with Instructions on Filling out the Laboratory Request Form
with Instructions on Filling out the Laboratory Request Form
with Instructions on Filling out the Laboratory Request Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
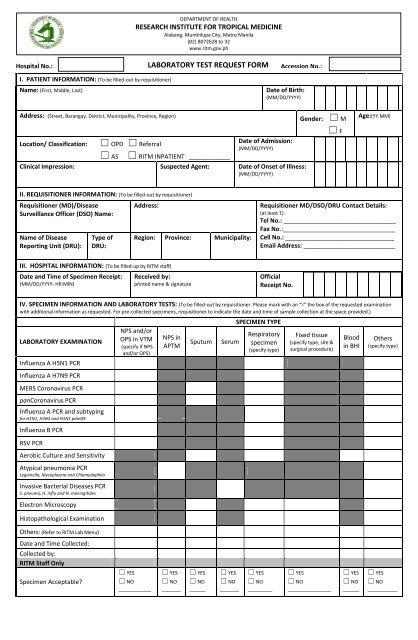
DEPARTMENT OF HEALTHRESEARCH INSTITUTE FOR TROPICAL MEDICINEAlabang, Muntinlupa City, Metro Manila(02) 8072628 to 32www.ritm.gov.phHospital WWW No.:LABORATORY TEST REQUEST FORMAccessi<strong>on</strong> No.:I. PATIENT INFORMATION: (To be filled-<strong>out</strong> by requisiti<strong>on</strong>er)Name: (First, Middle, Last)WWW.RITM.GOV.PHDate of Birth:(MM/DD/YYYY)Address: (Street, Barangay. District, Municipality, Province, Regi<strong>on</strong>)☐ OPD ☐ ReferralLocati<strong>on</strong>/ Classificati<strong>on</strong>:Date of Admissi<strong>on</strong>:(MM/DD/YYYY)☐ AS ☐ RITM INPATIENT ____________Clinical Impressi<strong>on</strong>: Suspected Agent: Date of Onset of Illness:(MM/DD/YYYY)Gender: ☐ M☐ FAge:(YY.MM)II. REQUISITIONER INFORMATION: (To be filled-<strong>out</strong> by requisiti<strong>on</strong>er)Requisiti<strong>on</strong>er (MD)/DiseaseSurveillance Officer (DSO) Name:Name of DiseaseReporting Unit (DRU):Type ofDRU:Address:Regi<strong>on</strong>: Province: Municipality:Requisiti<strong>on</strong>er MD/DSO/DRU C<strong>on</strong>tact Details:(at least 1)Tel No.: _________________________________Fax No.:_________________________________Cell No.: ________________________________Email Address: ___________________________III. HOSPITAL INFORMATION: (To be filled-up by RITM staff)Date and Time of Specimen Receipt:(MM/DD/YYYY- HR:MIN)Received by:printed name & signatureOfficialReceipt No.IV. SPECIMEN INFORMATION AND LABORATORY TESTS: (To be filled-<strong>out</strong> by requisiti<strong>on</strong>er. Please mark <str<strong>on</strong>g>with</str<strong>on</strong>g> an “X” <strong>the</strong> box of <strong>the</strong> requested examinati<strong>on</strong><str<strong>on</strong>g>with</str<strong>on</strong>g> additi<strong>on</strong>al informati<strong>on</strong> as requested. For pre-collected specimens, requisiti<strong>on</strong>er to indicate <strong>the</strong> date and time of sample collecti<strong>on</strong> at <strong>the</strong> space provided.)LABORATORY EXAMINATIONInfluenza A H5N1 PCRInfluenza A H7N9 PCRMERS Cor<strong>on</strong>avirus PCRpanCor<strong>on</strong>avirus PCRInfluenza A PCR and subtypingfor H1N1, H3N2 and H1N1 pdm09Influenza B PCRRSV PCRAerobic Culture and SensitivityAtypical pneum<strong>on</strong>ia PCRLegi<strong>on</strong>ella, Mycoplasma and ChlamydophilaInvasive Bacterial Diseases PCRS. pneumo, H. influ and N. meningitidesElectr<strong>on</strong> MicroscopyHistopathological Examinati<strong>on</strong>NPS and/orOPS in VTM(specify if NPSand/or OPS)NPS inAPTMSputumSerumSPECIMEN TYPERespiratoryspecimen(specify type)Fixed tissue(specify type, site &surgical procedure)Bloodin BHIO<strong>the</strong>rs(specify type)O<strong>the</strong>rs: (Refer to RITM Lab Menu)Date and Time Collected:Collected by:RITM Staff OnlySpecimen Acceptable?☐ YES☐ NO____________☐ YES☐ NO_______☐ YES☐ NO______☐ YES☐ NO_______☐ YES☐ NO_________☐ YES☐ NO________________☐ YES☐ NO______☐ YES☐ NO___________
DEPARTMENT OF HEALTHRESEARCH INSTITUTE FOR TROPICAL MEDICINEAlabang, Muntinlupa City, Metro Manila(02) 8072628 to 32www.ritm.gov.phWWWIMPORTANT INSTRUCTIONS ON FILLING OUT THE LABORATORY TEST REQUEST FORMWWW.RITM.GOV.PHThe highlighted fields in <strong>the</strong> sample <strong>Laboratory</strong> Test <strong>Request</strong> <strong>Form</strong> below are <strong>the</strong> MINIMUM REQUIREDINFORMATION to be filled <strong>out</strong>. Failure to provide <strong>the</strong>se minimum required informati<strong>on</strong> may result inspecimen rejecti<strong>on</strong> and delay in specimen processing.Informati<strong>on</strong> to be filled <strong>out</strong> by RITMStaff. Please leave <strong>the</strong>se fields blank.At least <strong>on</strong>e c<strong>on</strong>tact informati<strong>on</strong>required for specimen to bec<strong>on</strong>sidered as acceptable at RITM.Informati<strong>on</strong> in this secti<strong>on</strong> to befilled <strong>out</strong> by RITM Staff. Please leave<strong>the</strong>se fields blank.Fill <strong>out</strong> <strong>the</strong> specimen types matrix asshown in this sample form. Mark<str<strong>on</strong>g>with</str<strong>on</strong>g> “X” for collected specimens and<strong>the</strong> requested informati<strong>on</strong>; leaveblank if no specimen was collected.Specify if NPS <strong>on</strong>ly, OPS <strong>on</strong>ly or acombinati<strong>on</strong> of NPS and OPS.Specify site and procedure for fixedtissues.Indicate date and time of collecti<strong>on</strong>and name of staff collecting <strong>the</strong>specimen.