Sight and Life Magazine 1/2011
Sight and Life Magazine 1/2011
Sight and Life Magazine 1/2011

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
VOL. 25 (1) | <strong>2011</strong><strong>Sight</strong> <strong>and</strong> <strong>Life</strong>16 THE IMPORTANCE OF VITAMIN A30 THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNS38 FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREA44 IRON FORTIFICATION – NEW REVELATIONS?
Contents06 Editorial10 <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Statement67 New Developments in Carotenoids ResearchConference at Tufts University, Boston, USA,11–12 March <strong>2011</strong>13 The “<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> in My <strong>Life</strong>” Essay CompetitionField Reports14 Special Feature: Food prices on the rise again16 The Importance of Vitamin A for the Development<strong>and</strong> Function of Lungs in Newborns30 Testing the Feasibility of Delivering Vitamin Ato Newborns in Nepal <strong>and</strong> Bangladesh38 Diversification from Agriculture to Nutritionally<strong>and</strong> Environmentally Promotive Horticulture ina Dry-L<strong>and</strong> Area44 Iron Fortification – New Revelations?55 Opinion 1: Comments on “Iron Fortification –New Revelations?”56 Opinion 2: Venturing into the Jungle of MultipleInteractions between Iron, Modulating Influences,<strong>and</strong> Human Health72 Report from GogounouBlessings at the I-Domarou Health Center74 Report from Kathm<strong>and</strong>uA Project Report on Training of Adolescent Girlsfor Prevention <strong>and</strong> Control of Iron Deficiency Anemia2009/1077 Report from LembaCentre de Lutte Contre la Malnutrition de Lemba78 Report from RatanakkiriSchool Health Watch80 News96 Letter to the Editor98 Publications103 Imprint58 <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Interview A Day in the <strong>Life</strong> ofJohann C JerlingCongress Reports62 Fourth Africa Nutritional Epidemiology Conference(ANEC 4) Nutrition <strong>and</strong> Food Security: Successes<strong>and</strong> Emerging Challenges64 Report from the First Global Conferenceon Biofortification
⇢
4“Our work is more vital todaythan ever before”
6What is abr<strong>and</strong> ?It would be impossible to imagine the modern world withoutbr<strong>and</strong>s. From airlines to computers, from fruit drinks to clothes,from football teams to hair shampoo, our choices are informedby br<strong>and</strong>s. There are many definitions of the word ‘br<strong>and</strong>’.David Ogilvy, famous advertising copywriter <strong>and</strong> founder of theinfluential advertising agency Ogilvy <strong>and</strong> Mather, defined it thus:“The intangible sum of a product’s attributes: its name, packaging<strong>and</strong> price, its history, its reputation, <strong>and</strong> the way it’sadvertised.”The rebr<strong>and</strong> of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> coincides with the rebr<strong>and</strong>of DSM – the first for forty years. The new DSM br<strong>and</strong> promisesBright Science. Brighter Living. At <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> westrive in our own way to make continually evolving scientificinsights available to the ultimate benefit of the poorest<strong>and</strong> most disadvantaged populations of the world.Two newbr<strong>and</strong>s !
WelcomeA new look – an unchanging commitmentThis year, <strong>2011</strong>, sees the 25th anniversary of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>. Wecelebrate this significant milestone in our history with the launchof a new <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> br<strong>and</strong> – one that illustrates our move froma focus on vitamin A <strong>and</strong> sight to the vital role played by multiplemicronutrients in promoting health <strong>and</strong> preventing hidden hunger.This is the first issue of our magazine to reflect our new look<strong>and</strong> feel. As we celebrate 25 years of service in the field of micronutrients,we look back to where we have come from <strong>and</strong> lookforward to where we need to go. For despite our achievements inthe first quarter-century of our existence, our work in the worldis more vital today than ever before.The founding of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>The <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Task Force, as it was originally known, commencedoperations on 1 April 1986. Its objective was to helpcombat xerophthalmia – the eye disease caused by vitamin Adeficiency from which approximately ten million young childrenin developing countries suffered at the time. The 1986 <strong>Sight</strong> <strong>and</strong><strong>Life</strong> Annual Report estimated that every year, one million of thesechildren lost their eyesight. Of these, it noted that two-thirdsdied after a short period.A direct response to requests from the World Health Organization,the creation of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> was part of a much widerapproach to tackling vitamin A deficiency, which had been identifiedby the 37th World Health Conference as one of the five mainnutritional problems in the world. The initial activities of <strong>Sight</strong><strong>and</strong> <strong>Life</strong> included the provision of scientific <strong>and</strong> technical support,free distribution of vitamin A capsules for emergency situations,<strong>and</strong> financial support for selected research programs.“Our work is more vital todaythan ever before”Over the past 25 years, our focus has broadened to encompassthe entire spectrum of micronutrients, reflecting advances in scienceon the one h<strong>and</strong> <strong>and</strong> the increasingly recognized burden ofconcurrent multiple micronutrient deficiencies on the other. In2007, marking our 21st anniversary, I wrote in our Annual Reportthat we still faced the problem of two billion people worldwidebeing affected by hidden hunger. Further, I noted that it was unacceptablethat approximately one third of all children under fiveyears of age worldwide were stunted <strong>and</strong> almost 50% anemic,while at the same time some 155 million school-age childrenwere overweight or obese. These problems cannot be addressedby concentrating on vitamin A alone. Hence the widening of ourfocus to comprise the entire range of micronutrients.Our new logoThis exp<strong>and</strong>ed focus is expressed by our new logo, which symbolizesthe multiplicity of micronutrients essential for a healthylife. Whereas our original logo was based on the letter A <strong>and</strong>the human eye, clearly linking vitamin A with eye health, thisnew one puts <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> at the nexus of better nutrition <strong>and</strong>health. Whether this means growing the evidence, sharing information,advocating, promoting partnerships, or capacity buildingin the micronutrient arena, the message is clear: <strong>Sight</strong> <strong>and</strong><strong>Life</strong>’s mission is to build bridges for better nutrition focusing onlife, using a multiplicity of approaches <strong>and</strong> interacting with awide range of stakeholders.We hope that you too will like the new logo <strong>and</strong> also enjoy thenew look <strong>and</strong> feel of the magazine. Our intention was to createa publication that retained the scientific rigor for which our organizationhas always been known while presenting the contentin a more accessible <strong>and</strong> compelling manner. The <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>team welcomes your feedback – please let us know what youthink, as the magazine is produced not for us but for you, thereader.⇢
8EDITORIALOur history between two coversWhile April <strong>2011</strong> is the quarter-centenary of the founding of<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, we will be officially celebrating our birthday inOctober of this year, to tie in with World Food Day, which is celebratedevery year around the world on 16 October, <strong>and</strong> which Iwould like to see renamed World Food <strong>and</strong> Nutrition Day to recognizethat food does not automatically mean nutrition providingall the required micronutrients. Our jubilee celebrations willbe accompanied by the launch of a book recounting our 25-yearhistory in the context of the global fight against malnutrition. Ittells the story of the founding of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, of our changingfocus over the course of time, <strong>and</strong> of our enduring commitmentto combating malnutrition worldwide. Watch this space for morenews of the book launch!As I mentioned in my opening remarks, our commitment tocombating global micronutrient malnutrition is more necessarythan ever before. I am writing this editorial against the backdropof extensive political unrest in the Arab world. Tunisia, Algeria,Syria, the Yemen <strong>and</strong> Egypt have witnessed unprecedented uprisingsagainst long-established governments; Libya is in a stateof civil war as we prepare to go to press. While the reasons forthese revolts are multi-faceted <strong>and</strong> vary in their detail from countryto country, there can be no doubt that the rising cost of foodis one of the main drivers. The populations of North Africa haveto dedicate 35 to 50% of their income to food (contrast this withthe USA, for instance, where the figure is 7%). From 2010 to <strong>2011</strong>,the cost of wheat rose by 73%, that of maize by 88%.While these figures are already shocking, the future promisesto bring even more challenges. Global consumption of cerealsin 2010 amounted to two billion tons. This figure will doubleby 2050 in the light of unprecedented population growth. Andwhile the world’s population is growing, the resources availableto feed it are shrinking: the rising sea levels associated with climatechange are likely to eliminate vast swathes of l<strong>and</strong> in thecourse of time, especially in the world’s poorest countries thatcannot afford costly flood defenses. At the same time, urbanizationcontinues inexorably: in China alone, half a million hectaresof arable l<strong>and</strong> disappear each year as a result of that country’sspectacularly developing infrastructure.is written not only against the backdrop of the current politicalupheavals in the Arab world but also in the light of the appallingscenes following the earthquake <strong>and</strong> tsunami in Japan thathave claimed thous<strong>and</strong>s of lives <strong>and</strong> left the country battling forsurvival in the face of a nuclear disaster whose possible consequencescan barely be imagined. Already we are hearing reportsof food <strong>and</strong> water that has been contaminated by radioactivity.“The task before us is greaterthan ever”At a moment in the history of our organization that calls forcelebration, <strong>and</strong> for honoring the efforts of everyone who hashelped to make <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> what it is today, the task beforeus is greater than ever. Born in response to the famine createdby the war in Ethiopia in the mid-1980s, <strong>and</strong> initially focused onthe prevention of xerophthalmia caused by vitamin A deficiency,<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> now works across the entire spectrum of micronutrients,creating the bridges that link scientific research, policymaking<strong>and</strong> programs on the ground. We have more opportunitiesto influence the world than ever before. We also have morechallenges. Our commitment in the face of those challenges is asstrong as ever. The spirit of the 1986 <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Task Forcelives on in today’s organization, <strong>and</strong> we are proud to carry itforward with us into the next quarter-century.Yours sincerely,“We are committed to combatingmalnutrition worldwide”In 2008 this publication predicted that micronutrient malnutritionwould result from the rising price of food. The issuein question was written against the background of the 2008 cyclonethat hit Burma <strong>and</strong> the earthquake that devastated areasof China in the late spring of the same year. The present editorial
9“Roche had decided to make a formal commitmentto the battle against vitamin A deficiency, buildingon the ad hoc interventions it had already been supportingfor a number of years,” recollects ProfessorAl Sommer, Dean Emeritus, Johns Hopkins BloombergSchool of Public Health.The story:how …… <strong>Sight</strong><strong>and</strong> <strong>Life</strong> …“Dr John Gmünder would drop by from time to time todiscuss this undertaking <strong>and</strong> seek advice as to whereRoche should be focusing its efforts. We at Bloombergwere aware at the time that vitamin A had a hugeinfluence on physical <strong>and</strong> mental well-being. The linkhad not yet been proven, however, <strong>and</strong> the rest of theworld seemed reluctant to accept the theory.“One day John told me that Roche had decided tosponsor a new organization called <strong>Sight</strong> or <strong>Life</strong> –the implication being that if you couldn’t see, youweren’t living. I felt, however, that this sent too negativea message, <strong>and</strong> that it might be construed asoffensive by people who were blind <strong>and</strong> lived veryfull lives. I therefore suggested calling the new organization<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, because vitamin A is importantfor sight specifically but also for life in general.This little change gave the Task Force a verypositive name, <strong>and</strong> one which was intimately associatedwith vitamin A.”… gotits name.
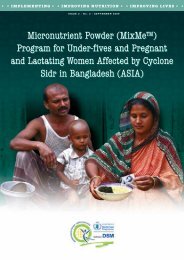
10 SIGHT AND LIFE STATEMENT<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>StatementLow Dose Iron Multiple MicronutrientPowder: Rationale for Use in MalariaEndemic AreasMultiple micronutrient powders (MNPs) are packaged in singleor multi-dose sachets. These sachets contain micronutrientsin powdered form, <strong>and</strong> can be added to foods prepared in thehousehold just before consumption. Usually, one dose of MNPprovides the full unit of recommended nutrient intake (RNI) ofvitamins <strong>and</strong> minerals.In 2007, the use of MNPs, particularly in emergency conditions,was endorsed by the World Health Organization (WHO),the World Food Programme (WFP) <strong>and</strong> the United NationsChildren’s Fund (UNICEF) as an effective way of improving themicronutrient status of nutritionally vulnerable sections of thepopulation, such as children under five years of age <strong>and</strong> pregnant<strong>and</strong> lactating women. 1The risk of untargeted iron supplementationBased on results from a study conducted in Zanzibar 2 <strong>and</strong> otherbodies of evidence, 3,4 it was concluded that untargeted iron supplementationmay increase child morbidity <strong>and</strong> mortality frommalaria in the absence of monitoring <strong>and</strong> treatment programs.A sub-study analysis suggested that adverse events occurredin supplemented children who had not been iron-deficient. TheWHO Consultation on Prevention <strong>and</strong> Control of Iron Deficiencyin Infants <strong>and</strong> Young Children in Malaria Endemic Areas 5 concludedthat the safety of home fortification, as practiced at thattime, is uncertain, whereas food fortification programs are stillregarded as safe. In the above-mentioned study in Zanzibar, thenegative impact on iron-replete children was demonstrated atlevels of 12 mg Fe (as FeSO₄ supplement) per day. The bioavailabilityof FeSO₄ from a supplement is considerably higher thanbioavailability from fortified food, where the amount of availableiron depends on the food matrix. The children who showedadverse effects during iron supplementation had therefore beenexposed to high doses of absorbed <strong>and</strong> unabsorbed iron.As a result, the micronutrient powder mix for malaria endemicareas designed by DSM contains a significantly lower dose ofiron (2.5 mg, as NaFeEDTA) in combination with a known enhancerof iron absorption (ascorbic acid). This iron dose is closeto or even lower than amounts provided in food fortification programs,<strong>and</strong> is not comparable to the bolus doses administeredin iron supplementation programs. A consequence of the loweriron dose contained in the MNP sachets is the need to ensurethat the amount of (bioavailable) iron delivered is high enoughto the cover the needs of the individual.Currently the compound used is NaFeEDTA, which belongs toa group of iron compounds with a high relative bioavailabilitycompared to ferrous sulphate (FeSO₄). The main advantage ofNaFeEDTA is better bioavailability in the presence of iron absorptioninhibitors such as phytic acid <strong>and</strong> tannins, whereas thebioavailability of FeSO₄ is heavily dependent on the presence orabsence of such inhibitors. In particular, home-fortification islinked to the consumption of the local diet or local complementaryfoods, where starchy staples with a significant amount ofiron absorption inhibitors are consumed. In addition, accordingto the latest recommendations for flour fortification, 6 NaFeEDTAis the recommended compound for flours with high levels ofphytates (e.g. maize flour).Possible explanations for the Zanzibar resultsTwo possible explanations for the results seen in Zanzibar havebeen proposed: the formation of non-transferrin-bound iron(NTBI) in plasma, <strong>and</strong> the stimulation of pathogen growth in thegastrointestinal tract (due to the amount of unabsorbed iron).It has been proposed that administration of bolus doses of ironcan result in large amounts of unabsorbed iron, which enters<strong>and</strong> passes through the intestine. Recently published results 7indicate that unabsorbed iron from fortified foods modifies the
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> 11“The main advantage ofNaFeEDTA is better bioavailabilityin the presence ofiron absorption inhibitors.”
