Remicade (infliximab) - Immune Modulators
Remicade (infliximab) - Immune Modulators
Remicade (infliximab) - Immune Modulators

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
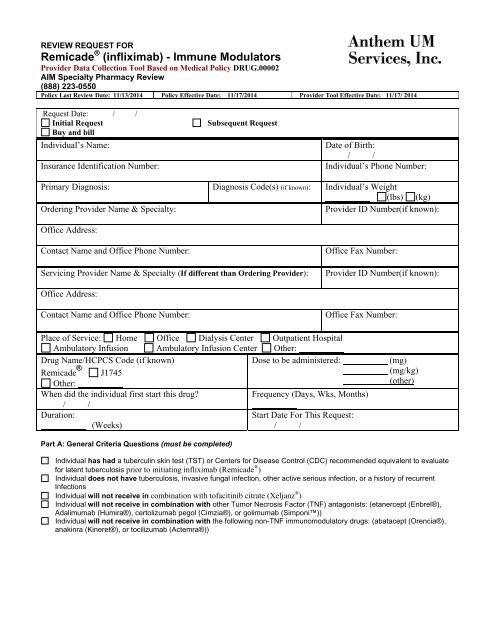
REVIEW REQUEST FOR<br />
<strong>Remicade</strong> ® (<strong>infliximab</strong>) - <strong>Immune</strong> <strong>Modulators</strong><br />
Provider Data Collection Tool Based on Medical Policy DRUG.00002<br />
AIM Specialty Pharmacy Review<br />
(888) 223-0550<br />
Policy Last Review Date: 11/13/2014 Policy Effective Date: 11/17/2014 Provider Tool Effective Date: 11/17/ 2014<br />
Request Date: / /<br />
Initial Request<br />
Buy and bill<br />
Individual’s Name:<br />
Insurance Identification Number:<br />
Subsequent Request<br />
Date of Birth:<br />
/ /<br />
Individual’s Phone Number:<br />
Primary Diagnosis: Diagnosis Code(s) (if known): Individual’s Weight<br />
(lbs) (kg)<br />
Ordering Provider Name & Specialty:<br />
Provider ID Number(if known):<br />
Office Address:<br />
Contact Name and Office Phone Number:<br />
Servicing Provider Name & Specialty (If different than Ordering Provider):<br />
Office Fax Number:<br />
Provider ID Number(if known):<br />
Office Address:<br />
Contact Name and Office Phone Number:<br />
Office Fax Number:<br />
Place of Service: Home Office Dialysis Center Outpatient Hospital<br />
Ambulatory Infusion Ambulatory Infusion Center Other:<br />
Drug Name/HCPCS Code (if known)<br />
Dose to be administered:<br />
<strong>Remicade</strong> ® J1745<br />
Other:<br />
When did the individual first start this drug?<br />
Frequency (Days, Wks, Months)<br />
/ /<br />
Duration:<br />
Start Date For This Request:<br />
(Weeks)<br />
/ /<br />
(mg)<br />
(mg/kg)<br />
(other)<br />
Part A: General Criteria Questions (must be completed)<br />
Individual has had a tuberculin skin test (TST) or Centers for Disease Control (CDC) recommended equivalent to evaluate<br />
for latent tuberculosis prior to initiating <strong>infliximab</strong> (<strong>Remicade</strong> ® )<br />
Individual does not have tuberculosis, invasive fungal infection, other active serious infection, or a history of recurrent<br />
Infections<br />
Individual will not receive in combination with tofacitinib citrate (Xeljanz ® )<br />
Individual will not receive in combination with other Tumor Necrosis Factor (TNF) antagonists: (etanercept (Enbrel®),<br />
Adalimumab (Humira®), certolizumab pegol (Cimzia®), or golimumab (Simponi))<br />
Individual will not receive in combination with the following non-TNF immunomodulatory drugs: (abatacept (Orencia®),<br />
anakinra (Kineret®), or tocilizumab (Actemra®))
Part B: (Only complete the section for appropriate diagnosis)<br />
(1) Rheumatoid Arthritis (RA)<br />
Individual is age 18 years or older and is diagnosed with moderate to severe active RA<br />
Agent is being used to reduce signs or symptoms<br />
Agent is being used to induce or maintain clinical response<br />
Agent is being used to inhibit the progression of structural damage<br />
Agent is being used to improve physical function<br />
Infliximab will be given in combination with methotrexate<br />
Individual is intolerant of methotrexate and will be given in combination with another<br />
immunosuppressive agent<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to one or more nonbiologic<br />
disease-modifying antirheumatic drugs (DMARDs) [methotrexate, sulfasalazine (Azulfidine®),<br />
hydroxychloroquine (Plaquenil®), Leflunomide (Arava®) or other immunosuppressants]<br />
Please list treatments tried:<br />
Other:<br />
(2) Plaque Psoriasis (Ps)<br />
Individual is age 18 years or older and is diagnosed with chronic moderate to severe (that is, extensive or<br />
disabling) plaque psoriasis<br />
Plaque psoriasis involves greater than 5% of the body surface area (BSA) Plaque psoriasis involves<br />
less than or equal to 5% of the body surface area (BSA) presenting with plague psoriasis involving<br />
sensitive areas or areas that would significantly impact daily function (such as palms, soles of feet,<br />
head/neck, or genitalia)<br />
Agent is being used to reduce signs or symptoms<br />
Agent is being used to induce or maintain clinical response<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to phototherapy or<br />
other systemic therapies [acitretin, cyclosporine, methotrexate]<br />
Please list treatments tried:<br />
Other:<br />
(3) Psoriatic Arthritis (PsA)<br />
Individual age 18 years or older and is diagnosed with active psoriatic arthritis<br />
Agent is being used to reduce signs or symptoms<br />
Agent is being used to induce or maintain clinical response<br />
Agent is being used to inhibit the progression of structural damage<br />
