Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...
Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...
Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Amrita</strong> <strong>Journal</strong> <strong>of</strong> <strong>Medicine</strong><br />
proximal motor neuropathy <strong>and</strong> metabolic bone disease.<br />
Going a step further, the temporal pr<strong>of</strong>ile <strong>of</strong> the illness,<br />
absence <strong>of</strong> fluctuating weakness/ wasting/<br />
fasciculations/ normal reflexes, narrow down the possibility<br />
to a muscle disease. Prior records from various<br />
hospitals showed that electrodiagnostic studies, serum<br />
CPK <strong>and</strong> muscle biopsy were all normal. She had also<br />
received steroids, but showed no response, thereby<br />
favouring the possibility <strong>of</strong> a metabolic myopathy rather<br />
than an inflammatory one.<br />
FUEL FOR THOUGHT<br />
She was investigated at various hospitals <strong>and</strong> found<br />
to have a raised alkaline phosphatase, normal calcium<br />
<strong>and</strong> low phosphorus, which was considered as secondary<br />
to hypovitaminosis D <strong>and</strong> hence she was put on Vit D<br />
<strong>and</strong> Calcium supplements without any improvement (she<br />
rather worsened).<br />
WHY NO RESPONSE AFTER 4 YEARS OF<br />
APPROPRIATE TREATMENT WITH<br />
VITAMIN D AND CALCIUM???<br />
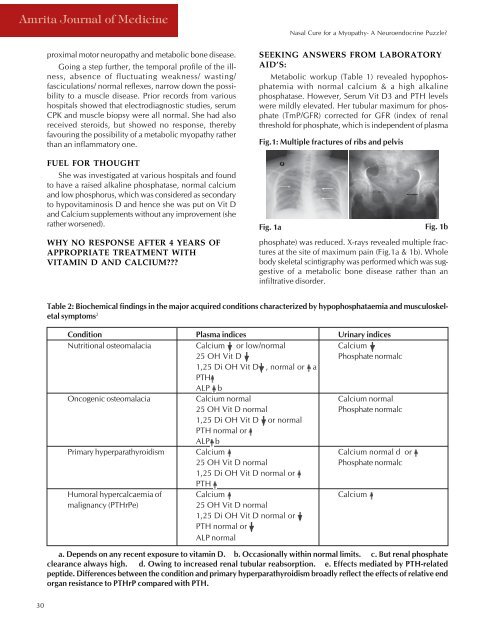
Fig.1: Multiple fractures <strong>of</strong> ribs <strong>and</strong> pelvis<br />
Fig. 1a<br />
Nasal Cure for a Myopathy- A Neuroendocrine Puzzle?<br />
SEEKING ANSWERS FROM LABORATORY<br />
AID’S:<br />
Metabolic workup (Table 1) revealed hypophosphatemia<br />
with normal calcium & a high alkaline<br />
phosphatase. However, Serum Vit D3 <strong>and</strong> PTH levels<br />
were mildly elevated. Her tubular maximum for phosphate<br />
(TmP/GFR) corrected for GFR (index <strong>of</strong> renal<br />
threshold for phosphate, which is independent <strong>of</strong> plasma<br />
Fig. 1b<br />
phosphate) was reduced. X-rays revealed multiple fractures<br />
at the site <strong>of</strong> maximum pain (Fig.1a & 1b). Whole<br />
body skeletal scintigraphy was performed which was suggestive<br />
<strong>of</strong> a metabolic bone disease rather than an<br />
infiltrative disorder.<br />
Table 2: Biochemical findings in the major acquired conditions characterized by hypophosphataemia <strong>and</strong> musculoskeletal<br />
symptoms 2<br />
Condition Plasma indices Urinary indices<br />
Nutritional osteomalacia Calcium or low/normal Calcium<br />
25 OH Vit D Phosphate normalc<br />
1,25 Di OH Vit D , normal or a<br />
PTH<br />
ALP b<br />
Oncogenic osteomalacia Calcium normal Calcium normal<br />
25 OH Vit D normal Phosphate normalc<br />
1,25 Di OH Vit D or normal<br />
PTH normal or<br />
ALP b<br />
Primary hyperparathyroidism Calcium Calcium normal d or<br />
25 OH Vit D normal Phosphate normalc<br />
1,25 Di OH Vit D normal or<br />
PTH<br />
Humoral hypercalcaemia <strong>of</strong> Calcium Calcium<br />
malignancy (PTHrPe)<br />
25 OH Vit D normal<br />
1,25 Di OH Vit D normal or<br />
PTH normal or<br />
ALP normal<br />
a. Depends on any recent exposure to vitamin D. b. Occasionally within normal limits. c. But renal phosphate<br />
clearance always high. d. Owing to increased renal tubular reabsorption. e. Effects mediated by PTH-related<br />
peptide. Differences between the condition <strong>and</strong> primary hyperparathyroidism broadly reflect the effects <strong>of</strong> relative end<br />
organ resistance to PTHrP compared with PTH.<br />
30