12 SIGHT AND LIFE STATEMENTcolonic microflora in African children to create a potentiallymore pathogenic profile. If this is confirmed, it could help to explainthe reported adverse effects of iron supplementation <strong>and</strong>bolus doses of iron.The other potential mechanism discussed is the formationof non-transferrin-bound iron (NTBI). Recently presented dataon the formation of NTBI 8 after administration of iron in womenwith low iron status (NTBI formation monitored over eight hours),showed that the highest NTBI concentrations were produced bya 60 mg dose without food, followed by 60 mg <strong>and</strong> 6 mg withfood. These first data indicate that iron administered with food<strong>and</strong> through fortification (rather than supplementation) resultedin lower NTBI formation.“The two-step approach of optimizingthe MNP formulation for malariaendemic areas is expected to be saferthan typically used iron doses”In conclusion, based on current knowledge, the two-step approachof optimizing the MNP formulation for malaria endemic areasis expected to be safer than typically used iron doses (12.5 mg).The reduction of the iron dose to levels closer to the amount of ironprovided in food fortification helps to reduce the amount of unabsorbediron in the intestine. Meanwhile, using a highly bioavailableiron compound in combination with iron absorption enhancersis crucial to supplying the individual with the iron needed.References01. WHO/WFP/UNICEF Joint Statement. Preventing <strong>and</strong> controllingmicronutrient deficiencies in populations affected by an emergency.Multiple vitamin <strong>and</strong> mineral supplements for pregnant <strong>and</strong>lactating women, <strong>and</strong> for children aged 6 to 59 months. WHO,2007.02. Sazawal, S, Black R, Ramsan M et al. Effects of routine prophylacticsupplementation with iron <strong>and</strong> folic acid on admission to hospital<strong>and</strong> mortality in preschool children in a high malaria transmissionsetting: community-based, r<strong>and</strong>omized, placebo-controlled trial.Lancet 2006;367(9505):133–4303. Oppenheimer SJ. Iron <strong>and</strong> its relation to immunity <strong>and</strong> infectiousdisease. J Nutr 2001;131(2S-2):616S-633S; discussion 633S–635S.04. Ojukwu J, Okebe J, Yahav D et al. Oral iron supplementation forpreventing or treating anemia among children in malaria-endemicareas. Cochrane Database Syst Rev 2009;(3): CD006589.05. WHO. Conclusions <strong>and</strong> recommendations of the WHOConsultation on prevention <strong>and</strong> control of iron deficiency in infants<strong>and</strong> young children in malaria-endemic areas. Food Nutr Bull2007;28:S621–S706. Hurrell, R, Ranum P, de Pee S et al. Revised recommendations foriron fortification of wheat flour <strong>and</strong> an evaluation of the expectedimpact of current national wheat flour fortification programs.Food Nutr Bull 2010;31(1 Suppl):S7–2107. Zimmermann, M, Chassard C, Rohner F et al. The effects of iron fortificationon the gut microbiota in African children: a r<strong>and</strong>omizedcontrolled trial in Côte d'Ivoire. Am J Clin Nutr 2010;92:1406–15.08. Egli I, Brittenham G, Zeder C et al. The influence of supplementation<strong>and</strong> fortification iron doses on the formation of plasma-nontransferrin-boundiron. (UC Davis) Conference on Bioavailability,Asilomar, CA, September 26–30, 2010 (only abstract available)
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>13The “<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>in My <strong>Life</strong>”Essay CompetitionIn the last issue of the magazine, we launched the <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> inMy <strong>Life</strong> Essay Competition. Its aim was to find out how <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> hasplayed a part in readers lives, as part of the organization’s 25thanniversary.The closing date for the competition was 15 March <strong>2011</strong> <strong>and</strong> we havereceived many wonderful stories. We have been delighted with theentries we have received <strong>and</strong> are looking forward to sharing these withyou in future issues. We are now in the process of reading <strong>and</strong> judgingthe entries <strong>and</strong> will be contacting the winners <strong>and</strong> those who sent ushighly commended entries later this summer.We have received entries from many countries, from Nigeria to SriLanka. Many fascinating photographs <strong>and</strong> even some original artworkhas come our way, such as the picture here by Dr Narendra Kumar,which is the cover of her booklet that helps children <strong>and</strong> families inIndia.We would like to say a very heartfelt thank you to all you who enteredthe competition. We appreciate the time you have spent on writing yourentries <strong>and</strong> would also like to thank you for all the amazing good workyou do in your communities.With warmest wishesThe <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Team
16THE IMPORTANCE OF VITAMIN AThe Importance of Vitamin Afor the Development<strong>and</strong> Function of Lungs inNewbornsHans Konrad BiesalskiUniversity of Hohenheim,Stuttgart, GermanySummaryVitamin A is essential for growth <strong>and</strong> development, inparticular for the adequate maturation of the lung in lateembryogenesis. If the developing embryo is not supplied withsufficient amounts of vitamin A delivered from the mother, embryoniclung retinyl ester stores remain low. As a consequence,the sources for retinol <strong>and</strong> subsequently the active metaboliteretinoic acid, important for gene expression in the lung, are notsufficiently available during the time of lung maturation.Low vitamin A stores in the lung impair the expression of surfactantproteins, alveoli formation <strong>and</strong> the development of therespiratory epithelium. Newborns with low vitamin A storesare at risk for respiratory diseases such as bronchopulmonarydysplasia <strong>and</strong> frequent infections in early childhood.IntroductionVitamin A is essential for the growth <strong>and</strong> development of cells<strong>and</strong> tissues. In its active form, retinoic acid (RA), it controls regulardifferentiation as a lig<strong>and</strong> for retinoic acid receptors (RAR,RXR). 1,2 Vitamin A plays a substantial role in the respiratoryepithelium <strong>and</strong> the lung. In the presence of moderate vitamin Adeficiency the incidence of diseases of the respiratory tract isconsiderably increased. Repeated respiratory infections can beinfluenced therapeutically by moderate vitamin A supplementation.3,4,5 Besides its importance for lung function, vitamin A isalso responsible for the development of many tissues <strong>and</strong> cells,as well as for embryonic lung development. Recent studies havedemonstrated that this occurs by various expressions of retinoidreceptors, as well as by time-dependent changes of the vitaminA concentration in the tissue. Where maternal vitamin A isdeficient fetal lung maturation might be seriously impaired, withconsequences for postnatal function.The influence of vitamin A on the maturation<strong>and</strong> differentiation of the lungVitamin A <strong>and</strong> its major active metabolite RA have a profoundinfluence on the alveolar development, maintenance <strong>and</strong> functionof the lung. Type II alveolar cells synthesize <strong>and</strong> secretesurfactant. 6 RA is able to stop – dependent on its concentration7 – the expression of the surfactant-protein A (SP-A) in humanfetal lung explants. Insulin, TGF- <strong>and</strong> high concentrationsof glucocorticoids can also down-regulate the expression of SP-A-mRNA, 8 but lower concentrations of glucocorticoids stimulatethe expression of these genes. 9 In contrast, the expression ofSP-A-mRNA is increased by hyperoxia in rats 10 <strong>and</strong> by dexamethasonein human fetal lung explants. 7Type PGE₂ prostagl<strong>and</strong>ins are able to increase surfactantsynthesis. Under the influence of EGF (epidermal growth factor)the formation of prostagl<strong>and</strong>in rises, especially that of PGE₂. Onthe other h<strong>and</strong>, the expression of the EGF receptor is increasedby RA. EGF increases proliferation of the lung tissues, leadingto an amplified formation of surfactant phospholipids. 11 RA <strong>and</strong>EGF both lead to an increase (40%, 80%) in the secretion ofPGE₂ in fetal lung cells of the rat in vitro. 12 The combination ofRA <strong>and</strong> EGF, however, leads to a more than a six-fold increasein the secretion of PGE₂. Consequently, RA can interfere in lungdevelopment due to its modulating effect on the expression ofEGF <strong>and</strong> the subsequent PGE₂-induced surfactant formation.Sufficient <strong>and</strong> continuous availability of vitamin A (either on theblood pathway or from local storage sites) is pivotal, especially
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>17“Repeated respiratoryinfections can be infl uencedtherapeutically by moderatevitamin A supplementation.”
18 THE IMPORTANCE OF VITAMIN Afor the timely regulation of lung development <strong>and</strong> the relatedformation of the active metabolite RA. During embryonic development,RA regulates cell proliferation <strong>and</strong> differentiation, <strong>and</strong>regular morphogenesis. In the postnatal period, RA is important13, 14for lung growth, alveolarization, <strong>and</strong> elastin formation.“The combination of RA <strong>and</strong> EGF leadsto more than a six-fold increase of thesecretion of PGE₂”Vitamin A kinetics during fetal lung developmentLocal extrahepatic stores are present in fibroblast-like cells closeto the alveolar cells, in type II cells <strong>and</strong> in the respiratory epitheliumretinyl esters. The importance of these retinyl esters asan acute reserve during the development of the lung becomesapparent during the late phase of gestation <strong>and</strong> the beginningof lung maturation. During this period, rapid emptying of theretinyl ester stores in the lung of rat embryos occurs. 15 This depletionis the result of increased RA dem<strong>and</strong> in the lung developmentprocess, because RA is instantly needed for the processof cellular differentiation <strong>and</strong> metabolic work. Indeed, RA is importantfor the formation of alveoli, <strong>and</strong> may rescue failed alveolarformation. 16,17 The effect of an adequate amount of RA onalveolar formation which starts prior to birth <strong>and</strong> lasts up to theage of eight years or even longer has recently been documented.Checkley <strong>and</strong> co-workers 18 reported that children of mothersfrom a region with vitamin A deficiency who were supplementedduring pregnancy <strong>and</strong> for six months after pregnancy with 7 mgpreformed vitamin A (7 mg retinol equivalents, RE) as a singleoral supplement once a week had significantly better lung functionat nine to 11 years old than those of mothers receiving eithera placebo or 42 mg -carotene (7 mg RE).“Vitamin A supplementation before,during <strong>and</strong> after pregnancy improvedlung function in offspring”was no further supplementation six months after delivery in thevitamin A deficient area, how might improvements of the lungfunction 10 years later be explained? One explanation might bethe sufficient repletion of vitamin A storing cells in the lung ofthe offspring, which may serve as storage sites for a longer timeperiod. Retinyl ester stores have been described in lipid-ladenfibroblasts 21 <strong>and</strong> in the bronchiolar epithelium. 22 These lipidinterstitial cells deliver RA, which induces alveolus formation. 23In the alveolus, the lipid-laden fibroblast is a major contributorto the formation of the extracellular matrix. 24 Following hydrolysisof retinyl esters to form retinol, retinol is oxidized via alcoholdehydrogenase (ADH) followed by irreversible oxidation to retinoicacid. All steps are tightly controlled via intracellular bindingproteins. Retinol bound to the cytoplasmic retinol binding protein(holo-CRBP) is protected from degradation <strong>and</strong> delivered tothe lecithin: retinol acyltransferase (LRAT) for esterification. 25Cytoplasmic retinoid binding proteins form a substrate-controllednetwork, which at least controls the delivery of RA to thenuclear-related metabolic enzymes (LRAT, ADH) via a feedbackmechanism. 26,27 This feedback network might explain why afigure 1: Decline of retinyl palmitate concentration<strong>and</strong> in-crease of retinol in embryonic rat lungs prior to <strong>and</strong>shortly after birth (Geevarghese <strong>and</strong> Chytil) 15Retinyl palmitate (μg/g weight)12111098Birth7654321018 19 20 21 22Gestational age (days)2,50Vitamin A kinetics during lung developmentThe fact that the -carotene group had no benefit regardinglung function may be due to either poor absorption, a lowercleavage rate or polymorphism of the -carotene monooxygenase(BCMO), as discussed recently. 19,20 Administration of preformedvitamin A will contribute to a more sufficient supply ofthe lung. The effect of vitamin A on later lung function mightbe a consequence of adequate alveolar formation during fetallung development <strong>and</strong> during early childhood. However, if thereRetinol (μg/g weight)2,252,001,751,5018 19 20 21 22Gestational age (days)Birth
