Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...
Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...
Journal of Medicine Vol 4 - Amrita Institute of Medical Sciences and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Amrita</strong> <strong>Journal</strong> <strong>of</strong> <strong>Medicine</strong><br />
CASE REPORT<br />
Rhinocerebral Mucormycosis in a<br />
Patient with Diabetic Nephropathy<br />
A. Mathew , J.C. Varghese, P. Nair *, V.N. Unni<br />
ABSTRACT<br />
Diabetes Mellitus <strong>and</strong> immunosuppressed states predispose patients to fungal infections like mucormycosis: We report<br />
a case <strong>of</strong> rhino cerebral mucormycosis in a patient with diabetic nephropathy <strong>and</strong> moderate renal failure.<br />
Key words : Rhinocerebral Mucormycosis, Diabetic Nephropathy<br />
INTRODUCTION<br />
Rhinocerebral mucormycosis is a<br />
life threatening infection that is associated<br />
with immunosuppressed states.<br />
The disease usually spreads rapidly;<br />
rarely, it may pursue an indolent<br />
course 1 . In diabetic subjects, it is characteristically<br />
associated with diabetic<br />
ketoacidosis. This case report describes<br />
fulminant <strong>and</strong> progressive rhinocerebral<br />
mucormycosis in a subject with<br />
diabetic nephropathy (without<br />
ketoacisosis). In addition to the case<br />
report, a brief discussion with the relevant<br />
review <strong>of</strong> the literature is also<br />
presented.<br />
CASE REPORT<br />
A 45 years old manual labourer, a<br />
known diabetic since 15 years <strong>and</strong><br />
hypertensive since six years, was admitted<br />
to our hospital with pain <strong>and</strong><br />
progressive swelling <strong>of</strong> the left side<br />
<strong>of</strong> the face since one week. He was<br />
found to have very high blood sugar<br />
levels <strong>and</strong> moderate renal failure, <strong>and</strong><br />
was referred to the Nephrologist for<br />
further treatment.<br />
Dept. <strong>of</strong> Nephrology, * Dept. <strong>of</strong> Otorhinolaryngology,<br />
AIMS, Kochi.<br />
On admission he was febrile, conscious<br />
<strong>and</strong> oriented. BP was 160/100<br />
mmHg. He had erythema <strong>and</strong> oedema<br />
over the left malar region <strong>of</strong> the face.<br />
Evaluation by ENT surgeon showed<br />
features <strong>of</strong> left maxillary sinusitis with<br />
sloughing <strong>of</strong> nasal mucosa. Optic<br />
fundi revealed non-proliferative diabetic<br />
retinopathy.<br />
Investigations showed neutrophilic<br />
leucocytosis (21,000/cu.mm) with<br />
shift to the left <strong>and</strong> prominent toxic<br />
granules in neutrophils. Blood sugars<br />
were uncontrolled (FBS: 523mg/dl,<br />
PPBS: 698 mg/dl); he had proteinuria<br />
(1800 mg in 24 hours) <strong>and</strong> a moderate<br />
renal failure (S.Creatinine: 3.3mg/<br />
dl). Ultrasonogram showed normal<br />
sized kidneys with increased<br />
echogenicity. Roentgenogram <strong>of</strong><br />
paranasal sinuses showed haziness <strong>of</strong><br />
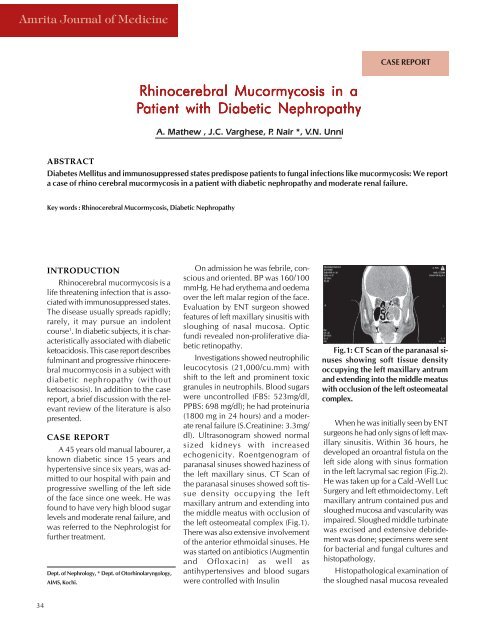
the left maxillary sinus. CT Scan <strong>of</strong><br />
the paranasal sinuses showed s<strong>of</strong>t tissue<br />
density occupying the left<br />
maxillary antrum <strong>and</strong> extending into<br />
the middle meatus with occlusion <strong>of</strong><br />
the left osteomeatal complex (Fig.1).<br />
There was also extensive involvement<br />
<strong>of</strong> the anterior ethmoidal sinuses. He<br />
was started on antibiotics (Augmentin<br />
<strong>and</strong> Ofloxacin) as well as<br />
antihypertensives <strong>and</strong> blood sugars<br />
were controlled with Insulin<br />
Fig.1: CT Scan <strong>of</strong> the paranasal sinuses<br />
showing s<strong>of</strong>t tissue density<br />
occupying the left maxillary antrum<br />
<strong>and</strong> extending into the middle meatus<br />
with occlusion <strong>of</strong> the left osteomeatal<br />
complex.<br />
When he was initially seen by ENT<br />
surgeons he had only signs <strong>of</strong> left maxillary<br />
sinusitis. Within 36 hours, he<br />
developed an oroantral fistula on the<br />
left side along with sinus formation<br />
in the left lacrymal sac region (Fig.2).<br />
He was taken up for a Cald -Well Luc<br />
Surgery <strong>and</strong> left ethmoidectomy. Left<br />
maxillary antrum contained pus <strong>and</strong><br />
sloughed mucosa <strong>and</strong> vascularity was<br />
impaired. Sloughed middle turbinate<br />
was excised <strong>and</strong> extensive debridement<br />
was done; specimens were sent<br />
for bacterial <strong>and</strong> fungal cultures <strong>and</strong><br />
histopathology.<br />
Histopathological examination <strong>of</strong><br />
the sloughed nasal mucosa revealed<br />
34