Guidelines for Specimen Collection, Storage and Transport for OPS ...
Guidelines for Specimen Collection, Storage and Transport for OPS ...
Guidelines for Specimen Collection, Storage and Transport for OPS ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Department of Health<br />
Research Institute <strong>for</strong> Tropical Medicine<br />
National Reference Laboratories <strong>for</strong> Emerging Infectious Diseases<br />
Filinvest Corporate City, Alabang, Muntinlupa City 1781<br />
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING<br />
FOR CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY<br />
NOVEL RESPIRATORY PATHOGENS<br />
Version 3 | 2 July 2013<br />
1. BACKGROUND<br />
Several novel respiratory pathogens (NRPs) have recently emerged <strong>and</strong> have continued<br />
to pose global public health threats with their potential to cause outbreaks or p<strong>and</strong>emics of<br />
severe acute respiratory infections:<br />
<br />
<br />
<br />
Avian Influenza A (H5N1) Virus. Since the occurrence of large epizootics of the<br />
avian Influenza A (H5N1) virus in Southeast Asia in 2004 <strong>and</strong> 2005, the virus<br />
continued to spread among avian populations geographically [1]. In the past year,<br />
the World Health Organization (WHO) reported sporadic human cases of H5N1 in<br />
Cambodia, Vietnam, Indonesia, Egypt <strong>and</strong> Bangladesh. [2]. Recent sporadic human<br />
cases in Egypt, Bangladesh, Cambodia, Vietnam <strong>and</strong> China indicate that<br />
appearance of other cases are expected <strong>and</strong> will likely occur in the future [3].<br />
Middle East Respiratory Syndrome Coronavirus (MERS-CoV). On September<br />
2012, the United Kingdom Health Protection Agency (UK HPA) in<strong>for</strong>med the WHO of<br />
a novel Coronavirus from a patient with acute respiratory syndrome, with travel<br />
history to Saudi Arabia <strong>and</strong> Qatar. The virus is similar to an earlier (July 2012) isolate<br />
from a fatal case in Saudi Arabia [4]. To date, WHO reports of laboratory-confirmed<br />
cases originating in the following countries: Jordan, Qatar, Saudi Arabia, <strong>and</strong> the<br />
United Arab Emirates. Furthermore, WHO encourages “all Member States to<br />
continue their surveillance <strong>for</strong> severe acute respiratory infections <strong>and</strong> to carefully<br />
review any unusual patterns” [5].<br />
Avian Influenza A (H7N2) Virus. WHO has been reporting cases of human infection<br />
with Avian Influenza A H7N9 viruses, with the source of infection <strong>and</strong> the mode of<br />
transmission currently unknown [6]. As of 29 May 2013, WHO has been in<strong>for</strong>med of<br />
a total of 132 laboratory-confirmed cases, including 37 deaths. It is expected that<br />
there will be further cases of human infection until the source of infection has been<br />
identified <strong>and</strong> controlled [7].
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
Laboratory confirmation is needed to classify a patient as a confirmed case of any of these<br />
NRPs <strong>and</strong> initiate clinical <strong>and</strong> epidemiological investigations. The Research Institute <strong>for</strong><br />
Tropical Medicine (RITM), the National Reference Laboratory <strong>for</strong> Emerging <strong>and</strong> Reemerging<br />
Infections, per<strong>for</strong>ms WHO-recommended methods of molecular detection by<br />
polymerase chain reaction (PCR) in the rapid detection of these NRPs. Furthermore, there<br />
may be other potential primary etiologies of community-acquired pneumonia aside from<br />
NRPs like Streptococcus pneumoniae, Hemophilus influenza type B, Legionella<br />
pneumophila, other recognized primary bacterial pneumonias, influenza, <strong>and</strong> respiratory<br />
syncytial virus. Testing <strong>for</strong> these other microorganisms is needed to identify the etiologic<br />
agent from a patient presenting with community-acquired pneumonia. RITM will be testing<br />