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 1919figure 2: Time dependent pattern of pre- <strong>and</strong> postnatal CRBP <strong>and</strong> CRABP in rats. CRABP increases during the first days of lifeas a sign of increased formation of RA. (Ong <strong>and</strong> Chytil, 1976) 69nmol CRBP/g lung ( )0.2 0.20.1 0.10 0nmol CRABP/g lung ( )Saccules Septation ThinningAlveoli–3 –1 0 1 3 5 10 12 15 21AdultAge, dayscombination of RA <strong>and</strong> retinyl palmitate, given orally on postnataldays 5–7, significantly increases lung retinyl esters in neonatalrats compared to RA <strong>and</strong> vitamin A alone. 28 RA increasesesterification of retinol <strong>and</strong> blocks hydrolysis of retinyl palmitateto avoid RA overload of the cells. Liver vitamin A stores, aswell as plasma levels of retinol <strong>and</strong> retinol binding protein (RBP),are relatively low at birth. 29-32 Consequently, sufficient prenatalpulmonary retinyl ester stores <strong>and</strong> their metabolization to RA inthe lung are the critical component regulating fetal lung maturation,including alveolarization <strong>and</strong> postnatal function.Three days prior to delivery, the retinyl ester stores of ratfetal lungs decline <strong>and</strong> the retinol concentration increases. 15(Figure 1)Retinol is metabolized to RA, which serves as a lig<strong>and</strong> for thenuclear receptors, which control the gene expression of variousproteins responsible for late lung development <strong>and</strong> maturation.Impact of steroids on lung developmentPrenatal lung development is also influenced by glucocorticoids.Steroid hormones have a similar effect on lung development tovitamin A, <strong>and</strong> the two factors complement each other. This is notsurprising, however, as the receptors for steroids <strong>and</strong> retinoidsbelong to the same multireceptor complex. The mode of actionof glucocorticoids exists not only on the level of gene expression,but seems also to have an impact during a much earlier phase ofvitamin release. The application of dexamethasone leads to anincrease in the maternal <strong>and</strong> fetal retinol binding protein, leadingto an improvement of the vitamin A supply by channeling outvia the normal hepatic pathway. This increase in the vitamin Aconcentration in the systemic circulation clearly diminishes themorbidity <strong>and</strong> mortality attributable to bronchopulmonary dysplasia33,34 in the case of babies born prematurely.Dexamethasone <strong>and</strong> glucocorticoids not only lead to an improvementof the total vitamin A supply through a change of therelease from the liver; but also influence, as recently described, 15the metabolization of the vitamin A esters stored in the lung. Followingadministration of dexamethasone, even without steroidapplication, a significant reduction of retinyl esters in the maturinglung can be detected, as well as a moderate increase inretinol, the hydrolysis product of retinyl esters. This observationmay explain therapeutic successes with steroids, as well as theirfailures in cases of poor retinyl ester stores, during the therapyof lung distress syndrome of premature infants.Vitamin A binding proteinsA further component involved in the hydrolysis <strong>and</strong> formation ofretinyl esters is the concentration of CRBP. 35 A high apo-CRBPconcentration increases the activity of the retinyl ester hydrolase,which subsequently results in an increase in retinol <strong>and</strong>,as a consequence, an increase in holo-CRBP. Lig<strong>and</strong>ed CRBPis responsible for the delivery of retinol to LRAT for esterification.36 Indeed, lipid-laden pulmonary interstitial fibroblasts derivedfrom perinatal rat lungs show a high CRBP concentration,which declines following the formation of retinol <strong>and</strong>, finally,retinoic acid during the early postnatal period. 37 (Figure 2)Where the supply of Vitamin A is insufficient, inadequate retinylester stores due to a shortage in the supply to the fetal lungduring late pregnancy mean that glucocorticoids <strong>and</strong> apo-CRBPcannot act to regulate vitamin A metabolism in the lung cells.Consequences of marginal deficiencyMasuyama <strong>and</strong> co-workers 38 demonstrated that a marginal vitaminA deficiency, which is not necessarily detected via lowplasma retinol due to homoeostatic control, may have an importantimpact on late lung development. (Figure 3)They also documented an additional aspect: Retinyl ester increasedrapidly to a peak on day 17 of gestation <strong>and</strong> decreasedto a minimum on day 21 of gestation. These data show that there
20 THE IMPORTANCE OF VITAMIN ARetinyl palmitate (μg/g weight)figure 3: Pattern of retinyl ester concentration inthe pre- <strong>and</strong> post-natal rat lung (Masuyuma et al., 1997). 38The data show the 10-fold concentration of retinyl estersin the fetal lung, compared to the adult lung of the rat.The rapid decline prior to birth documents theimportance of retinyl ester hydrolysis to form retinol<strong>and</strong> subsequently retinoic acid. The latter controlslung maturation.6543Birth21015 17 19 21 1 3 5 7 AdultPrenatal Postnatalmight be a very small window during which the retinyl esters arestored in the lung shortly before they are needed. If, in the caseof early delivery, the stores are not adequately filled, this mighthave serious consequences for lung maturation. Retinoic acidreceptor (RAR) <strong>and</strong> RAR mRNA were detected in all samplesobtained from perinatal <strong>and</strong> adult rat lung, but only a trace ofRAR mRNA was detected in the fetuses on days 15, 17 <strong>and</strong> 19of gestation <strong>and</strong> in adults. After a maternal retinol deficiency of28 days, fetal body <strong>and</strong> lung weights were significantly lowerthan those of the controls; concentrations of retinyl palmitate<strong>and</strong> phosphatidylcholine (PC) in the lung after a maternal retinoldeficiency over 14, 21, or 28 days were significantly lowerthan those of controls. Expression of RAR mRNA in the groupwith 28-day retinol deficiency was lower than in controls. Thatof RAR mRNA was increased <strong>and</strong> that of RAR mRNA was notinfluenced by retinol deficiency. In the developing mouse embryo,RAR expression is spatially <strong>and</strong> temporally restricted invarious tissues, suggesting a role for RAR in morphogenesis. 39RAR is both a strong target for RA <strong>and</strong> also highly activated bytreatment with exogenous RA. 40 The rate of choline incorporationinto PC in fetal lung explants was significantly higher in thegroup treated with RA than in the controls. RA enhanced theeffect of epidermal growth factor on choline incorporation <strong>and</strong>prevented that of dexamethasone. Taken together, marginal deficiencyresults in the altered expression of nuclear receptors ofvitamin A, with impaired maturation as a consequence.The influence of vitamin A supply for the post-nataldevelopment of the lung in preterm infantsAn adequate vitamin A intake during pregnancy is of great importancefor the formation of retinyl ester stores in the developinglung. These stores are the basis for RA formation during lungmaturation <strong>and</strong> postnatal function, with long-term benefits asabove. 18 However, in the case of early delivery or very low birthweight, an insufficient vitamin A supply during pregnancy mighthave serious consequences.A disease observed recurrently in connection with vitamin Asupply is bronchopulmonary dysplasia (BPD). The pathogenesisof BPD certainly depends on a multitude of factors. Some of theobserved morphological changes are strongly reminiscent ofvitamin A deficiency in humans <strong>and</strong> animals. Of particular noteis the focal loss of ciliated cells with keratinizing metaplasia <strong>and</strong>necrosis of the bronchial mucosa, as well as an increase in mucoussecreting cells. 41Focal keratinizing metaplasia, such as may occur after vitaminA deficiency, especially strengthens the assumption of animpairment of differentiation on the level of gene expression.Since vitamin A regulates the expression of different cytokeratins<strong>and</strong> therefore influences terminal differentiation, it seemsobvious to assume the existence of common mechanisms. Consequently,premature neonates are dependent on a sufficientsupply of vitamin A to ensure adequate lung maturation. Theearlier a child is born before its due date, the lower its serumretinol levels. 31Retinol serum levels in neonatesIt was shown repeatedly that serum retinol level <strong>and</strong> RBP leveldepends on birth weight <strong>and</strong> is significantly lower in prematureinfants with low birth weight, compared to similar-aged neonateswith higher birth weight. 30 In addition, mothers from lowincome groups had lower levels of serum vitamin A <strong>and</strong> a higherincidence of prematurity. 42 Significantly lower retinol levels canbe found in the liver of premature infants, in comparison to neonates.43 Plasma values lower than 0.70 μmol/L are not rare inthis case, <strong>and</strong> they should be taken as an indicator of a relativevitamin A deficit.Very low plasma vitamin A levels can be found recurrentlyin premature infants compared to term neonates. 44,45 This can,among other things, be attributed to the relative immaturity ofthe liver for the synthesis of retinol binding proteins. The neonateis almost exclusively dependent on the mother for its supply: thisincludes the lung retinyl esters which are either directly absorbedby the cells (from chylomicrons) or by esterification of retinolafter uptake into the cells. These lung retinyl ester stores can onlybe sufficiently filled if the mother guarantees an appropriate vitaminA supply, especially during late pregnancy.Reduced plasma levels during the first developmental months
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 2121have a considerable influence on the total development of infants,as well as on their susceptibility to infections. In the caseof reduced retinol plasma levels, repeated infections are moreoften described, 3,46 <strong>and</strong> are counted among the main complicationsof a poor vitamin A supply in developing countries. Inaddition, the serum vitamin A level during infectious diseases,particularly of the respiratory tract, continues to drop. 47,48 Thiscan be explained on the one h<strong>and</strong> by an increased metabolicdem<strong>and</strong>, <strong>and</strong> on the other h<strong>and</strong> by renal elimination of retinol<strong>and</strong> of RBP during the process of acute infections. 49 If the retinylester stores of the lung are low at delivery, these storage sites arereplenished with difficulty, <strong>and</strong> as a consequence lung functionmay be impaired.Marginal vitamin A deficiency in developed countriesEven in developed countries with a wide variety of food containingpreformed vitamin A, low plasma levels (
22 THE IMPORTANCE OF VITAMIN ADespite low plasma retinol levels, most of the women had high-carotene levels (80% >0.5 μmol/L). However, the high levelsof -carotene in plasma may be taken as a sign of low conversionto vitamin A due to the recently described BCMO polymorphism.20 As a consequence, these women are at risk of low vitaminA supply due to a very low intake of preformed vitamin A.This results in very low levels of retinol in blood <strong>and</strong> breast milkfor the newborn.There is limited data linking the intake of vitamin A duringpregnancy to cord blood levels <strong>and</strong> fetal development. Shah <strong>and</strong>co-workers demonstrated a strong relationship between lowsocio-economic status, low cord blood <strong>and</strong> low body weight ofthe newborn. 44If there is evidence that the vitamin A status of the mother ispoor, a parenteral supply (intramuscular application) is recommended.The impact on the general health of the child includinglung function is controversial, however.Prevention <strong>and</strong> therapyIn view of the importance of vitamin A, as above, the questionarises as to possible therapeutic interventions – especially forimminent premature deliveries, but also for premature infants<strong>and</strong>, in cases of poor maternal vitamin A status, for prevention ofpotential diseases <strong>and</strong> /or immaturities of the lung. Where thereis a risk of prematurity, vitamin A might be delivered antenatally,regardless of maternal vitamin A status, to ensure sufficient fetallung retinyl ester stores. Based on US Dietary Reference Intakerecommendations, daily vitamin A supplementation during anypart of the fertile period should be limited to 3,000 IU. However,a moderate dosage <strong>and</strong> a short period of supply might notbe sufficient to replete lung retinyl ester stores in cases of poormaternal vitamin A status. Higher doses during the last termof pregnancy might be more effective <strong>and</strong> pose no risk of teratogenicity,but this has not been proven to date.One solution could be the intravenous administration of vitaminA. However, with the infusion systems used so far it appearsthat vitamin A is almost completely absorbed by the polyethylenetubes <strong>and</strong> is damaged by light. 6 One way of improvingavailability consists of coating the infusion systems with foil toavoid further loss of the vitamin due to light. Since such solutionsare no longer available on the market <strong>and</strong> new parenteralvitamin A preparations are not yet available, the importance ofsupplying the mother with vitamin A before delivery needs tobe highlighted. Parenteral administration of retinyl margarinate(an unphysiological fatty acid ester of retinol) resulted in arapid increase of retinyl margarinate <strong>and</strong> further retinyl esters(as a result of hydrolysis <strong>and</strong> re-esterification) in several tissues,including the lung, in vitamin A depleted rats. 52 The results ofthis study clearly document that retinyl esters can be taken upinto different tissues circumventing the liver <strong>and</strong> the control ofdelivery via retinol-RBP. At present there are no data regardingthe risk of parenteral vitamin A supply in pregnant women witha high risk of preterm labor (e.g. those on bed rest). However,because teratogenic effects occur during the first term, adminisfigure5: Retinol <strong>and</strong> -carotene in maternal plasma, cord blood <strong>and</strong> colostrum in women who delivered twins (n=6) (A)or women with short birth intervals (n=24) (B). (Schulz et al., 2007) 507.5A***2.5B2.0Retinol [μmol/L]5.02.5*-carotene [μmol/L]1.51.00.50.0MaternalplasmaCordplasmaColostrum0.0MaternalplasmaCordplasmaColostrum*p
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 2323figure 6: Model of VA metabolism in neonatal rat lung (Wu <strong>and</strong> Ross, 2010) 68ARA, 6 hThe two panels represent the observed <strong>and</strong> proposed pathways ofretinoid uptake, esterification, <strong>and</strong> oxidative metabolism in theRELRATROHCyp26B1RAPolarmetaboliteslungs of neonates treated with RA for 6 h (A) <strong>and</strong> 12 h (B). Changesin gene expression represent the effects of the acidic retinoids, with<strong>and</strong> without VA, while retinol uptake <strong>and</strong> retinyl ester formation re-VAStra6present the treatments that included VA.A When RA is administered to neonatal rats with a supplementof VA, RA up-regulates the expression of LRAT <strong>and</strong> CYP26B1 to theBRA, 12 hsame extent at 6 h, with the flow of retinol to RE formation or topolar metabolites kept in balance. More dietary retinol is taken upRELRATROHCyp26B1RAPolarmetabolitesby lung tissue due to up-regulation of STRA6 <strong>and</strong> elevated plasmaretinol at 6 h.B At 12 h, RA is metabolized by CYP26B1. Although the biologicalVAactivity of RA has declined, the pathway is still balanced as STRA6,LRAT, <strong>and</strong> CYP26B1 have all returned to basal levels.tration during the second or third term might be without any risk,<strong>and</strong> vitamin A could be administered to pregnant women with ahigh risk of preterm labor.Vitamin A supply <strong>and</strong> lung diseaseThe results of two r<strong>and</strong>omized double-blind controlled studies53,54 of premature infants show that supplementation withvitamin A in a study 54 led to a considerable reduction (55%) inthe risk of being affected by chronic lung disease of prematurity.In a third study, 55 12 premature infants received vitamin A intravenouslyfor a period of 28 days (400 IU/d) <strong>and</strong> during later developmentvitamin A was also administered orally (1,500 IU/d).During supplementation the initially reduced plasma <strong>and</strong> RBPvalues rose significantly. The latter is an indication of an actualvitamin A deficiency of premature infants, because an increase inretinol-RBP is only observed if a vitamin A deficiency really exists(the principle of the relative dose response test).“The significance of supplying themother with vitamin A before deliveryneeds to be highlighted”A direct effect of plasma concentration on the developmentof chronic lung disease of prematurity could not be determined.The author has come to the logical conclusion that the plasmalevel after delivery poorly reflects the supply of the lung withvitamin A before delivery. It should be borne in mind that thisstudy confirmed that relative vitamin A deficiency is characteristicof premature infants, in particular. Thus, attention shouldbe directed to their supply of vitamin A. On the other h<strong>and</strong>, thevitamin A supply of the premature infant appears to be eitherinsufficient to ensure adequate concentrations in the lung or theavailability of the vitamin to the corresponding cells of the lungis not guaranteed.All trials delivered vitamin A in doses of