Agent is being used to improve physical function<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to conventional therapy<br />
[nonbiologic DMARDs: methotrexate, sulfasalazine (Azulfidine®), hydroxychloroquine (Plaquenil®),<br />
corticosteroids (such as hydrocortisone, prednisone) or other immunosuppressants]<br />
Please list treatments tried:<br />
Other:<br />
(4) Ankylosing Spondylitis (AS)<br />
Individual is age 18 years or older and has active ankylosing spondylitis<br />
Agent is being used to reduce signs or symptoms of the disease<br />
Individual failed to respond to, is intolerant of, or has medical contraindication to conventional therapies [such as<br />
nonsteroidal anti-inflammatory drugs NSAIDS (such as Ibuprofen, Motrin®) or nonbiologic DMARDS<br />
[methotrexate, sulfasalazine (Azulfidine®), hydroxychloroquine (Plaquenil®), corticosteroids (such as<br />
hydrocortisone, prednisone) or other immunosuppressants]<br />
Please list treatments tried:<br />
Other:
(5) Crohn’s Disease (CD)<br />
Individual is age 6 years of age or older<br />
Individiual is diagnosed with fistulizing or moderate to severe active Crohn’s Disease which has responded to<br />
previous therapy with <strong>infliximab</strong> (<strong>Remicade</strong>)<br />
Agent is being used to reduce the number of draining enterocutaneous or rectovaginal fistulas in an<br />
individual with fistulizing CD of at least 3 months duration<br />
Agent is being used to reduce sign or symptoms in an individual with moderately to severely active CD<br />
Agent is being used to induce or maintain clinical remission in an individual with moderately to<br />
severely active CD<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to conventioinal<br />
therapy (such as 5-Aminosalicylic acid [5-ASA] products, sulfasalazine, systemic corticosteroids,<br />
or immunosuppressive drugs)<br />
Please list treatment(s) tried:<br />
Other:<br />
(6) Ulcerative Colitis (UC)<br />
Individual is age 6 years or older and is diagnosed with moderately to severely active Ulcerative Colitis<br />
Agent is being used to reduce signs or symptoms<br />
Agent is being used to induce or maintain clinical remission and mucosal healing<br />
Individual has failed to respond to, is intolerant of, or has medical contraindication to conventional<br />
therapies [5-ASA products (e.g. Pentasa®, Rowasa®), sulfasalazine (Azulfidine®),<br />
systemic corticosteroids (i.e. hydrocortisone, prednisone), other immunosuppressive drugs<br />
Please list treatment(s) tried:<br />
Other:<br />
(7) Juvenile Idiopathic Arthritis (JIA)<br />
Individual is 2 years of age or older and has moderately to severely active JIA<br />
Agent is being used to reduce signs or symptoms<br />
Agent is being used to induce or maintain clinical response<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to one or more nonbiologic<br />
DMARDs: methotrexate, sulfasalazine (Azulfidine®), hydroxychloroquine (Plaquenil®), or corticosteroids (for<br />
example hydrocortisone, prednisone) or other immunosuppressants.<br />
Please list nonbiologic DMARDs tried:<br />
Other:<br />
(8) Non-infectious Uveitis<br />
Individual has chronic, recurrent, treatment-refractory disease<br />
Individual has vision-threatening disease<br />
Individual has a medical contraindication to conventional therapy (such as corticosteroids or immunosuppressive<br />
drugs [for example, azathioprine, cyclosporine, or methotrexate]).<br />
Individual has failed to respond to, is intolerant of, or has a medical contraindication to conventional therapy<br />
(such as corticosteroids, azathioprine, cyclosporine, methotrexate or other immunosuppressants).<br />
Please list treatments tried:<br />
Other:<br />
(9) Other indications not otherwise specified above (Please submit all supporting documents including labs, progress notes,<br />
imaging, etc., for review.)<br />
This request is being submitted:<br />
Pre-Claim<br />
Post–Claim. If checked, please attach the claim or indicate the claim number<br />
I attest the information provided is true and accurate to the best of my knowledge. I understand that the health plan or its<br />
designees may perform a routine audit and request the medical documentation to verify the accuracy of the information<br />
reported on this form.
Name & Title of Provider or Provider Representative Completing Form<br />
Date<br />
& attestation (Please Print)*<br />
*The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted<br />
Anthem UM Services, Inc., a separate company, is the licensed utilization review agent that performs utilization<br />
management services on behalf of your health benefit plan or the administrator of your health benefit plan.