<strong>for</strong> specific <strong>and</strong> differential diagnosis <strong>for</strong> these NRPs, as indicated by the attending<br />
physician in the laboratory request.<br />
This document provides the interim guidelines <strong>for</strong> sample collection, storage <strong>and</strong> transport<br />
<strong>and</strong> laboratory testing <strong>for</strong> specific detection <strong>and</strong> differential diagnosis of NRPs. This<br />
document supersedes earlier <strong>and</strong> similar versions of guidelines release by RITM.<br />
2. SAMPLE TYPES FOR COLLECTION<br />
2.1. For patients falling under the DOH Case Definition <strong>for</strong> Case Under Observation<br />
(CUO) <strong>for</strong> the NRP being investigated, collect the following priority specimens <strong>for</strong> the<br />
specific detection of the NRP <strong>and</strong> <strong>for</strong> differential diagnosis of other possible causative<br />
agents:<br />
<br />
For MERS-CoV:<br />
Priority specimens: Lower respiratory specimens such as sputum,<br />
endotracheal aspirate, broncheoalveolar lavage or pleural fluid collected within<br />
14 days after the onset of symptoms.<br />
<br />
Alternative specimens: Nasopharyngeal swab AND oropharyngeal swab<br />
combined in Virus <strong>Transport</strong> Medium 1 (VTM), if patients do not have signs <strong>and</strong><br />
symptoms of lower respiratory tract infection <strong>and</strong> lower tract specimens are not<br />
possible or clinically indicated.<br />
1 VTM collection kits are available by request from the RITM Clinical Laboratory,<br />
Telephone Nos. (02) 8422442 or (02) 8072628 to 32 local 201. Refer to Section 7<br />
of this document <strong>for</strong> the prices.<br />
Page 2 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
<br />
For MERS-CoV (continued):<br />
The WHO recommends that “[i]f initial testing of a nasopharyngeal swab is<br />
negative in a patient who is strongly suspected to have MERS-CoV infection,<br />
patients should be retested using a lower respiratory specimen or a repeat<br />
nasopharyngeal specimen with additional oropharyngeal specimen if lower<br />
respiratory specimens are not possible” [8]. RITM may <strong>for</strong> request additional<br />
specimens depending on initial testing results.<br />
<br />
For Novel Influenza Viruses A(H5N1) <strong>and</strong> A(H7N9):<br />
<br />
Oropharyngeal swab (<strong>OPS</strong>) AND Nasopharyngeal swab (NPS) combined in<br />
Virus <strong>Transport</strong> Medium 1 (VTM) <strong>and</strong> collected within 14 days after the onset of<br />
symptoms<br />
2.2. Other specimens which may be tested <strong>for</strong> the molecular detection of the NRPs <strong>and</strong> <strong>for</strong><br />
differential diagnosis are as follows:<br />
<br />
<br />
<br />
<br />
Fresh tissue samples (e.g., lung tissues), collected as clinically indicated<br />
Serum sample, collected within seven days after the onset of symptoms<br />
Blood sample in BHI broth <strong>for</strong> patients with signs <strong>and</strong> symptoms of septicemia<br />
Nasopharyngeal swab (NPS) in Atypical Pneumonia <strong>Transport</strong> Medium 1 (APTM),<br />
collected within 14 days after the onset of symptoms, <strong>for</strong> detection of causative<br />
agents of atypical pneumonia<br />
2.3. Refer to the document on the RITM Website <strong>for</strong> the laboratory investigation by electron<br />
microscopy <strong>and</strong> histopathology.<br />
2.4. Other specimen types may be collected as indicated by the attending physician.<br />
1 VTM/APTM collection kits are available by request from the RITM Clinical Laboratory,<br />
Telephone Nos. (02) 8422442 or (02) 8072628 to 32 local 201. Refer to Section 7 of<br />
this document <strong>for</strong> the prices.<br />
Page 3 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
3. BIOSAFETY GUIDELINES DURING SAMPLE COLLECTION<br />
During the collection of specimens from patients suspected with any of the NRPs, isolate<br />
patient to minimise contact/exposure to staff <strong>and</strong> other patients. Wear personal protective<br />