24 THE IMPORTANCE OF VITAMIN Afigure 7a: Schematic model of retinyl ester storage in the neonatal rat lung following VARA 67AA Lung RE on postnatal (P) days 4 <strong>and</strong> 8 in newborn rats treatedLog ₁₀ RE + retinol, nmol/g lung2.62.42.22.01.81.61.41.21.00.80.60.40.20c,d(1.6)b(5.5)P4a(45.7)d(1.0)c(2.8)P8b(6.8)with VARA, vitamin A or oil. Newborn rats (n = 7/group) were treatedon days 1, 2 <strong>and</strong> 3 with oil (control), vitamin A alone, or VARA, <strong>and</strong>lung RE was determined on P4 (n = 4/group) <strong>and</strong> P8 (n = 3/group).Data are the mean SD <strong>and</strong> were analyzed by 2-way ANOVA afterlog ₁₀ transformation (as illustrated), <strong>and</strong> the least squares meanstest. Values shown in parentheses are the anti-logs of the log ₁₀ means.(Adapted from Ross <strong>and</strong> Ambavalanan, 2007) 67B Lung <strong>and</strong> liver retinyl ester in 8-day-old rats treated with oil(control), VARA, dexamethasone (Dex), or Dex <strong>and</strong> VARA. (1) A LungRE + retinol concentration. (2) B Liver RE + retinol concentration.(3) C Plasma total retinol. For each treatment, n = 3 pools/groupwere analyzed by HPLC; each pool contained equal portions of tissueControlVitamin A aloneVARAAge: 0.0001Treatment: 0.0001Age*Trt: 0.003a > b > c > d, p < 0.003from 2 identically treated neonates. The results were analyzed bytwo-way ANOVA; different letters above groups indicate significantdifferences by the least squares means test. (Adapted from Ross <strong>and</strong>Ambalavanan, 2007) 67leads to higher plasma concentrations of retinyl palmitate <strong>and</strong>,subsequently, to higher uptake of the retinyl esters into tissues.However, the fact that more cases of retinopathy <strong>and</strong> necrotizingcolitis occurred in the once-per-week dose group, comparedwith the 10,000 IU three times per week group, may be the consequenceof the solubilzer polysorbate. Hale <strong>and</strong> co-workers 57evaluated the effect of the solubilizer (polysorbate 80) in neonatalpigs. The authors speculate that “rapid intravenous injectionof vitamin E emulsions produces massive accumulation inphagocytic cells of the spleen <strong>and</strong> to a lesser extent liver <strong>and</strong>lung, possibly leading to increased susceptibility to sepsis <strong>and</strong>/or abnormal pulmonary function.” The intravenously suppliedvitamin E (E-Ferol) led to deaths in 38 cases in 1984 in the US<strong>and</strong> was consequently stopped. Because a mixture of polysorbate80 <strong>and</strong> polysorbate 20 is used as a carrier in E-Ferol, thesecomponents were also tested <strong>and</strong> were found to be responsiblefor the suppression, especially the polysorbate 80.Improving lung retinyl ester storesRoss <strong>and</strong> co-workers documented a way to improve vitamin Asupply to the lung via administration of preformed vitamin A(VA) <strong>and</strong> RA (VARA) in a ratio of 10:1. 58 Based on their data, Ross<strong>and</strong> co-workers created a model of how <strong>and</strong> why retinyl esterstores are formed following delivery of preformed vitamin A plusRA. RA induces CYP26 <strong>and</strong> LRAT to save the cell from high <strong>and</strong>potentially toxic concentrations. 59 As a consequence, the suppliedpreformed vitamin A entering the cell via the Stra6 receptoris stored as retinyl esters <strong>and</strong> the RA is detoxified; 6 h later,normal RA <strong>and</strong> ROH levels document the homoeostatic controlof the cell. (Figure 6)Ross <strong>and</strong> co-workers’ data also demonstrate that an isolatedsupply with RA might exert a short-term effect on lung maturation,but that, in the long term, the surplus of RA is detoxified<strong>and</strong>, consequently, without efficacy. In further experiments,James <strong>and</strong> co-workers showed that the synergistic effect of VARAon lung retinyl ester content was blunted in mice exposed tohyperoxia. 60 Regardless of the mechanism by which RA exerttheir effects, a sufficient content of retinyl esters or an increasefollowing the VARA application is essential for this benefit. Thecombination of VA <strong>and</strong> RA has the therapeutic potential of reducingBPD to a greater extent than VA or RA supplementationalone. (Figure 7)This data also clearly demonstrates that the usual approachto supply the lung of the newborn with vitamin A (intramuscularly)might be not very successful <strong>and</strong> explains the moderate<strong>and</strong> sometimes conflicting results. The proposed mechanismalso shows that delivery of RA alone might be counterproductive,<strong>and</strong> might lead to an up-regulation of the detoxifying enzymes(CYP26) <strong>and</strong>, in parallel, to an increased expression of CRABP,which may reduce RA action. The intramuscular supply in extremelylow birth weight infants with vitamin A might be also oflimited success, if it is not ensured that the liver can transport
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 2525figure 7b:BPlasma total retinol, μmol/LLiver RE + retinol, nmoL/gLung RE + retinol, nmol/g201816141210864204003503002502001501005002.52.01.51.00.501baControl VARA Dex VARA + DexVARA: 0.0001Dex: NS2cControlaVARA: 0.0001Dex: NS3bControlVARA: 0.0027Dex: NSbaVARA*Dex: NSa > b, p < 0.0001bVARA Dex VARA + DexaaVARA*Dex: NSa > b > c, p < 0.01bVARA Dex VARA + DexaVARA*Dex: NSa > b, p < 0.05retinol bound to RBP to the lung. Nevertheless, if an increase incirculating retinyl esters following parenteral application occurs,the retinyl esters are directly delivered to the cells. 52From recent data in two cases of completely impaired RBPsynthesis due to a mutation 61 it can be concluded that retinylesters delivered to cells <strong>and</strong> tissues can serve as major vitamin Asource.Inhalation of vitamin AAn alternative solution could be inhaled vitamin A. With this,the lung is directly targeted <strong>and</strong> retinyl esters administered byinhalation can be absorbed into the cells <strong>and</strong> metabolized in acontrolled way, as shown in various animal studies. 62 In addition,the inhalative approach results in an increase of vitamin Ain plasma <strong>and</strong> tissues of rats. 63 We reported successful vitamin Asupplementation by inhalation of retinyl palmitate in a placebocontrolledpilot study in 25 pre-school children (two to five yearsof age) in the rural district of Gondar, Ethiopia. 64 Pre-school children(n = 161) were r<strong>and</strong>omly selected from 220 households. Outof this cohort, 25 children were r<strong>and</strong>omly assigned to each of twotreatment groups: One received retinyl palmitate by inhalationof two puffs of an aerosol containing 1 mg (3,000 IU) per deliveryto give a total of 2 mg (6,000 IU); <strong>and</strong> the other received anaerosol without retinyl palmitate. Both treatments were administeredevery two weeks for three months. Serum retinol <strong>and</strong> RBPconcentrations in the group treated with vitamin A were 0.68(SD 0.31) μmol/L <strong>and</strong> 59.4 (SD 24.2) mg/L before <strong>and</strong> 1.43 (SD0.46) μmol/L (P
26 THE IMPORTANCE OF VITAMIN Afigure 8: Retinol <strong>and</strong> RBP in plasma before <strong>and</strong> after inhalation of retinyl palmitate (Biesalski et al., 1999) 6422Normal range RBPRetinol [μmol/L]1Normal range RetinolRBP [μmol/L]10Pre-inhalationPost-inhalation0Pre-inh.Post-inhalationWhole population (n =161)Study group (n =25)Placebo group (n =25)Study groupPlacebo groupInhalation of vitamin A improves vitamin A status in Ethiopian children with severe fat malabsorptionmay serve as an alternative method for vitamin A therapy duringchronic or acute episodes of malnutrition, malabsorption or inthe case of insufficient compliance with other therapies, <strong>and</strong> itmight be useful in treating respiratory diseases associated withvitamin A deficiency.“Delivery of retinyl palmitate byinhalation is effective in improvingvitamin A status”It should be investigated to what extent the “topical” applicationof retinyl esters on the respiratory epithelium, especiallyin those with chronic lung disease of prematurity, can contributeto the replenishment of lung stores <strong>and</strong> thus lead to an improvedclinical outcome.ConclusionThe results cited show that retinyl esters in respiratory epithelium<strong>and</strong> in alveolar cells form a pool of vitamin A, which can beused physiologically by the tissue. The formation of retinol <strong>and</strong>,subsequently, retinoic acid from retinyl esters is strictly controlled.So far, unphysiological formation of retinoic acid <strong>and</strong> subsequenttoxicity do not seem possible. Retinyl esters, however, arebiochemically inert with respect to gene expression or vitamin Aactivity as long as they are not hydrolyzed. Consequently, inhalativeapplication, especially in cases of insufficient lung development,could represent a true alternative. Oral administration ishardly successful because of poor RBP synthesis by the liver, <strong>and</strong>a parenteral solution is currently not available.To ensure sufficient ante- <strong>and</strong> postnatal lung maturation, acontinuous adequate supply of vitamin A is important before<strong>and</strong> during pregnancy. The vicious cycle of poor vitamin A statusin pregnancy <strong>and</strong> the consequently poor status of the newborn<strong>and</strong> the consequences for further development including adulthood<strong>and</strong> pregnancy needs to be interrupted. If no fortified foodwith preformed vitamin A is available, -carotene sources eitherfrom green leafy vegetables <strong>and</strong> fruit or biofortified food (e.g.maize, sweet potatoes) represent an alternative to improve thevitamin A supply. In cases of an “emergency” approach, supplementswith high doses either before pregnancy or in the finalterm may be useful, but data are inconsistent. A future approachwhich might help to overcome poor vitamin A status with impairedlung function is the inhalation of retinyl esters.Despite conflicting results from intervention studies, due todifferent study protocols <strong>and</strong> dosages, there can be no doubt thatthe adequate vitamin A statuses of mother <strong>and</strong> newborn have agreat impact on outcome <strong>and</strong>, in particular, the lung function ofthe newborn <strong>and</strong> the mortality <strong>and</strong> morbidity of both mother <strong>and</strong>child. It is therefore of great importance to harmonize differentsupplementation protocols to develop useful <strong>and</strong> effective recommendationsfor vitamin A delivery at the different stages ofpregnancy, as well as the antenatal <strong>and</strong> postnatal periods.
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 2727Correspondence: Hans-Konrad Biesalski, University ofHohenheim, Institute 140, Fruwirthstrasse 12, 70593 Stuttgart,Germany E-mail: biesal@uni-hohenheim.deReferences01. Kurokowa R, DiRenzo J, Boehm M et al. Regulation of retinoidsignalling by receptor polarity <strong>and</strong> allosteric control of lig<strong>and</strong>binding. Nature 1994; 371:528–531.02. Morree DM: Intracellular actions of vitamin A. In Jeon KW, ed.Friedl<strong>and</strong>er: International review of cytology. San Diego:Academic Press, 1992; 1–31.03. Pinnock CB, Douglas RM, Badcock NR. Vitamin a status in childrenwho are prone to respiratory tract infections. Aust Paediatr J 1986;22:95–99.04. Sommer A. Vitamin A supplementation <strong>and</strong> childhood morbidity.Lancet 1993; 342:1420–1224.05. West KP, Pokhrel RP, Katz J et al. Efficacy of vitamin A in reducingpreschool child mortality in Nepal. Lancet 1991; 338:67–71.06. Zachman RD. Retinol (vitamin A) <strong>and</strong> the neonate: specialproblems of the human premature infant. Am J Clin Nutr 1989;50:413–424.07. Metzler MD, Snyder JM. Retinoic acid differentially regulatesexpression of surfactant-associated proteins in human fetal lung.Endocrinology 1993; 133:1990–1998.08. Weaver TE, Whitsett JA. Function <strong>and</strong> regulation of expressionof pulmonary surfactant-associated proteins. Biochem J 1991;273:249–264.09. Odom MJ, Snyder JM, Boggaram V. Glucocorticoid regulationof the major surfactant associated protein (SP-A) <strong>and</strong> itsmessenger ribonucleic acid <strong>and</strong> of morphological development ofhuman fetal lung in vitro. Endocrinology 1988; 123:1712–1720.10. Allred TF, Mercer RR, Thomas RF et al. Brief 95% O2 exposureeffects on surfactant protein <strong>and</strong> mRNA in rat alveolar <strong>and</strong>bronchiolar epithelium. Am J Physiol. 1999;276:L999–L100911. Sundell HW, Gray ME, Serenius FS et al. Effects of epidermalgrowth factor on lung maturation in fetal lambs.Am J Pathol 1980; 100:707–725.12. Oberg KC, Carpenter G. EGF-induced PGE2 release is synergisticallyenhanced in retinoic acid treated fetal rat lung cells. BiochemBiophys Res Commun. 1989 ;162(3):1515–2113. Maden M, Hind M. Retinoic acid in alveolar development,maintenance <strong>and</strong> regeneration. Philos Trans R Soc Lond B Biol Sci.2004; 29;359:799–808.14. Bl<strong>and</strong> RD, Albertine KH, Pierce RA et al. Impaired alveolardevelopment <strong>and</strong> abnormal lung elastin in preterm lambs withchronic lung injury: potential benefits of retinol treatment. BiolNeonate. 2003;84:101–2.15. Geevarghese SK, Chytil F. Depletion of retinyl esters in the lungscoincides with lung prenatal morphological maturation. BiochemBiophys Res Commun 1994; 200:529–535.16. Massaro D, Massaro GD. Toward therapeutic pulmonary alveolarregeneration in humans. Proc Am Thorac Soc.3: 709-712 200617. Massaro D, Massaro GD. Lung development, lung function, <strong>and</strong>retinoids. N Engl J Med. 2010; 362(19):1829-31 (8):709-1218. Checkley W, West KP Jr, Wise RA et al. Maternal vitamin Asupplementation <strong>and</strong> lung function in offspring. N Engl J Med.2010;362:1784–9419. Grune T, Lietz G, Palou A et al. Beta-carotene is an importantvitamin A source for humans. J Nutr. 2010 Dec;140(12):2268S–2285S.20. Leung WC, Hessel S, Méplan C et al. Two common singlenucleotide polymorphisms in the gene encoding beta-carotene15,15'-monoxygenase alter beta-carotene metabolism in femalevolunteers. FASEB J. 2009;23(4):1041–521. Shenai JP., Chytil F. Vitamin A stores in the lungs during perinataldevelopment in the rat. Biol. Neonate. 1990; 57: 126–13222. Biesalski HK. Separation of retinyl esters <strong>and</strong> their geometricisomers by isocratic adsorption high-performance liquidchromatography. Methods Enzymol. 1990;189:181–9.23. Dirami G, Massaro GD, Clerch LB et al. Lung retinol storing cellssynthesize <strong>and</strong> secrete retinoic acid, an inducer of alveolus formation.Am J Physiol Lung Cell Mol Physiol. 2004;286(2):L249–5624. Isakson BE, Lubman RL, Seedorf GJ et al. Modulation of pulmonaryalveolar type II cell phenotype <strong>and</strong> communication by extracellularmatrix <strong>and</strong> KGF. Am.J.Cell.Physiol. 2001; 281: C1291–C129925. Gottesman ME, Quadro L, Blaner WS. Studies of vitamin A metabolismin mouse model systems. Bioessays 2001; 23: 409–41926. Blomhoff R, Green RH, Berg T et al. Transport <strong>and</strong> storage of vitaminA. Science 1990; 250:399–40427. Theodosiou M., Laudet V, Schubert M. From Carrot to clinic:an overview of the retinoic acid signaling pathway. Cell Mol <strong>Life</strong> Sci.2010; 67:1423–144528. Ross AC, Ambalavanan N. Retinoic acid combined with vitaminA synergizes to increase retinyl ester storage in the lungs ofnewborn <strong>and</strong> dexamethasone-treated neonatal rats. Neonatology.2007;92:26–32.29. Ambalavanan N, Tyson JE, Kennedy KA et al. National Institute ofChild Health <strong>and</strong> Human Development Neonatal Research Network.Vitamin A supplementation for extremely low birth weight infants:outcome at 18 to 22 months. Pediatrics. 2005;115:249–54.⇢
