un atrofia<br />
congentia de los testiculos y miembro v.ril. EI Siglo /4ed 1856;3:211-<br />
zzl<br />
4. lvloorman JR, Crain B, Osborne D. <strong>Kallmann</strong>'s syndrome with associated<br />
cardiovascular and intracranial abnormalities. Am J /vled<br />
'1984:77:369-372<br />
5. Kovacs K, Sheehan HL. Pituitary changes in <strong>Kallmann</strong>'s syndrome: a<br />
histologic immunocytologic, ultrastructural and immunoelectron microscopic<br />
study. Fertil Steril 1982;37:83-89<br />
6. Bardin CW, Ross GT, Rifkind AB, Cargille CM, LiPsette MB. Studies<br />
of the pituitary-leydig cell assessing young men with hypogonadotropic<br />
hypogonadism and hyposmia. Comparison wlth normal men,<br />
prepuberal boys and hypopituitary parents. J Clin Invest<br />
1969:48:2O46<br />
7. Lieblich JM, Rogol AD, White BJ, Rosen SW. Syndrome of anosmia<br />
with hypogonadotroPic hypogonadism in (<strong>Kallmann</strong>s syndrome).<br />
Clinicaf and laboratory studies in 23 cases. Am J Med '1982;73:<br />
506-519<br />
8. Turner RC, Bobrow M, Bobrow LG, et al. Cryptorchidism in a family<br />
member with <strong>Kallmann</strong>'s syndrome. Proc R Soc Ned'1974;67:33-35<br />
9. Rogol AD, et al. HLA compatible paternity in two "fertile eunuchs"<br />
with congenital hypogonadotropic hypogonadism and anosmia (the<br />
<strong>Kallmann</strong>'s syndrome). J Clin Endocrinol Neab 1980;38:275<br />
10. Klingsmuller D, Dewes W, Krahe Th, Brecht G, Shweikert H. Alagnetic<br />
resonance imaging of the brain in Patient's with anosmia and hypothalamic<br />
hypogonadism (<strong>Kallmann</strong>'s syndrome). J Clin Endoctinol<br />
fie tab 1987 :62:58.1 -584<br />
11. lvlalat J, Virapongse C. Brain calcification in <strong>Kallmann</strong>'s syndrome.<br />
Computed tomograPhic appearance. Pediatr Neurosci'1985-<br />
1986:72:257-259<br />
12. Von Dewes W, Krahe Th, Klingmuller D, Harder Th. <strong>MR</strong> tomographie<br />
beim Kallman syndrom. Fortschr Rontgenstr 7987 :147 :4OA-442<br />
13. Williams PL, Warwick R (eds). Aray's anatomy.36th ed. Philadelphia:<br />
WB Saunders, 1986:994-995