equipment – correctly-fitted N95 respirator, gown, gloves <strong>and</strong> eye protection.<br />
Good Laboratory Practices <strong>and</strong> st<strong>and</strong>ard precautions <strong>for</strong> Biosafety Level 2 laboratories must<br />
be strictly observed in h<strong>and</strong>ling specimens suspected of containing NRPs. Refer to the<br />
following document (WHO Laboratory Biosafety <strong>Guidelines</strong> <strong>for</strong> H<strong>and</strong>ling <strong>Specimen</strong>s<br />
Suspected of Containing Avian Influenza A Virus) <strong>for</strong> more in<strong>for</strong>mation:<br />
http://www.who.int/influenza/resources/documents/guidelines_h<strong>and</strong>ling_specimens/en/.<br />
Furthermore, laboratories are advised to avoid per<strong>for</strong>ming the following procedures with<br />
samples from suspected cases. Per<strong>for</strong>mance of these procedures could put the<br />
laboratory staff at risk <strong>for</strong> laboratory-acquired infections. These procedures may only be<br />
per<strong>for</strong>med at RITM, using Biosafety Level 3 practices.<br />
<br />
<br />
<br />
<br />
aliquoting <strong>and</strong>/or diluting specimens<br />
per<strong>for</strong>ming diagnostic testing that involves propagation of viral agents in vitro or in<br />
vivo<br />
per<strong>for</strong>ming nucleic acid extractions that involve untreated specimens<br />
preparing smears using heat or chemical fixation<br />
4. GUIDELINES FOR SPECIMEN COLLECTION<br />
Effective <strong>and</strong> accurate diagnosis is highly dependent on the timing of specimen collection,<br />
appropriate clinical sample, <strong>and</strong> the condition during transport to the laboratory. Refer to the<br />
instructions below <strong>for</strong> specimen collection.<br />
4.1. General <strong>Guidelines</strong><br />
Label each specimen container with the Patient’s Name, Age <strong>and</strong> Sex, <strong>Specimen</strong> Type<br />
<strong>and</strong> Date of <strong>Specimen</strong> <strong>Collection</strong>. The label should remain attached to the specimen<br />
container under all conditions of storage <strong>and</strong> transport. The in<strong>for</strong>mation on the label<br />
Page 4 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
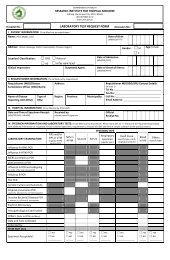
must be legible <strong>and</strong> should match the in<strong>for</strong>mation on the RITM Laboratory Test<br />
Request Form, downloadable from the RITM website. Please fill out all the indicated<br />
fields in the <strong>for</strong>m. Failure to do so could result in delays in the processing of the<br />
specimen.<br />
After collection, transport the specimens immediately to RITM. Refer to Section 5 of this<br />
document <strong>for</strong> proper transport of specimens. If delays between collection <strong>and</strong> transport<br />
are expected, refrigerate specimen at 4°C <strong>and</strong> ship within 48 hours of collection.<br />
4.2. Sputum<br />
Have the patient rinse the mouth with water. Let the patient expectorate deep cough<br />
sputum directly into a sterile screw-capped sputum collection cup or a sterile dry<br />
container.<br />
4.3. Broncheoalveolar lavage, tracheal aspirate, pleural fluid <strong>and</strong> nasal aspirate<br />
Collect 2 - 3 mL into a leak-proof, screw-capped sputum collection cup or sterile dry<br />
container.<br />
4.4. Nasopharyngeal <strong>and</strong> oropharyngeal swabs<br />
Refer to the document: <strong>Guidelines</strong> <strong>for</strong> <strong>Specimen</strong> <strong>Collection</strong>, <strong>Storage</strong> <strong>and</strong> <strong>Transport</strong><br />
<strong>for</strong> <strong>OPS</strong> <strong>and</strong> NPS in the RITM website:<br />
www.ritm.gov.ph/Announcements/<strong>Guidelines</strong>%20<strong>for</strong>%20<strong>Specimen</strong>%20<strong>Collection</strong>,%20S<br />
torage%20<strong>and</strong>%20<strong>Transport</strong>%20<strong>for</strong>%20<strong>OPS</strong>%20<strong>and</strong>%20NPS.pdf<br />