28 THE IMPORTANCE OF VITAMIN A30. Mupanemunda RH, Lee DSC, Fraher LJ et al. Postnatal changes inserum retinol status in very low birth weight infants. Early HumDev 1994; 38:45–54.31. Shah RS, Rajalekshmi R. Vitamin A status of the newborn inrelation to gestational age, body weight, <strong>and</strong> maternal nutritionalstatus. Am J Clin Nutr 1984; 40:794–800.32. Shenai JP, Chytil F, Jhaveri A et al. Plasma vitamin A <strong>and</strong> retinolbindingprotein in premature <strong>and</strong> term neonates. J Pediatr 1981;99:302–305.33. Shenai JP, Kennedy KA, Chytil F et al. Clinical trial of vitamin Asupplementation in infants susceptible to bronchopulmonarydysplasia. J Pediatr 1987; 111:269–277.34. Shenai JP, Rush MG, Stahlman MT et al Plasma retinol-bindingprotein response to vitamin A administration in infants susceptibleto bronchopulmonary dysplasia. J Pediatr 1990; 116:607–614.35. Boerman MH, Napoli JL. Cholate-independent retinyl ester hydrolysis.Stimulation by Apo-cellular retinol-binding protein. J BiolChem. 1991 Nov 25;266(33):22273–836. Ross AC, Zolfaghari R. Regulation of hepatic retinol metabolism:perspectives from studies on vitamin A status. J Nutr. 2004Jan;134(1):269S–275S37. McGowan SE, Harvey CS, Jackson SK. Retinoids, retinoic acidreceptors, <strong>and</strong> cytoplasmic retinoid binding proteins in perinatalrat lung fibroblasts. Am J Physiol. 1995 Oct;269(4 Pt 1):L463–738. Masuyama H, Hiramatsu Y, Kudo T. Effect of retinoids on fetal lungdevelopment in the rat. Biol Neonate. 1995;67(4):264–7339. Hind M, Corcoran J, Maden M. Temporal/spatial expression ofretinoid binding proteins <strong>and</strong> RAR isoforms in the postnatal lung.Am J Physiol Lung Cell Mol Physiol. 2002 Mar;282(3):L468–7640. Kurie JM, Lotan R, Lee JJ et al. Treatment of former smokerswith 9-cis-retinoic acid reverses loss of retinoic acid receptor-betaexpression in the bronchial epithelium: results from ar<strong>and</strong>omized placebo-controlled trial. J Natl Cancer Inst. 2003 Feb5;95(3):206–1441. Stofft E, Biesalski HK, Zschaebitz A et al. Morphological changesin the tracheal epithelium of guinea pigs in conditions of “marginal”vitamin A deficiency. Int J Nutr Res 1992; 62:134–142.42. Radhika MS, Bhaskaram P, Balakrishna N et al. Effects of vitaminA deficiency during pregnancy on maternal <strong>and</strong> child health. BJOG.2002 Jun;109(6):689–9343. Shenai JP, Chytil F, Stahlman MT. Liver vitamin A reserves of verylow birth weight neonates. Pediatr Res 1985; 19:892–893.44. Shah S, Rajalakshmi R. Vitamin A status of the newborn in relationto gestational age, body weight, <strong>and</strong> maternal nutritional status.Am. J. Clin Nutr 1984; 40: 794–800.45. Coutsoudis A, Adhikari M, Coovadia HM. Serum vitamin A(retinol) concentrations <strong>and</strong> association with respiratory disease inpremature infants. J Trop Pediatr. 1995;41(4):230–346. Filteau SM, Morris SS, Abbott RA et al. Influence of morbidity onserum retinol of children in a community-based study in northernGhana. Am J Clin Nutr 1993; 58:192–197.47. Neuzil KM, Gruber WC, Chytil F et al. Serum vitamin A levels inrespiratory syncytial virus infection. J Pediatr 1994; 124:433–436.48. Agarwal DK, Singh SV, Gupta V et al. Vitamin A status in earlychildhood diarrhoea, respiratory infection <strong>and</strong> in maternal <strong>and</strong>cord blood. J Trop Pediatr. 1996;42:12–449. Pinnock CB, Douglas RM, Badcock NR. Vitamin a status in childrenwho are prone to respiratory tract infections. Aust Paediatr J 1986;22:95–99.50. Schulz C, Engel U, Kreienberg R et al. Vitamin A <strong>and</strong> beta-carotenesupply of women with gemini or short birth intervals: a pilot study.Eur J Nutr. 2007;46:12–20.51. Godel JC, Basu TK, Pabst HF et al. Perinatal vitamin A (retinol)status of northern Canadian mothers <strong>and</strong> their infants. Biol Neonate.1996;69(3):133–952. Gerlach T, Biesalski HK, Weiser H et al. Vitamin A in parenteralnutrition: uptake <strong>and</strong> distribution of retinyl esters after intravenousapplication. Am J Clin Nutr. 1989 Nov;50(5):1029–3853. Pearson E, Bose C, Snidow T et al. Trial of vitamin A supplementationin very low birth weight infants at risk for bronchopulmonarydysplasia. J Pediatr 1992, 121:420–427.54. Barreto MI, Santos IMP, Assis AMO et al. Effect of vitamin Asupplementation on diarrhoea <strong>and</strong> acute lower-respiratory-tractinfections in young children in Brazil. Lancet 1994;344:228–231.55. Italian Collaborative Group on Preterm Delivery (ICGPD). Supplementation<strong>and</strong> plasma levels of vitamin A premature newbornsat risk for chronic lung disease. Dev Pharmacol Ther 1993;20:144–151.56. Ambalavanan N, Wu TJ, Tyson JE et al. A comparison of threevitamin A dosing regimens in extremely-low-birth-weight infants.J Pediatr. 2003;142:656–6157. Hale TW, Rais-Bahrami K, Montgomery DL et al. Vitamin E toxicityin neonatal piglets. J Toxicol Clin Toxicol. 1995;33(2):123–358. Ross AC, Ambalavanan N, Zolfaghari R et al. Vitamin A combinedwith retinoic acid increases retinol uptake <strong>and</strong> lung retinyl esterformation in a synergistic manner in neonatal rats. J Lipid Res.2006;47:1844–51.59. Ross AC. Retinoid production <strong>and</strong> catabolism: role of diet inregulating retinol esterification <strong>and</strong> retinoic acid oxidation.J Nutr. 2003;133:291S–296S.60. James ML, Ross AC, Bulger A et al. Vitamin A <strong>and</strong> retinoic acid actsynergistically to increase lung retinyl esters during normoxia <strong>and</strong>reduce hyperoxic lung injury in newborn mice. Pediatr Res. 2010Jun;67(6):591–761. Biesalski HK, Frank J, Beck SC et al. Biochemical but not clinicalvitamin A deficiency results from mutations in the gene for retinolbinding protein. Am J Clin Nutr. 1999;69:931–6. Erratum in:Am J Clin Nutr 2000;71(4):101062. Biesalski HK, Nohr D. New aspects in vitamin a metabolism: therole of retinyl esters as systemic <strong>and</strong> local sources for retinol in
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE IMPORTANCE OF VITAMIN A 2929mucous epithelia. J Nutr 2004 Dec;134(12 Suppl):3453S–3457S.63. Biesalski HK. Effects of intra-tracheal application of vitamin A onconcentrations of retinol derivatives in plasma, lungs <strong>and</strong> selectedtissues of rats. Int J Vitam Nutr Res. 1996;66(2):106–1264. Biesalski H, Reifen R, Fürst P et al. Retinyl palmitate supplementationby inhalation of an aerosol improves vitamin A status ofpreschool children in Gondar (Ethiopia). Br J Nutr. 1999;82:179–8265. Kohlhäufl M, Häussinger K, Stanzel F et al. Inhalation of aerosolizedvitamin a: reversibility of metaplasia <strong>and</strong> dysplasia of humanrespiratory epithelia -- a prospective pilot study. Eur J Med Res.2002 Feb 21;7(2):72–866. Singh AJ, Bronshtein V, Khashu M et al. Vitamin A is systemicallybioavailable after intratracheal administration with surfactant inan animal model of newborn respiratory distress. Pediatr Res. 2010Jun;67(6):6167. Ross AC., Ambalavanan N. Retinoic acid combined with vitamin Asynergizes to increase retinyl ester storage in the lungs of newborn<strong>and</strong> dexamethasone-treated neonatal rats. Neonatology 2007; 92:26–3268. Wu L, Ross AC. Acidic retinoids synergize with vitamin A to enhanceretinol uptake <strong>and</strong> STRA6, LRAT, <strong>and</strong> CYP26B1 expression inneonatal lung. J.Lipid.Res. 2010 51:378–38769. Ong DE, Chytil F. Changes in levels of cellular retinol- <strong>and</strong> retinoicacid-bindingproteins of liver <strong>and</strong> lung during perinatal developmentof rat. PNAS 1976; 73: 3976-78
30THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNSTesting the Feasibilityof Delivering Vitamin Ato Newborns in Nepal<strong>and</strong> BangladeshRolf DW KlemmCenter for Human Nutrition, Bloomberg, School ofPublic Health, Johns Hopkins University <strong>and</strong> A2Z:The USAID Micronutrient <strong>and</strong> Child Blindness ProjectRaj Kumar Pokharel, R P BichhaMinistry of Health <strong>and</strong> Population, NepalBackgroundInfants are born with small livers <strong>and</strong> total body stores of vitaminA (VA). 1–5 Exclusively breastfed infants depend on adequatebreastfeeding <strong>and</strong> good health to build body stores. 6However, low breast milk vitamin A, inadequate breast milk intakeconcentration, 5–8 poor complementary food quality 9 <strong>and</strong>/orfrequent infection 10 can all reduce an infant’s ability to achievenormal vitamin A status.Makhduma NargisRevitalization of Community Health CareInitiative/Community Clinic, Ministry of Health <strong>and</strong>Family Welfare, BangladeshZeba MahmudMicronutrient Initiative, BangladeshLesley OotA2Z: The USAID Micronutrient <strong>and</strong> Child BlindnessProject, AED, Washington, DC, USAPankaj Mehta, Naveen Paudyal UNICEF, NepalJaganath Sharma NFHP II/USAID, NepalM R Maharjan, Neera SharmaMicronutrient Initiative, NepalMahbubur Rashid The JiVitA Project,Gaidb<strong>and</strong>ha, BangladeshA promising new interventionNewborn vitamin A supplementation (NVAS) is a promising newintervention that involves supplementing infants shortly afterbirth with a single, large oral dose of vitamin A (50,000 IU)(Figure 1). The intervention was tested in three field trials insouthern Asia (Indonesia, India, <strong>and</strong> Bangladesh), each of whichreported significant reductions of ≥ 15% in infant mortality inthe first six months of life. 11–13 When combined, the resultssuggest that infant mortality can be reduced by approximately20% in southern Asia by giving newborns a single, oral dose ofvitamin A. 14 Given previous evidence of safety with respect toshort- or long-term side effects, 15–20 newborn vitamin A supplementationappears to be a low-cost approach to reducing infantmortality in South <strong>and</strong> Southeast Asia.In Africa, however, this intervention had no beneficial effecton early infant survival in an urban setting in Zimbabwe, 21 <strong>and</strong>a peri-urban setting in Guinea Bissau. 22,23 All three African studies(two in Guinea Bissau) were done in populations with little,if any, vitamin A deficiency. Mortality in the Zimbabwean studywas very low. 21 In one study in Guinea Bissau, investigatorsreduced mortality by excluding the highest risk infants (thosewith low birth weight) <strong>and</strong> giving free care <strong>and</strong> drugs to sickinfants. 22A 2008 WHO Technical Consultation on Neonatal Vitamin ASupplementation Research Priorities 24 made the following
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>31“Insuffi cient evidence existsto recommend a global policy ofsupplementing newborns withvitamin A.”figure 1: Female community health volunteer (FCHV)dosing newborn with vitamin A in Nepal
32 THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNSFigure 2: Map of NVAS pilot districts in NepalNVAS pilot districtsFar-WesternRegionBankeIndiaMid-WesternRegion0 20 60 100 KilometersWestern RegionNawalparasiTanahuCentral RegionFCHV dosing modelMother dosing modelSindhuliEastern Regionrecommendation: “Operational research on how to reach mostbabies in developing countries within two days of birth shouldbe conducted in general, not necessarily in the context of neonatalvitamin A supplementation.” The consultation also revieweda systematic review of neonatal vitamin A trials. 25 It concludedthat insufficient evidence existed to recommend a global policyof supplementing newborns with vitamin A until further efficacytrials in appropriate populations are conducted in Africa <strong>and</strong>Asia. WHO is currently supporting additional efficacy studies inAfrica (Tanzania <strong>and</strong> Ghana) <strong>and</strong> South Asia (India), as well asstudies investigating potential biological mechanisms throughwhich NVAS may decrease the risk of early infant mortality.Program implicationsAdequate <strong>and</strong> effective NVAS will require innovative but feasibleprograms in South Asian settings, where often >80% of infantsare born at home. For example, newborn dosing might requireidentifying <strong>and</strong> engaging neighborhood “watch” networks todetect births <strong>and</strong> rapidly dose infants, or using cell phones tocontact health workers at the time of birth. The capsule wouldneed to be widely available, perhaps through both the private<strong>and</strong> public sectors. It could be included as a new component in“safe birthing kits” for women to use themselves (obtained duringantenatal care or purchased in local shops), provided at thetime of home-delivery by nurse midwives or trained traditionalbirth attendants or, lastly, at clinic- or hospital-based obstetriccare <strong>and</strong> delivery programs. Newborn VA delivery could be combinedwith other emerging <strong>and</strong> effective neonatal care services,such as cord cleaning with chlorahexadine wipes 26 <strong>and</strong> newborncare intervention packages. 27 It could provide an opportunityto establish birth dates <strong>and</strong> set the timing for an infant’s “sixmonth”VA-dosing visit – an idea that is currently gaining interest.Alternatively, in contexts where a high proportion of womenattend antenatal clinics, women could be given the supplement<strong>and</strong> instructed on its use <strong>and</strong> administration, <strong>and</strong> then give itdirectly to their newborn shortly after birth.NVAS feasibility activities purposeIn both Nepal <strong>and</strong> Bangladesh, NVAS feasibility activities wereto identify, develop, <strong>and</strong> evaluate feasible models for deliveringNVAS integrated within existing ante- <strong>and</strong> postnatal interventionsat a scalable level within existing delivery platforms <strong>and</strong>government health services.NepalBackground. Nepal is on track to meet its Millennium DevelopmentGoal (MDG)-4 to reduce under-five mortality by two-thirds;however, the government is finding ways to make further reductionsby seeking efficacious interventions that reduce neonatal<strong>and</strong> early infant deaths. The Child Health Division, Departmentof Health Services of the Nepal Ministry of Health <strong>and</strong> Populationformulated a policy to pilot first, <strong>and</strong> piloted NVAS in 2009in four districts (Figure 2), in partnership with the USAID-fundedNepal Family Health Program-II (NFHP-II), UNICEF, <strong>and</strong> theMicronutrient Initiative (MI).Delivery models. Considering that ~80% of births in Nepaloccur in the home, the extensive network of female communityhealth volunteers (FCHVs), <strong>and</strong> the government’s effortsto intensify <strong>and</strong> improve access to Antenatal Care services,Nepal selected two distribution models for feasibility testing:1. The “FCHV Dosing” model, using postnatal home visits byfemale community health volunteers to administer vitamin Adirectly to newborns in two districts (Banke <strong>and</strong> Nawalparasi)(Figure 3); <strong>and</strong>2. The “Mother / Family Member Dosing” model, in which motherswho attend an antenatal clinic at a health facility (HF), or arevisited at home by the FCHV after the eighth month of pregnancy,are counseled about NVAS <strong>and</strong> given a supplement which theygive directly to their newborn, also in two districts (Sindhuli <strong>and</strong>Tanahu) (Figure 4).Monitoring <strong>and</strong> evaluation. NVAS implementation is beingmonitored through the routine government health management<strong>and</strong> information system. To record information on NVASreceipt, the existing Iron Intensification Register, a record usedto track iron <strong>and</strong> folic acid tablet receipt among pregnant <strong>and</strong>postpartum mothers, was modified. Data from this record arecompiled <strong>and</strong> sent monthly to the district <strong>and</strong> national levels.In addition, three to four external monitors per district provide
