IRS Form 990-PF for 2009 - Blue Shield of California Foundation
IRS Form 990-PF for 2009 - Blue Shield of California Foundation
IRS Form 990-PF for 2009 - Blue Shield of California Foundation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
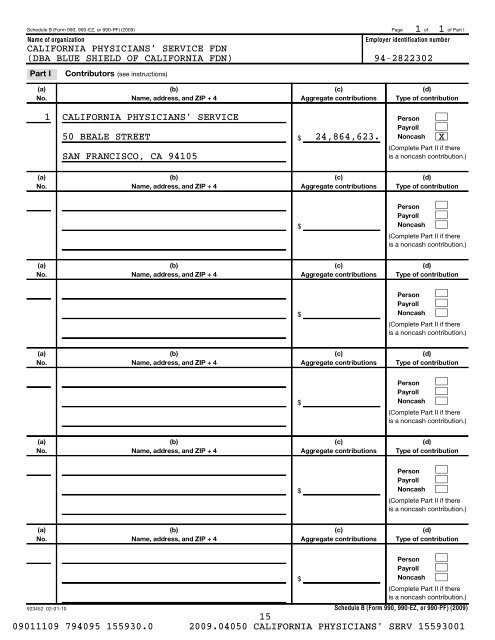
Schedule B (<strong>Form</strong> <strong>990</strong>, <strong>990</strong>-EZ, or <strong>990</strong>-<strong>PF</strong>) (<strong>2009</strong>) Page <strong>of</strong> <strong>of</strong> Part I<br />
Name <strong>of</strong> organization<br />
Employer identification number<br />
CALIFORNIA PHYSICIANS' SERVICE FDN<br />
(DBA BLUE SHIELD OF CALIFORNIA FDN) 94-2822302<br />
1 1<br />
Part I<br />
Contributors<br />
(see instructions)<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
1 CALIFORNIA PHYSICIANS' SERVICE<br />
Person<br />
Payroll <br />
Noncash <br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
50 BEALE STREET 24,864,623. X<br />
SAN FRANCISCO, CA 94105<br />
$<br />
<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
$<br />
Person<br />
Payroll<br />
Noncash<br />
<br />
<br />
<br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
$<br />
Person<br />
Payroll<br />
Noncash<br />
<br />
<br />
<br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
$<br />
Person<br />
Payroll<br />
Noncash<br />
<br />
<br />
<br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
$<br />
Person<br />
Payroll<br />
Noncash<br />
<br />
<br />
<br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
(a)<br />
No.<br />
(b)<br />
Name, address, and ZIP + 4<br />
(c)<br />
Aggregate contributions<br />
(d)<br />
Type <strong>of</strong> contribution<br />
923452 02-01-10<br />
$<br />
Person<br />
Payroll<br />
Noncash<br />
<br />
<br />
<br />
(Complete Part II if there<br />
is a noncash contribution.)<br />
Schedule B (<strong>Form</strong> <strong>990</strong>, <strong>990</strong>-EZ, or <strong>990</strong>-<strong>PF</strong>) (<strong>2009</strong>)<br />
15<br />
09011109 794095 155930.0 <strong>2009</strong>.04050 CALIFORNIA PHYSICIANS' SERV 15593001