Collect nasopharyngeal swabs <strong>for</strong> VTM <strong>and</strong> APTM media separately.<br />
4.5. Serum<br />
Collect 5mL to 10mL of whole blood in a serum separator tube. After clotting, centrifuge<br />
the tube <strong>and</strong> collect the resulting serum in polypropylene, external screw-capped vials<br />
with internal O-ring seals. If the vial has no internal O-ring seal, seal the vial tightly with<br />
the available cap <strong>and</strong> seal with Parafilm to prevent leakage. RITM requires a<br />
minimum amount of 500µL serum <strong>for</strong> testing <strong>and</strong> banking.<br />
Page 5 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
5. SPECIMEN STORAGE AND TRANSPORT<br />
The sending laboratory is responsible <strong>for</strong> the proper packaging of the specimens <strong>and</strong> in<br />
assuring that the specimen reaches RITM in good condition.<br />
5.1. For NPS <strong>and</strong> <strong>OPS</strong> samples: Wrap the specimen tubes in tissue paper or any<br />
absorbent material; place upright in a separate 50 mL centrifuge tube or any<br />
leak/puncture proof container. Place the 50 mL tube in a resealable plastic bag (e.g.,<br />
Ziplock). The materials needed are provided in the VTM or APTM collection kit<br />
available from RITM (See Section 2.1 above).<br />
5.2. For serum, sputum <strong>and</strong> other samples: Use screw-capped, polypropylene tubes or<br />
containers <strong>for</strong> transport. Do not transport the samples in glass containers. Individually<br />
place each sample container in a resealable plastic bag (e.g., Ziplock).<br />
5.3. Place all the specimen containers except BHI in a shipment/carrier box with at least four<br />
(4) frozen ice packs inside to maintain prescribed temperature. Put the frozen ice packs<br />
in first, at the bottom <strong>and</strong> at the sides of the carrier box; then place specimens at the<br />
middle so that they are surrounded by the ice packs. Cover the carrier box.<br />
5.4. BHI samples must be stored <strong>and</strong> transported in room temperature. Do not include BHI<br />
samples inside the box with samples to be transported in cold chain.<br />
5.5. Place the completely filled-up RITM Laboratory Test Request Form in a separate ziplocked<br />
plastic bag <strong>and</strong> put on top of the box <strong>and</strong> secure with tape.<br />
5.6. Notify RITM be<strong>for</strong>e sending the specimen. RITM receives samples 24 hours a day,<br />
seven days a week.<br />
5.7. Send to the Research Institute <strong>for</strong> Tropical Medicine (RITM) using the following contact<br />
in<strong>for</strong>mation:<br />
RESEARCH INSTITUTE FOR TROPICAL MEDICINE<br />
CLINICAL LABORATORY<br />
Filinvest Corporate City, Alabang<br />
Muntinlupa City 1781<br />
Telephone Numbers: (02) 842 2442<br />
(02) 807 2628 to 32 local 201<br />
Page 6 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
5.8. If delays between collection <strong>and</strong> transport are expected, refrigerate specimen at 4°C<br />
<strong>and</strong> ship within 48 hours of collection.<br />
5.9. All polystyrene foam (“styrofoam”) boxes used <strong>for</strong> specimen transport will be<br />
decontaminated <strong>and</strong> disposed of by RITM as infectious waste.<br />
Page 7 of 12
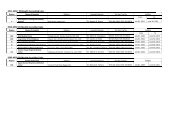
6. LABORATORY TESTING AT RITM<br />
Available Tests as of 2 July 2013<br />
Samples referred as Case Under Observation (CUO) by the National Epidemiology Center are FREE of testing charges.<br />
Samples referred by other institutions will be charged by RITM with the indicated testing fees. Testing fees indicated in this<br />
section supersede the testing fees <strong>for</strong> similar tests indicated in earlier documents released by RITM.<br />
Tests Available<br />
<strong>Specimen</strong><br />
Type<br />
Appropriate <strong>Collection</strong><br />
Time; Days After Onset<br />
of Symptoms<br />
Turnaround<br />
Time<br />
Testing Fees<br />
Specific detection of NRPs<br />
Influenza A screening <strong>and</strong> subtyping <strong>for</strong> Novel<br />