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNS 3333figure 3: FCHV Dosing ModelAntenatal contactwith pregnant womenIron distribution by FCHVspecial technical support visits, <strong>and</strong> interview health workers<strong>and</strong> mothers whose babies have received the VA. In addition, theeffectiveness of the intervention is being evaluated using twopopulation-based cross-sectional surveys at baseline (September2009) <strong>and</strong> end-line (February <strong>2011</strong>).FCHV notified at birth byfamilyFHCV visits newborn’shome within 48 hoursof birthFCHV doses newbornwith vitamin A <strong>and</strong>recordsfigure 4: Mother Dosing ModelANC visitHFOutreachclinicFCHV visitwithin48 hours ofdeliveryAntenatal contactwith pregnantwomenNVAS dispensingto pregnant womenat 8 months ofpregnancy by HFstaff or FCHVNVAS dosing within48 hours of deliveryby mothers/familymembersConfirmationof newborn dosing<strong>and</strong> dosing if missed<strong>and</strong> recordingDelivery at healthinstitutionNewborn dosed withvitamin A within 48 hoursof birthPostnatal visit by FCHV toconfirm if dosed at HFIrondistributionby FCHV <strong>and</strong>counselingNVASDelivery athealthinstitutionNewborndosed withvitamin APreliminary findings. Through the initial nine months of implementationin the four pilot districts, >18,000 newborns havebeen supplemented. Preliminary findings suggest that 62% ofnewborns are reached in the female community health volunteer(FCHV) <strong>and</strong> community health worker dosing model, <strong>and</strong> only45% in the mother/family member dosing model.Interesting preliminary observations frommonitoring surveys include:> High NVAS coverage in districts where institutional deliveriesare high, <strong>and</strong> where other community-based services targetingnewborns have been well established (e.g. in Banke).> Low ANC attendance, especially the last visit at eight months’gestation, appears to lead to low NVAS coverage.> In the “Mother/Family Member Dosing” model, ~11% of mothersare reluctant to dose their newborns. Instead, they waitfor the community health worker (i.e. the FCHV) to visit <strong>and</strong>dose the newborn.> Fewer than one percent of mothers <strong>and</strong> about one percent ofhealth workers reported a bulging fontanel in dosed infants.All cases were transitory <strong>and</strong> recovered without treatment.BangladeshBackground. The Ministry of Health <strong>and</strong> Family Welfare (Mo-HFW) in Bangladesh has extensive experience in consideringresearch findings, establishing a permissive policy, pilotingmodels to test implementation feasibility, <strong>and</strong> scaling up interventions.In December 2009, the Government of Bangladesh approvedpilot feasibility testing activities for NVAS in three districts(Tangail, Pirojpur <strong>and</strong> Nilphamari), <strong>and</strong> six sub-districtsdivided between the Directorate General of Family Planning <strong>and</strong>Revitalization of Community Health Care Initiative/CommunityClinic, Bangladesh (Figure 5).Delivery models. In Bangladesh >80% of births occur in thehome,
34 THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNSfigure 5: Map of districts in Bangladesh whereNVAS is being pilotedNilphamariJaldhaka<strong>and</strong> DimlaupazilasIndia(WestBengal)PirojpurSadar <strong>and</strong>Nesarabadupazilas0 25 50 KilometersTangailJaldhaka<strong>and</strong> DimlaupazilasIndia(Assam)India(Tripura)Myanmar(Burma)<strong>and</strong> home- or clinic-based antenatal (ANC) visits (Figure 7). Inaddition to key ANC services <strong>and</strong> messages, pregnant womenreceive an individually packaged dose of vitamin A (50,000 IU),<strong>and</strong> are instructed about why, when, <strong>and</strong> how to administer thedose to their newborns, <strong>and</strong> how to manage potential side effects.This information is accompanied by a counseling card<strong>and</strong> a “Health Worker Contact Card” that includes the name,cell phone number, <strong>and</strong> address of the local health worker. Thepotential advantage of this model is that the VA supplement isin the home at the time of delivery, <strong>and</strong> does not require thenotification of or waiting for the arrival of a health worker toadminister the dose.2. The “Health Worker Dosing” model also uses FWAs <strong>and</strong> HAs;however, the mother or a family member must contact the healthworker at the time of birth <strong>and</strong> the health worker must visit themother <strong>and</strong> her newborn to directly administer the vitamin A(Figure 8). To facilitate birth notification, health workers informpregnant mothers about the importance of early birth notificationso that the baby can obtain newborn vitamin A <strong>and</strong> otheressential newborn services. In this model, a “Health WorkerContact Card” is also provided to promote prompt <strong>and</strong> directcommunication with the health worker.Monitoring <strong>and</strong> evaluation. Monitoring the pilot activitiesinvolves a two-pronged strategy consisting of (1) routine datacollection within the MoHFW system; <strong>and</strong> (2) special monitoringinterviews <strong>and</strong> observations conducted by locally hired“extenders” to assess how well NVAS is being integrated intoexisting ANC <strong>and</strong> postpartum visits, <strong>and</strong> to assess communityacceptability (Figure 9). Two cross-sectional surveys in eachprogram upazila, or region, at baseline <strong>and</strong> at six months afterimplementation (i.e. end-line), will be conducted among recentlydelivered mothers to assess coverage <strong>and</strong> timeliness of thedelivery of newborn vitamin A. In addition, community healthworkers (CHW) will be surveyed at baseline <strong>and</strong> end-line toassess knowledge, attitudes, <strong>and</strong> practices about integratingNVAS into existing services.figure 6: NVAS design workshop participantsin Bangladeshdesign workshop, including national, district <strong>and</strong> sub-districtlevel health <strong>and</strong> family planning managers, was held in October2010 (Figure 6) <strong>and</strong> proposed two delivery platforms:1. The “Mother / Family Member Dosing” model in Bangladeshuses two cadres of community health workers: The “Female WelfareAssistant” (FWA) <strong>and</strong> the “Health Assistant” (HA), who integratesNVAS into routine home-based pregnancy surveillanceConclusionsBoth Nepal <strong>and</strong> Bangladesh have made important strides in bridgingthe research-to-program gap by examining scientific evidence<strong>and</strong> its relevance within each country’s context, establishingpolicies that permit feasibility testing of this new intervention,<strong>and</strong> closely monitoring <strong>and</strong> evaluating NVAS implementationbefore formulating a policy for national scale-up. From preliminarydata, implementation challenges facing NVAS are similar tothose faced by other interventions that target pregnant women<strong>and</strong> newborns. These include identifying <strong>and</strong> reaching a highproportion of pregnant women <strong>and</strong> their newborns in a timelymanner, overcoming geographic, travel <strong>and</strong> time constraints
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNS 3535figure 7: Mother/Family Dosing ModelPregnancyContact Points> Home-based pregnancyidentification/registration> Home-based ANC visit> Satellite-clinic ANC visit> FWC-based ANCActionsAntenatal contact with pregnant womenPregnant women given NVAS <strong>and</strong> instructedon why, what, when, how <strong>and</strong> who will give NVAS(integrated into usual ANC services/counseling)BirthPhone callActionsMother or family members gives NVAS tonewborn within 2 days of birthPostpartum (0–2 days after birth)Contact Points> Postnatal home visit by FWAor HAActionsFWA or HA confirms newborndosing <strong>and</strong> doses baby if missedfigure 8: Health Worker Dosing ModelPregnancyContact Points> Home-based pregnancyidentification/registration> Home-based ANC visit> Satellite-clinic ANC visit> FWC-based ANCActionsAntenatal contact with pregnant womenPregnant women given NVAS <strong>and</strong> instructedon why, what, when, how <strong>and</strong> who will give NVAS(integrated into usual ANC services/counseling)BirthPhone callBaby is born,please come!ActionsFamily member contacts health worker bymobile phone or drops card at clinicPostpartum (0–2 days after birth)Contact Points> Postnatal home visit by FWAor HAActionsHealth worker directly doses newborn
36 THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNSfigure 9: Monitoring <strong>and</strong> evaluation of NVAS pilot activities in BangladeshFormative research, advocacy, planning,training, communications, logisticsDistrict Level Programm (CC, FP)Recentlydeliveredwomen <strong>and</strong>communityhealthworkersBaselineNBVAS ImplementationPerformance MonitoringRoutine (through MoHFW) <strong>and</strong> special monitoringconducted by externally hired “extenders”Recently deliveredwomen <strong>and</strong>community healthworkersEndlineUpazila 1NBVAS-Mother/Family Member ModelUpazila 2NBVAS-CHW ModelDec. ‘10Jan. ‘11Feb. ‘11March ‘11April ‘11May ‘11June ‘11July ‘11in reaching a health facility or a home, <strong>and</strong> tracking pregnantwomen who travel to their parental home to give birth. Lessonslearned from these pilot activities will provide useful insightson how to introduce <strong>and</strong> integrate this new intervention withinexisting health systems <strong>and</strong> delivery platforms in South Asia.Correspondence: Rolf DW Klemm, A2Z: The USAIDMicronutrient <strong>and</strong> Child Blindness Project, AED, 1825 ConnecticutAvenue, NW, Washington, DC 20009, USAE-mail: rklemm@jhsph.eduReferences01. Dahro M, Gunning D, Olson JA. Variations in liver concentrationsof iron <strong>and</strong> vitamin A as a function of age in young Americanchildren dying of the sudden infant death syndrome as well as ofother causes. Int J Vitam Nutr Res 1983;5302. Gebre-Medhin M, Vahlquist A. Vitamin A nutrition in the humanfetus. A comparison of Sweden <strong>and</strong> Ethiopia. Acta Paediatr Sc<strong>and</strong>1984;73:333–40.03. Montreewasuwat N, Olson JA. Serum <strong>and</strong> liver concentrationsof vitamin A in Thai fetuses as a function of gestational age.Am J Clin Nutr 1979 Mar;32(3):601–6.04. Shah RS, Raalakshmi R, Bhatt RV et al. Liver stores of vitamin Ain human fetuses in relation to gestational age, fetal size <strong>and</strong>maternal nutritional status. Br J Nutr 1987;58:181–905. West KP, Jr. Public health impact of preventing vitamin Adeficiency in the first six months of life. In: Delange FM, West KP Jr,eds. Micronutrient Deficiencies in the First Months of <strong>Life</strong>. Vevey,Switzerl<strong>and</strong>: Karger; 2003;103–28.06. Haskell MJ, Brown KH. Maternal vitamin A nutriture <strong>and</strong> thevitamin A content of human milk. J Mammary Gl<strong>and</strong> BiolNeoplasia 1999;4(3):243–5707. Rice AL, Stoltzfus RJ, de Francisco A et al. Low breast milk vitamin Aconcentration reflects an increased risk of low liver vitamin A storesin women. Adv Exp Med Biol 2000;478:375–6.08. Stoltzfus RJ, Humphrey JH. Vitamin A <strong>and</strong> the nursing motherinfantdyad: evidence for intervention. Adv Exp Med Biol2002;503:39–47.09. Kimmons JE, Dewey KG, Haque E et al. Low nutrient intakesamong infants in rural Bangladesh are attributable to low intake<strong>and</strong> micronutrient density of complementary foods. J Nutr 2005Mar;135(3):444–51.10. Mitra AK, Wahed MA, Chowdhury AK et al. Urinary retinol excretionin children with acute watery diarrhoea. J Health Popul Nutr2002;20(1):12–7.11. Humphrey JH, Agoestina T, Wu L et al. Impact of neonatal vitaminA supplementation on infant morbidity <strong>and</strong> mortality. J Pediatr1996;128:489–96.12. Rahmathullah L, Tielsch JM, Thulasiraj RD et al. Impact ofsupplementing newborn infants with vitamin A on early infantmortality: community based r<strong>and</strong>omized trial in southern India.BMJ 2003;327:254.13. Klemm RD, Labrique A, Christian P et al. Newborn vitamin A supplementationreduced infant mortality in rural Bangladesh. Pediatrics,2008:122;E242–E25014. West KP, Jr. Newborn vitamin A dosing: Policy implications for Asia<strong>and</strong> Africa. Micronutrient Forum Abstracts, Istanbul, Turkey, 16–18April 2007.15. Agoestina T, Humphrey JH, Taylor GA et al. Safety of one 52-μmol(50,000 IU) oral dose of vitamin A administered to neonates. BullWorld Health Organ. 1994;72(6):859–68.16. Humphrey JH, Agoestina T, Juliana A et al. Neonatal vitamin Asupplementation: Effect on development <strong>and</strong> growth at 3 y of age.Am J Clin Nutr 1998;68(1):109–17.17. Baqui AH, de Francisco A, Arifeen SE et al. Bulging fontanelle aftersupplementation with 25,000 IU of vitamin A in infancy using
