APPLICATION FORM FOR ACCREDITATION - 2011 (pdf)
APPLICATION FORM FOR ACCREDITATION - 2011 (pdf)
APPLICATION FORM FOR ACCREDITATION - 2011 (pdf)
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
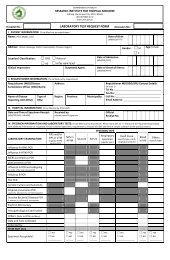
Part I. Laboratory Information:Republic of the PhilippinesDepartment of HealthPhilippine Health Insurance CorporationandResearch Institute for Tropical MedicineAntimicrobial Resistance Surveillance Program<strong>APPLICATION</strong> <strong>FOR</strong> <strong>ACCREDITATION</strong> OF AEROBIC BACTERIOLOGY LABORATORY(To be accomplished by Pathologist)Date of application: ___________ New [ ] Renewal [ ]MM/DD/YYName of Institution/Laboratory: ______________________________________________________Category of Lab -Classification of laboratory by level:Classification of laboratory by ownership:Health Facility: ___ Government: ___District : ___ Private : ___Provincial : ___ Number of cultures performed per year: ___Regional : ___National : ___Address :___________ ________________________ ____________________________________No. Street Barangay______________________________ ___________ _______________ _______Municipality/City Province Region Zip codeTelephone No: __________________________ Facsimile No: __________________Area code + Phone #BHFS License Permit No: _________________ Validity Date: __________________MM/DD/YYPart II. Organization Data:A. Name of Hospital Director: _____________________ _____________________ ___Surname First Name M.I.B. Head of Laboratory: _____________________ ________________________ ___Surname First Name M.I.Address :___________ ________________________ _________________________No. Street Barangay______________________________________ _______________ _______Municipality/City Province Zip codeTelephone No :__________________________ Facsimile No: __________________Area code + Phone #PRC License No :__________________________ Validity Date: __________________MM/DD/YYDate of certification by the Philippine Society of Pathology: _______________MM/DD/YYName of specialty board: [ ] AP, [ ] CP, [ ] AP-CP,[ ] others (specify) ______________1
C. StaffingLaboratory Staff Name Position Title1. Clinical Microbiologist2. Hospital Epidemiologist3. Technical Consultant4. Bacteriology Supervisor5. Medical Technologist6. Laboratory Assistant/Technician7. Laboratory Aide8. ClerkNote: Please use separate sheet if necessary.Part III: Service CapabilitiesEducationalAttainmentPRC No/ValidityTEST1. Gram’s Staining2. Culture (Isolationand Identification)3. SusceptibilityTesting4. Others, (specify)() ifdoneSend-outName of Laboratory Address TelephonePart IV. FeesInitial accreditation and renewal fee: (Non-refundable) P 1500.00EQAS fee (Non-refundable) 5,500.00Mode of Payment: Cash: (ARSP-RITM Cashier) ________________AmountCheck: (Payable to Research Institute for Tropical Medicine)________________Check Number________________Amount________________Bank/ Branch________________DateIf you do not receive an acknowledgement receipt within 3 weeks after submission of application form, pleasecall ARSRL office at 02 8099763.2
Part V: DeclarationI hereby certify that the foregoing statements are true. I hereby submit this application for accreditation underARSP and agree to comply with the rules and regulations of PHILHEALTH CIRCULAR No. 15, s- 2006._________________________________Name in Print and Signature_________________________________Designation_________________________________PTR_________________________________Date3
Republic of the Philippines)Manila) S.S.Before me at Manila this ___ day of ___________, came and appeared the following and exhibited hisCommunity Tax Certificate as shown above known to me and to me known to be the same persons whoexecuted the foregoing Application for Accreditation of Aerobic Bacteriology Laboratory and acknowledgedthe same as their voluntary act and lawful deed.CTX No. __________________ issued at _________________on ___________________________This document consisting of four (4) pages, including this on which the acknowledgement is writtenhas been signed by the parties and their witnesses on each and every page thereof and pertains to anapplication for accreditation.WITNESS MY HAND AND SEALDoc. No. ___Page __Book No. __Series of _____ATTY. _________________________________Notary PublicUntil ________________IBP No. ______________4