Influenza viruses by PCR<br />
- Avian Influenza H5N1<br />
- Avian Influenza H7N9<br />
NPS <strong>and</strong> <strong>OPS</strong><br />
in VTM<br />
other respiratory<br />
samples<br />
within 14 days<br />
within 7 days<br />
4 working days<br />
single subtype:<br />
PhP 4,000.00<br />
package:<br />
PhP 5,000.00<br />
MERS-CoV detection by PCR Refer to Section 2.1 within 14 days 4 working days PhP 5,000.00
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
Tests Available<br />
<strong>Specimen</strong><br />
Type<br />
Appropriate <strong>Collection</strong><br />
Time; Days After Onset<br />
of Symptoms<br />
Turnaround<br />
Time<br />
Testing Fees<br />
Differential diagnosis<br />
Influenza A screening <strong>and</strong> subtyping <strong>for</strong><br />
currently circulating Influenza viruses by PCR<br />
- Seasonal Influenza H1N1<br />
- Seasonal Influenza H3N2<br />
- P<strong>and</strong>emic Influenza 2009 H1N1<br />
NPS <strong>and</strong>/or <strong>OPS</strong><br />
in VTM<br />
other respiratory<br />
samples<br />
within 14 days<br />
within 7 days<br />
4 working days<br />
screening <strong>and</strong><br />
subtyping<br />
package:<br />
PhP 6,000.00<br />
Influenza B PCR detection<br />
NPS <strong>and</strong>/or <strong>OPS</strong><br />
in VTM<br />
other respiratory<br />
samples<br />
within 14 days<br />
within 7 days<br />
4 working days PhP 4,000.00<br />
Respiratory Syncytial Virus PCR detection<br />
NPS <strong>and</strong>/or <strong>OPS</strong><br />
in VTM<br />
other respiratory<br />
samples<br />
within 14 days<br />
within 7 days<br />
4 working days PhP 5,000.00<br />
panCoronavirus detection by PCR<br />
(Detects all human Coronaviruses)<br />
NPS <strong>and</strong> <strong>OPS</strong> in<br />
VTM<br />
other respiratory<br />
samples<br />
within 14 days<br />
within 7 days<br />
4 working days PhP 5,000.00<br />
Page 9 of 12
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
Tests Available<br />
<strong>Specimen</strong><br />
Type<br />
Appropriate <strong>Collection</strong><br />
Time; Days After Onset<br />
of Symptoms<br />
Turnaround<br />
Time<br />
Testing Fees<br />
Atypical pneumonia PCR panel<br />
(Mycoplasma, Legionella <strong>and</strong> Chlamydia)<br />
NPS in APTM<br />
as clinically indicated,<br />
be<strong>for</strong>e antibiotic<br />
treatment<br />
4 working days<br />
single pathogen:<br />
PhP 3,500.00<br />
package:<br />
PhP 5,000.00<br />
Invasive bacterial diseases PCR panel<br />
(H. influenzae, S. pneumonia, N. meningitidis)<br />
serum<br />
as clinically indicated,<br />
be<strong>for</strong>e antibiotic<br />
treatment<br />
4 working days<br />
single pathogen:<br />
PhP 3,500.00<br />
package:<br />
PhP 5,000.00<br />
Aerobic culture<br />
sputum <strong>and</strong>/or<br />
blood in BHI<br />
as clinically indicated,<br />
be<strong>for</strong>e antibiotic<br />
treatment<br />
4 working days PhP 1,274.00<br />
Electron microscopy<br />
Histopathological examination<br />
fresh tissues<br />
<strong>and</strong> secretions<br />
fresh tissues<br />
<strong>and</strong> secretions<br />
as clinically indicated Please refer to a separate<br />
document in the RITM website<br />
<strong>for</strong> specimen collection, cost <strong>and</strong><br />
turn-around time <strong>for</strong> electron<br />
as clinically indicated microscopy <strong>and</strong> histopathology<br />
diagnostics.<br />
Page 10 of 12
7. COLLECTION KITS<br />
VTM <strong>and</strong> APTM collection kits are available by request from the RITM Clinical Laboratory,<br />
Telephone Nos. (02) 8422442 or (02) 8072628 to 32 local 201. Cost of the kits are indicated<br />
below.<br />
<strong>Collection</strong> Kit<br />
VTM <strong>Collection</strong> kit (contains VTM tube, <strong>OPS</strong>, NPS, tongue<br />
depressor, ziplock bag, absorbent material <strong>and</strong> 50mL tube as<br />
secondary container)<br />
Cost<br />
P 300.00<br />
APTM <strong>Collection</strong> kit (contains APTM tube, NPS, , ziplock bag,<br />