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNS 3737immunization contacts. Acta Paediatr 1995;84(8):863–6.18. Iliff et al. Nutr Res 1999;19:437.19. West KP Jr, Khatry SK, LeClerq SC et al. Tolerance of young infants toa single, large dose of vitamin A: a r<strong>and</strong>omized community trial inNepal. Bull World Health Organ 1992;70(6):733–9.20. WHO/CHD. R<strong>and</strong>omized trial to assess benefits <strong>and</strong> safety ofvitamin A supplementation linked to immunization in early infancy.WHO/CHD immunization-linked vitamin A supplementation studygroup. Lancet 1998;352:1257–63.1 Malaba LC, Iliff PJ, Nathoo KH et al. Effect of post-partum maternalor neonatal vitamin A supplementation on infant mortality amonginfants born to HIV-negative mothers in Zimbabwe. Am J Clin Nutr2005;81:454–60.21. Benn CS, Diness BR, Roth A et al. R<strong>and</strong>omized trial of the effect onmortality of 50,000 IU vitamin A given with BCG vaccine to infantsin Guinea-Bissau, West-Africa. BMJ 2008; 336:1416–20.22. Benn CS, Fisker AB, Napirna BM et al. Vitamin A supplementation<strong>and</strong> BCG vaccination at birth in low birthweight neonates: two bytwo factorial r<strong>and</strong>omised controlled trial. BMJ. 2010;340:c1101.23. WHO 2009 http://www.who.int/nutrition/publications/micronutrients/vitamin_a_deficieny/NVAS_report.pdf24. Gogia S, Sachdev HS. Neonatal vitamin A supplementation forprevention of mortality <strong>and</strong> morbidity in infancy: systematic reviewof r<strong>and</strong>omised controlled trials. BMJ. 2009 Mar 27;338:b91925. Tielsch JM, Darmstadt GL, Mullany LC et al. Impact of newbornskin-cleansing with chlorhexidine on neonatal mortality in southernNepal: a community-based, cluster-r<strong>and</strong>omized trial. Pediatrics.2007 Feb;119(2):e330–40.26. Baqui AH, El-Arifeen S, Darmstadt GL et al. Projahnmo Study Group.Effect of community-based newborn-care intervention packageimplemented through two service-delivery strategies in Sylhetdistrict Bangladesh: a cluster-r<strong>and</strong>omised controlled trial. Lancet.2008;371(9628):1936-44.27. National Institute of Population Research <strong>and</strong> Training (NIPORT),Mitra <strong>and</strong> Associates, <strong>and</strong> Macro International. 2009. BangladeshDemographic <strong>and</strong> Health Survey 2007. Dhaka, Bangladesh <strong>and</strong>Calverton, Maryl<strong>and</strong>, USA: National Institute of Population Research<strong>and</strong> Training, Mitra <strong>and</strong> Associates, <strong>and</strong> Macro International.Available soon !The new “Manual on Vitamin ADeficiency Disorders (VADD)” by<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Press
38FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREADiversification fromAgriculture to Nutritionally<strong>and</strong> EnvironmentallyPromotive Horticulture ina Dry-L<strong>and</strong> AreaMahtab S Bamji, PVVS MurtyDangoria Charitable Trust, Hyderabad, IndiaM Vishnuvardhan RaoNational Institute of Nutrition, Hyderabad, IndiaG SatyanarayanaANGR Agriculture University, Hyderabad, IndiaIntroductionCereal pulse-based Indian diets are qualitatively poor in vitamins<strong>and</strong> minerals due to inadequate consumption of vegetables <strong>and</strong>fruits – the major source of micronutrients in vegetarian diets. 1Homestead gardens have been reported to improve access to<strong>and</strong> consumption of vegetables. 2, 3, 4 Homestead food productionalso helps with household food security. 2, 5This study has attempted partial diversification from the water-intensivecropping pattern (rice <strong>and</strong> sugar cane) to horticultureusing green methods of farming in a dry-l<strong>and</strong> area to improvehousehold access to vegetables <strong>and</strong> environment security.Subjects <strong>and</strong> methodsThe study was conducted in 15 villages from 4 m<strong>and</strong>als (population24,000), of the Medak district of the South Indian state ofAndhra Pradesh. The project was explained in village-level meetings;222 farmers who had l<strong>and</strong> (marginal or small) <strong>and</strong> werewilling to partially diversify from rice <strong>and</strong> sugar cane to horticulture(mixed orchards, vegetable gardens), <strong>and</strong> adopt greenmethods of farming, were identified. Seeds/seedlings of micro-nutrient-rich varieties of vegetable <strong>and</strong> fruit were distributedamong the farmers identified. Drumstick, papaya, curry leaves(Murraya Koenigii) <strong>and</strong> creeper spinach (Basilla alba) seedlingswere raised by village women in backyard nurseries <strong>and</strong> thenpurchased from them, providing them with some income.Organic fertilizers, such as vermi compost, <strong>and</strong> botanicalpesticides, such as neem kernel <strong>and</strong> chili garlic decoction, werepromoted. Once every two months, experts were invited as faculty<strong>and</strong> centralized training programs were conducted on thecampus of the Dangoria Charitable Trust (DCT) in the villageof Narsapur. H<strong>and</strong>s-on training was also given via village-levelmeetings <strong>and</strong> visits to individual farms. In addition to horticulture,<strong>and</strong> the use of organic methods of farming, education in nutrition,health <strong>and</strong> environment formed an important part of thetraining. Focused group discussions (FGD) <strong>and</strong> slide <strong>and</strong> soundshows were organized in the evenings. School education wasalso an important part of creating awareness.Impact assessment was carried out by making a record ofdiverted l<strong>and</strong>, crops grown <strong>and</strong> their survival, the adoption oforganic methods of farming etc. A rough estimate of vegetablessold <strong>and</strong> consumed at home was obtained by visiting householdsevery month <strong>and</strong> making enquiries.Baseline <strong>and</strong> end-line surveys on Knowledge, Attitude, <strong>and</strong>Practice (KAP) were carried out in four villages, representing threem<strong>and</strong>als, using a pretested questionnaire to test know-ledge ongreen methods of farming <strong>and</strong> nutrition. A diet survey using asemi-quantitative method was held to examine the impact onconsumption of protective foods such as vegetables, pulses <strong>and</strong>animal products. This method involves obtaining information onthe frequency of consumption of different foods by the familyduring a typical week (when there are no guests, festivities, or
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREA3939Mixed orchards in India contribute to home food production<strong>and</strong> boost vegetable consumptionfasting), the daily quantity cooked <strong>and</strong> the number of householdmembers above the age of one year (capita).Based on this information, an estimate of mean quantity ingrams of different foods consumed per capita per day was obtained.During the end-line survey, intake per consumption unit(CU), 1 in addition to per capita intake, was also ascertained byobtaining additional information on the sex, age, physiologicalstatus <strong>and</strong> activity of different members of the family (data notreported). However, the difference between per capita <strong>and</strong> perCU values was negligible. This method of diet survey can be appliedin rural households where diets <strong>and</strong> menus are routine.The initial survey in the four selected villages included allfarmers who had agreed to participate in the project. All of thefarmers who actually participated (stakeholders) were also includedin the end-line survey (experimental group). This covered82% of the initial cohort. Some farmers who initially acceptedthen dropped out, but some who were initially unwilling joinedlater on. To allow for the impact of time, in the end-line survey50 farming households from the same villages who had not participatedin l<strong>and</strong> diversion were also interviewed (control group).However, even the control group farmers were allowed to participatein the training programs conducted in the villages. Due tomaterial <strong>and</strong> human resource constraints, the KAP survey couldnot be carried out in all 15 villages. In addition, more than 50%of the farmers who joined the project were from the four selectedvillages. The two interviewers were trained <strong>and</strong> spoke the locallanguage fluently.“Monthly inquires suggested salesof 25–50% of the vegetablesgrown, with the rest being consumedat home”
40 FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREAtable 1: Knowledge of nutrition. Values are % of respondents. No prompting. Multiple answers.DescriptionInitialMarch / April 2007End-line ExperimentalMarch / April 2010End-line ControlMarch / April 2010Number of respondents 125 128 50Why do we eat food?Good health 70.4 *** 95.3 80.0 **Gives energy 40.0 *** 76.6 64.0 **Gives strength 32.8 *** 55.5 54.0Protects against diseases 3.2 *** 63.8 24.0 *** ***For living 5.6 *** 49.6 40.0 ***For hunger 12.8 19.5 28.0 *Any other 0.8 3.3 4.0What are the components of a balanced diet ?Cereals 63.2 *** 98.4 100.0 ***Roti (dry pancakes from cereals 49.6 *** 71.1 60.0<strong>and</strong> millets)Pulses 23.2 *** 95.9 66.0 *** ***Vegetables 36.0 *** 98.4 70.0 *** ***Fruits 38.4 *** 62.2 42.0 *Green leafy vegetables 42.4 *** 81.1 38.0 ***Milk 19.2 *** 77.3 56.0 ** ***Eggs 13.6 *** 66.4 36.0 *** ***Meat/fish etc 19.2 39.8 32.0What are the functions of fruits <strong>and</strong> vegetables ?Good health 64.0 *** 85.9 76.0Gives energy 51.2 57.0 62.0Gives strength 47.2 45.7 55.1Protects against diseases 5.6 *** 69.6 22.0 *** ***Improves eyesight 4.0 *** 58.0 52.0Protects against anemia 0 75.8 34.0 *** ***Makes teeth <strong>and</strong> bones stronger 0 37.6 16.0 **For taste 0 39.1 52.0Any other 0.8 3.1 2.0The Two Proportion Z test was used to see the differences in proportions between two groups* P
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREA 4141table 2: Food consumption: Weekly frequency <strong>and</strong> quantity consumed per capita per day.DescriptionInitialEnd-line ExperimentalEnd-line ControlMarch / April 2007March / April 2010March / April 2010Number of respondents 125 128 50FoodVegetables: frequency 3.85 ± 1.04 c 3.4± 0.631 a 3.1 ± 0.340 bg /capita /day 57.7± 31.11 ac 52.3 ± 21.7 a 37.1 ± 10.34 bGLV: frequency-mean 2.2 ± 0.72 2.9 ± 0.750 2.5 ± 0.614g /capita /day 36.0 ± 20.08 c 51.6 ± 24.3 a 57.1 ± 24.4 abPulses: frequency-mean 2.63 ± 1.08 2.8 ± 0.741 2.7± 0.519g /capita /day 20.4 ± 13.03 19.0 ± 8.62 17.9 ± 5.52Milk: frequency-mean 6.76 ± 1.30 6.94 ± 0.621 7.0 ± 0.000g /capita /day 95.8 ± 138.68 c 71.3 ± 46.75 a 47.7 ± 18.78 bEggs: frequency-mean 1.3 ± 0.87 a 2.0 ± 1.458 b 1.9 ± 0.274 bcnumber / capita / day 0.15 ± 0.1199 a 0.41 ± 1.16 b 0.3 ± 0.079 bMeat: frequency-mean 1.02 ± 0.297 a 1.35 ± 0.685 b 1.64 ± 0.485 cg /capita /day 18.49 ± 8.745 a 27.8±44.62 b 27.3± 9.36 bcMeans with different superscripts a, b, c are significantly different at P
42 FROM AGRICULTURE TO HORTICULTURE IN A DRY-LAND AREAover 50% of families depended on sources outside the villagefor their household requirements. In both the surveys, over 90%of families mentioned that they ate all of the above food grains,except maize, which a third of the families did not eat despitecultivating it.“For poor households, economiccompulsions outweigh nutritionalwisdom”DiscussionDiets were poor with regard to foods such as pulses, vegetables<strong>and</strong> animal products. The marked reduction in the mean consumptionof vegetables in the control group in the end-line survey,as compared to the initial survey, demonstrates the adverseimpact of the price rise. The experimental group seems to havebeen shielded against this effect, stressing the need to promotethe homestead production of protective foods. An almost 44%increase in the consumption of GLV in the end-line, as comparedto the initial survey, suggests the positive impact of nutritioneducation. The increase, which occurred even in the controlgroup, is not surprising; growing GLV is easy <strong>and</strong> all of thesewere included in the community education efforts. Despite thefact that vegetable consumption was far below the recommendedlevel, all of the farmers mentioned that they sold 25–50% of thevegetables grown. For poor households, economic compulsionsoutweigh nutritional wisdom. Village-level security for rice wasbetter than that for other foods which had to be procured fromoutside sources. The fact that most families consumed cereals<strong>and</strong> millets other than rice suggests a healthy traditional practiceof consuming mixed-grain diets. This needs to be nurtured,particularly since, in recent years, the preference for millets hasdeclined due to easy access to rice <strong>and</strong> wheat.In earlier studies 6,7 aimed at promoting home gardens to combatvitamin A deficiency in the Medak district, it was observedthat home gardening alone may not be adequate to prevent vitaminA deficiency. Other methods, including the promotion ofanimal husb<strong>and</strong>ry <strong>and</strong> poultry, would be needed to complementthis food-based approach. In the authors’ experience, diversificationto horticulture from other crops requires considerableadvocacy <strong>and</strong> persuasion, since farmers with marginal <strong>and</strong> smalll<strong>and</strong>-holdings hesitate to diversify from traditional crops. On theother h<strong>and</strong>, acceptance of back-yard poultry was good (unpublished).In conclusionHomestead gardening can have a positive impact on the consumptionof horticultural produce, but this by itself will not meetthe daily requirements in a small-farm-holding family where incomeis a priority. Poverty alleviation measures are needed toimprove household food security.AcknowledgementsThe authors are grateful to the Department of Biotechnology,Government of India for financial support; the Dangoria CharitableTrust for logistical support, <strong>and</strong> Dr T Vishnumurthy <strong>and</strong> SriNarsimha Reddy for training in horticulture.Correspondence: Mahtab S Bamji, Dangoria Charitable TrustDCT), 1-7-1074, Musheerabad, Hyderabad 500020, IndiaE-mail: msbamji@gmail.comReferences01. National Nutrition Monitoring Bureau. Diet <strong>and</strong> nutrition statusof population <strong>and</strong> prevalence of hypertension among adults inrural areas. Technical Report No. 24, National Institute of Nutrition,Hyderabad, India, Indian Council of Medical Research, 2006.02. Talkukdar A, Haselow NJ, Osel AK et al. Homestead food productionmodel contributes to improved household food security <strong>and</strong> nutritionstatus of young children <strong>and</strong> women in poor populations. FieldActions Science Reports (online), Special Issue 1: Urban Agriculture,online since 17 February 2010, accessed 13 June 2010. http//factsreports.revues.org/index404.html.03. Rahman FMM, Mortuza MGG, Rahman MT et al. Food securitythrough homestead vegetable production in the smallholder agriculturalimprovement project (SAIP) area. J Bangladesh Agril Univ2008;6:261–69.04. Iannoti L, Cunningham K, Ruel M. Improving diet quality <strong>and</strong>micronutrient nutrition. Homestead food production in Bangladesh.IFPRI discussion paper 00928, prepared for the project on MillionsFed: Proven Successes in Agriculture Development, November2009;1–44. www.IFPRI.org/millions fed05. Ndaeyo NU. Assessing the contributions of homestead farming tofood security in a developing economy: A case study of SouthernNigeria. J Agri Soc Sci 2007;3:11–1606. Vijayraghavan K, Nayak UM, Bamji MS et al. Home gardening forcombating vitamin A deficiency in rural India. Food <strong>and</strong> NutritionBulletin 1997;18:337-343.07. Murty PVVS, Lakshmi KV, Bamji MS. Impact of home gardening<strong>and</strong> nutrition education in a district of rural India. Readers’ Forum.Bulletin of the World Health Organization 1999;77:784.
Buildingbridgesfor betternutrition.
