Child Life Council Twentieth Annual Conference On Professional ...
Child Life Council Twentieth Annual Conference On Professional ...
Child Life Council Twentieth Annual Conference On Professional ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
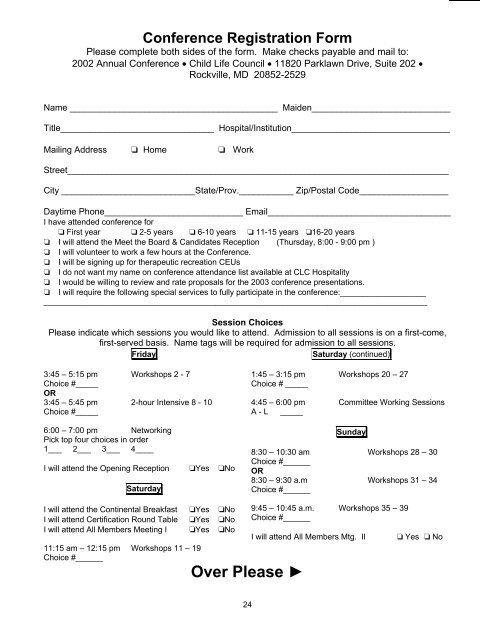
<strong>Conference</strong> Registration Form<br />
Please complete both sides of the form. Make checks payable and mail to:<br />
2002 <strong>Annual</strong> <strong>Conference</strong> • <strong>Child</strong> <strong>Life</strong> <strong>Council</strong> • 11820 Parklawn Drive, Suite 202 •<br />
Rockville, MD 20852-2529<br />
Name __________________________________________ Maiden____________________________<br />
Title_______________________________ Hospital/Institution________________________________<br />
Mailing Address ❏ Home ❏ Work<br />
Street_____________________________________________________________________________<br />
City ___________________________State/Prov.___________ Zip/Postal Code__________________<br />
Daytime Phone____________________________ Email_____________________________________<br />
I have attended conference for<br />
❏ First year ❏ 2-5 years ❏ 6-10 years ❏ 11-15 years ❏16-20 years<br />
❏ I will attend the Meet the Board & Candidates Reception (Thursday, 8:00 - 9:00 pm )<br />
❏ I will volunteer to work a few hours at the <strong>Conference</strong>.<br />
❏ I will be signing up for therapeutic recreation CEUs<br />
❏ I do not want my name on conference attendance list available at CLC Hospitality<br />
❏ I would be willing to review and rate proposals for the 2003 conference presentations.<br />
❏ I will require the following special services to fully participate in the conference:___________________<br />
_____________________________________________________________________________________<br />
Session Choices<br />
Please indicate which sessions you would like to attend. Admission to all sessions is on a first-come,<br />
first-served basis. Name tags will be required for admission to all sessions.<br />
Friday<br />
Saturday (continued)<br />
3:45 – 5:15 pm Workshops 2 - 7<br />
Choice #_____<br />
OR<br />
3:45 – 5:45 pm 2-hour Intensive 8 - 10<br />
Choice #_____<br />
6:00 – 7:00 pm Networking<br />
Pick top four choices in order<br />
1___ 2___ 3___ 4____<br />
I will attend the Opening Reception ❏Yes ❏No<br />
Saturday<br />
1:45 – 3:15 pm Workshops 20 – 27<br />
Choice # _____<br />
4:45 – 6:00 pm Committee Working Sessions<br />
A - L _____<br />
Sunday<br />
8:30 – 10:30 am Workshops 28 – 30<br />
Choice #______<br />
OR<br />
8:30 – 9:30 a.m Workshops 31 – 34<br />
Choice #______<br />
I will attend the Continental Breakfast ❏Yes ❏No<br />
I will attend Certification Round Table ❏Yes ❏No<br />
I will attend All Members Meeting I ❏Yes ❏No<br />
11:15 am – 12:15 pm Workshops 11 – 19<br />
Choice #______<br />
Over Please ►<br />
9:45 – 10:45 a.m. Workshops 35 – 39<br />
Choice #______<br />
I will attend All Members Mtg. II<br />
❏ Yes ❏ No<br />
24