absorbent material <strong>and</strong> 50mL tube as secondary container)<br />
P 250.00<br />
8. FOLLOW-UP OF RESULTS<br />
Testing results may be followed-up after the indicated turnaround time at this number: (02)<br />
425 8910. RITM will be releasing additional contact in<strong>for</strong>mation as soon as these are<br />
available.<br />
Results will be faxed to the official fax number of the referring institution or emailed as a pdf<br />
copy to the official email address of the referring institution, as indicated in the RITM<br />
Laboratory Test Request Form. Alternately, results may be picked-up at RITM-DOH.<br />
As an institutional policy, RITM does not release Official Results by phone.<br />
9. REFERENCES<br />
[1] The Writing Committee of the World Health Organization (WHO) Consultation on Human Influenza<br />
A/H5, "Avian Influenza A (H5N1) Infection in Humans," The New Engl<strong>and</strong> Journal of Medicine, vol.<br />
353, pp. 1374-1385, 2005.<br />
[2] World Health Organization, "Situation Updates - Avian influenza," 2013. [Online]. Available:<br />
http://www.who.int/influenza/human_animal_interface/avian_influenza/archive/en/index.html.<br />
[Accessed 22 April 2013].<br />
[3] World Heath Organization, "Influenza at the human-animal interface: Summary <strong>and</strong> assessment as<br />
of 4 June 2013," 4 June 2013. [Online]. Available:
GUIDELINES FOR SPECIMEN COLLECTION AND LABORATORY TESTING FOR<br />
CASE FINDING AND INVESTIGATION OF HUMAN INFECTION CAUSED BY NOVEL RESPIRATORY PATHOGENS<br />
http://www.who.int/influenza/human_animal_interface/Influenza_Summary_IRA_HA_interface_04Ju<br />
n13.pdf. [Accessed 2 July 2013].<br />
[4] United Kingdom Health Protection Agency, "Questions <strong>and</strong> Answers - novel coronavirus September<br />
2012," 24 September 2012. [Online]. Available:<br />
http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/RespiratoryViruses/NovelCoronavirus<br />
/respq<strong>and</strong>anovelcoronavirusspet2012/. [Accessed 27 September 2012].<br />
[5] World Health Organization - Global Alert <strong>and</strong> Response, "Middle East respiratory syndrome<br />
coronavirus (MERS-CoV) - update," 26 June 2013. [Online]. Available:<br />
http://www.who.int/csr/don/2013_06_26/en/index.html. [Accessed 2 July 2013].<br />
[6] World Health Organization, "Background <strong>and</strong> Summary of Human Infection with Influenza A(H7N9)<br />
Virus– As of 5 April 2013," [Online]. Available:<br />
http://www.who.int/influenza/human_animal_interface/latest_update_h7n9/en/index.html. [Accessed<br />
22 April 2013].<br />
[7] World Health Organization - Global Alert <strong>and</strong> Response, "Human Infection with Avian Influenza<br />
A(H7N9) Virus in China - 19 April 2013 Update," [Online]. Available:<br />
http://www.who.int/csr/don/2013_04_19/en/index.html. [Accessed 22 April 2013].<br />
[8] World Health Organization, "Novel coronavirus infection - update," 25 September 2012. [Online].<br />
Available: http://www.who.int/csr/don/2012_09_25/en/index.html. [Accessed 27 September 2012].<br />
[9] United Kingdom Health Protection Agency, "Infection Control Advice - Suspected or Confirmed<br />
Novel Coronavirus Cases," 26 September 2012. [Online]. Available:<br />
http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317136232722. [Accessed 27 September<br />
2012].<br />
[10] World Health Organization, "Revised interim case definition – novel coronavirus," 29 September<br />
2012. [Online]. Available:<br />
http://www.who.int/csr/disease/coronavirus_infections/case_definition/en/index.html. [Accessed 3<br />
October 2012].<br />
[11] World Health Organization, "Novel coronavirus infection - update," 25 September 2012. [Online].<br />
Available: http://www.who.int/csr/don/2012_09_25/en/index.html. [Accessed 27 September 2012].<br />
[12] World Health Organization - Global Alert <strong>and</strong> Response, "Middle East respiratory syndrome<br />
coronavirus (MERS-CoV)," 26 June 2013. [Online]. Available:<br />
http://www.who.int/csr/don/2013_06_26/en/index.html. [Accessed 2 July 2013].<br />
Page 12 of 12