44IRON FORTIFICATION – NEW REVELATIONS?IronFortification– NewRevelations?David ThurnhamNorthern Irel<strong>and</strong> Centre for Food <strong>and</strong> Health,University of Ulster, Coleraine, United KingdomKey messagesThe results of the recent r<strong>and</strong>omized controlled trial (RCT) inPemba, 1 where there was more severe child morbidity <strong>and</strong> mortalityin the group receiving supplements of iron <strong>and</strong> folic acid,brought to a halt the unsupervised use of iron supplements toremove iron deficiency anemia – especially in malaria-endemicareas. 2 However, there is uncertainty whether the adverse effectsof the supplements were due to interactions between iron<strong>and</strong> malaria, iron <strong>and</strong> enteric infections, impaired effectivenessof anti-malarial treatment due to the folate, a combination ofall three, or some other explanation. In this issue of <strong>Sight</strong> <strong>and</strong><strong>Life</strong>, I will discuss the issue of iron <strong>and</strong> its apparent effects onenteric bacteria, following a recent article in which the authorsdescribed the impact of poorly bioavailable fortification ironon the profile of the gut microbiota of African children. 3 In thisstudy, the additional iron appeared to increase the proportion ofpathogenic bacteria <strong>and</strong> act as a biomarker of inflammation inthe feces. Nevertheless, there was no evidence of any increasein systemic infection in the children receiving the iron. To try tounderst<strong>and</strong> the meaning of the observations, I will also describesome results from two other papers where the authors examinedindividual sub-strains of commensal Clostridium bacteria<strong>and</strong> showed that they had both individual <strong>and</strong> collective effectson immune cells within the lining of the gut, <strong>and</strong> can have bothpro- <strong>and</strong> anti-inflammatory effects in different circumstances. 4,5Such results indicate that quantitation of the major bacterialstrains within the microbiota may, in fact, tell us very little about> Iron deficiency anemia is a worldwide problem> Fortifying flour with iron is an effective way to address theproblem if iron deficiency is the underlying cause> Electrolytic or elemental iron is commonly used as afortificant in cereal flours> Only 2–3% of these forms of iron are absorbed,so most ends up in the colon> Ivorian children received an extra ~9 mg electrolyticiron/d for 6 months> Children who received the supplemental iron had ahigher proportion of Enterobacteria <strong>and</strong> fewer Lactobacillispp in their feces> Excess iron may accelerate the growth of Enterobacteriaat the expense of Lactobacilli spp.> Iron supplementation is also associated with increasedcolonic inflammation> Cause of inflammation is not known
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>IRON FORTIFICATION – NEW REVELATIONS?4545> There was no increase in systemic inflammation inthe children> Endogenous species of bacteria can stimulate CD4 +lymphocytes to produce T helper (T h ) 17 or T reg cells in theintestinal wall> T h17 cells are potentially pro-inflammatory <strong>and</strong> T reg cells areanti-inflammatory> Iron may stimulate (as yet unknown species of) Enterobacteriato increase pro-inflammatory immune cells in the gut wall> Inflammatory effects of supplemental iron may be reducedby using less but more bioavailable forms of iron <strong>and</strong> phytaseto release intrinsic iron from phytate.the physiological effects of the microbiota on the host. To underst<strong>and</strong>the interaction of iron <strong>and</strong> the microbiota, the source ofthe inflammation <strong>and</strong> /or the bacteria involved must be characterizedfirst.IntroductionDeficiencies of iron, vitamin A, iodine <strong>and</strong> other micronutrientsaffect at least one third of the world’s population, the majorityof whom live in developing countries. Public health nutritionistsare acutely aware that iron deficiency is the most prevalent, <strong>and</strong>it is estimated that just over 2 billion people are anemic due tonutritional <strong>and</strong> non-nutritional causes. 6,7 Reports that iron supplementationof iron-deficient individuals can improve cognitivefunction, school performance, <strong>and</strong> work capacity, 8,9 <strong>and</strong> that severeanemia increases the risk of maternal <strong>and</strong> child mortality, 10have provided a strong rationale for iron interventions.“Iron-deficiency anemia is ahuge problem in the third world”Unfortunately, there are health risks associated with iron. Ithas been known for more than 40 years that it is dangerous togive iron supplements to sick, malnourished children; 11 accidentaloverdose of iron-containing products is a leading cause offatal poisonings in healthy children under six years; 12 diets richin iron have been linked to a higher risk of colon cancer; 13,14 <strong>and</strong>iron supplements, even at nutritional levels, produce a numberof unpleasant side effects such as diarrhea, nausea, <strong>and</strong> vomiting.But the main problem taxing the minds of the regulatoryauthorities is how to combat the huge problem of iron-deficiencyanemia in the developing world, following the publication of the“Pemba” study 1 that found routine treatments of iron <strong>and</strong> folicacid given to pre-school children were associated with higherrisks of severe illness <strong>and</strong> death than in the control groups.Currently, iron supplementation programs have come to a haltaround the world, potentially putting millions of children at riskof the adverse impacts of iron-deficiency anemia. 2Food fortification with iron can be an effective strategy tocontrol iron deficiency anemia, 15 <strong>and</strong> the foodstuffs most oftenused for mass fortification are cereal flours. Worldwide, the mostcommonly used fortificants for flours are elemental iron powderssuch as hydrogen-reduced iron or electrolytic iron, despite theirlow bioavailability, which can often be as low as 90% of unabsorbediron passing unabsorbed into the colon. 3 Iron is able to undergoreduction <strong>and</strong> oxidation, making it important in many physiologicalprocesses. This inherent redox property of iron, however,also renders it toxic when it is present in excess. Iron-mediatedgeneration of reactive oxygen species via the Fenton reaction,if uncontrolled, may lead to cell damage as a result of lipid peroxidation,oxidation of DNA, <strong>and</strong> protein damage. 13 Most ironin the blood <strong>and</strong> tissues of the body is tightly bound to variousproteins to control its reactivity, but there is no similar systemfor sequestration of dietary iron in the gut lumen. Instead, thehuman gut is packed with resident bacteria, collectively knownas the microbiota, <strong>and</strong> the multiple strains vigorously competefor unabsorbed iron, which they need in order to grow. 17 Growthof some pathogenic species of bacteria, however, (e.g. Salmonellaor Shigella) was associated with increased virulence <strong>and</strong>colonization. 18 Animal experiments have shown that increasingdietary iron increased the incidence of diarrhea, <strong>and</strong> increasedthe proportion of pathogenic bacteria within gut lumen. 19 Mindfulof the uncertainty about what caused the higher risks of severeillness <strong>and</strong> mortality in the iron/folate group in Pemba, theWHO consultation that followed cautioned about whether therisks associated with iron supplementation were specific to malariaor applied to other infections, including sepsis <strong>and</strong> entericbacteria. 20Iron fortificationThe best way to prevent micronutrient malnutrition is to ensureconsumption of a balanced diet that is adequate in every nutrient.Unfortunately, this is far from being achievable everywhere,since it requires universal access to adequate food <strong>and</strong> appropriatedietary habits. From this st<strong>and</strong>point, food fortification hasthe dual advantage of being able to deliver nutrients to largesegments of the population without requiring radical changes infood consumption patterns. In fact, fortification has been used
46 IRON FORTIFICATION – NEW REVELATIONS?table 1: Anemia <strong>and</strong> hemoglobin concentration (mean ± SD) in children in Côte d’Ivoire at baseline<strong>and</strong> following 6 months of iron supplementation ¹,²Iron Group (n=69)Control Group (n=70)Baseline 6 months Baseline 6 monthsHemoglobin g/L 110.7 ± 10.5 107.1 ± 10.5 110.8 ± 9.4 106.6 ± 9.7Anemia % 75.4 88.4 71.4 87.1¹ Anemia defined as hemoglobin >80 g/L <strong>and</strong>
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> IRON FORTIFICATION – NEW REVELATIONS? 4747my colleagues, 22,23 the cut-offs should be lower (CRP 5 mg/L;AGP 1.0 g/L), which would suggest that more like 40% of thechildren had systemic inflammation on the basis of AGP alone.Furthermore, the underestimates of inflammation will also haveproduced underestimates of iron deficiency, which were derivedon the basis of serum ferritin concentrations. However, therewas no significant difference in these inflammation biomarkersbetween the two groups at baseline or after intervention, so theunderestimate in systemic inflammation is unlikely to have affectedany difference in iron deficiency between the groups.Detection <strong>and</strong> quantitation of gut microbiotaThe main aim of the Ivorian sub-study was to determine whateffect, if any, the additional iron in the fortified biscuits had onthe gut microbiota. Thirty children were r<strong>and</strong>omly selected fromgroups 1 <strong>and</strong> 4 (see above). None of the children had unusualdietary habits or had received antibiotics in the three monthsbefore the baseline survey. During the survey, the number ofdays of antibiotics did not differ between the two groups. Nochild was given antibiotics in the three weeks before the sixmonthsample. In the mornings at school, fecal samples werecollected into pre-labeled beakers with lids <strong>and</strong> stored for therest of the morning in an ice chest, <strong>and</strong> then aliquots were frozenat -30° C until analysis. Total bacterial DNA was extracted from200 mg fecal samples (Fast DNA SPIN kit, MP Biomedicals, Illkirch,France) <strong>and</strong> DNA was measured at 260 nm, before storingthe samples at -24° C until further analysis.The polymerase chain reaction (PCR) was used to quantifythe total bacterial content <strong>and</strong> individual species in the fecalDNA sample. In the PCR, short nucleotide sequences (= primers),originally obtained from the 16S ribosomal ribonucleic acid(rRNA) sub-units of specific bacteria, attach to complementaryDNA sequences in the fecal DNA sample, together with a DNApolymerase enzyme. 16S rRNA gene primers are used, as theycontain many highly conserved primer binding sites <strong>and</strong>, in addition,hyper-variable regions that can provide species-specificsignature sequences useful for bacterial identification. The DNApolymerase enzymatically assembles new DNA str<strong>and</strong>s fromeach primer using deoxy-nucleotide triphosphates, the buildingblocks from which the new DNA str<strong>and</strong> is synthesized. As thePCR progresses, the DNA generated attaches to more primer <strong>and</strong>is itself used as a template for replication. This sets in motiona chain reaction in which the DNA template is identified or targetedby the primer <strong>and</strong> exponentially amplified. The pro-cess isprecisely temperature regulated <strong>and</strong> timed to enable the productsto be quantitatively related to the starting amount of fecalDNA.Several types of PCR were used on the fecal DNA at baseline<strong>and</strong> six months, to (1) investigate the whole bacterial diversity;(2) identify the species of Lactobacillus; (3) quantify the majorbacterial species; <strong>and</strong> (4) detect bacterial gut pathogens. Baseline<strong>and</strong> six-month samples from the same volunteer were alwaysrun together where gel electrophoresis was involved, foraccurate comparisons.Influence of the fortification iron on the gut microbiotaThe authors investigated whole bacterial diversity by using twouniversal primers for the polymerase chain reaction that attachedto variable regions 2 <strong>and</strong> 3 on the bacterial 16S ribosomalRNA genes, in conjunction with temperature gradient electrophoresisof the resultant products. These qualitative resultssuggested that there was no difference between baseline <strong>and</strong> sixmonths in the absolute number of b<strong>and</strong>s revealed in the electrophoreticgels, i.e., the number of bacterial types or groups in thefecal samples. However, when the consistency (or comparability)in b<strong>and</strong> behavior between baseline <strong>and</strong> six months was compared,consistency in b<strong>and</strong> behavior was significantly greater inthe control than the iron-treated group. That is, b<strong>and</strong> distancesdiffered by only 15 ± 7.5% in the controls, whereas b<strong>and</strong>s differedby 32.3 ± 12.5% (Dice coefficient analysis, P
48 IRON FORTIFICATION – NEW REVELATIONS?table 3: Some characteristics of the main bacteria species in the microbiota (99% anaerobes)BacteroidesA genus of gram negative bacillus bacteria; motile <strong>and</strong> non motile forms; non-endospore forming;anaerobes but some are aerotolerant; cell wall often confers pathogenicity by containing lipopolysaccaride(LPS); some opportunistic infections caused by infection of the peritoneal cavity <strong>and</strong> appendicitis; mostsubstantial portion of the human mammalian gastrointestinal flora (~30%); bulk may benefit host byexcluding potential pathogens; will metabolize simple sugars but mainly polysaccharides; important rolein metabolizing complex molecules to simple ones; resistant to a wide variety of antibiotics.Example Bacteroides fragilis (causes most opportunistic peritoneal infections)EnterobacteriaGram negative; motile; facultative anaerobes; rod shaped; several strains pathogenic but usual route ofinfection is opportunistic; most infections in immune-compromised hospital patients frequently targetingthe urinary <strong>and</strong> respiratory tracts.Examples include Escherichia coli, Salmonella spp, Shigella sppBifidobacteriaLactobacilliGram positive; non-motile; branched shape; anaerobic; aid digestion; may lower the risk of allergy; somespecies used as probiotics; before 1960 species referred to as Lactobacillus bifidus; optimal growth at moreacid pH which may discourage growth of gram negative organismsGram positive; facultative anaerobes; aerotolerant <strong>and</strong> high tolerance to hydrogen peroxide; producelactic acid which lowers pH <strong>and</strong> discourages growth of some pathogenic bacteria; as many as 125 speciesidentified; many species do not require iron for growth; potential therapeutic properties – anti-inflammatory,anti-neoplastic; potential probiotic activity; used for production of many foods e.g. cheese, yogurt,sauerkraut, beer, pickles etc; convert lactose <strong>and</strong> other sugars to lactic acid.of the bacterial counts or changes in the fecal bacteria <strong>and</strong> baselineserum ferritin, transferrin receptors or zinc protoporphyrinconcentrations.Gut inflammation in the Ivorian childrenThe authors measured fecal concentrations of the inflammatoryprotein, calprotectin. Calprotectin is a calcium-binding proteinthat is found in all body fluids, in proportion to the level of inflammationpresent. Calprotectin is derived predominantly fromneutrophils <strong>and</strong>, to a lesser extent, from monocytes <strong>and</strong> reactivemacrophages. The presence of calprotectin in the feces isdirectly proportional to neutrophil migration towards the intestinaltract. 26 Fecal calprotectin is remarkably stable <strong>and</strong> auseful marker of gastrointestinal inflammation. 27,28 Inflammationin the bowel implies a loss of barrier function <strong>and</strong> a lossof tolerance against luminal <strong>and</strong> self antigens, <strong>and</strong> both thesephenomena cause the recruitment of leukocytes in the intestinalwall. 28 Activated leukocytes infiltrating into the intestinalmucosa are detected in the feces due to epithelial shedding inthe intestinal lumen. The most important leukocyte populationin the mucosal wall is polymorphonuclear neutrophils; hence,there is an increase in fecal calprotectin when there is intestinalinflammation. Several studies have shown that a cut-off of30 mg/L had 100% sensitivity <strong>and</strong> 94% specificity for screeningirritable bowel syndrome, but the calprotectin threshold predictiveof systemic inflammation (CRP >6 mg/L) was 284 mg/L. 28Thus, inflammation in the bowel will not necessarily be detectedsystemically until intestinal inflammation is severe.Fecal calprotectin concentrations in the Ivorian childrenwho received additional iron for six months were significantly
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> IRON FORTIFICATION – NEW REVELATIONS? 4949log number bacteria / g fecesincreased (Figure 4). The authors used a more sensitive assaythan that described above, in which the median calprotectin concentrationsin healthy persons was 25 μg/g 29 or below a cut-off of50 μg/g. 26 Hence, the calprotectin concentration in the childrenwho received iron, viz. 75 μg/g feces, indicated evidence of marfigure1: Profile of fecal bacteria in Ivorian childrenbefore iron supplementation121086420Total countsBacteroidesEnterobacteriaBifidobacteriaLactobacilliColumns are means of the log number of gene copies of cell numbersof bacteria indicated by real-time polymerase chain reaction (PCR)on baseline fecal DNA samples from Ivorian children (n = 59). All countswere significantly different from each other (one factor ANOVA with posthoc ‘t’ tests; P < 0.02). Modified from reference 3ginal intestinal inflammation. Furthermore, the authors found acorrelation between the changes in calprotectin <strong>and</strong> the changesin numbers of enterobacteria (r = 0.32, P
50 IRON FORTIFICATION – NEW REVELATIONS?table 4: Total numbers of bacteria in control <strong>and</strong> iron groupafter 6 months iron supplementation ¹Control Group¹ Data shown are mean (SE) log number of bacteria/g fecesIron GroupBaseline 11.29 (0.67) 11.62 (0.94)6 Months 11.28 (0.81) 11.78 (0.59)table 5: Comparison of main bacterial groups in feces of Ivorianchildren <strong>and</strong> young European adultsBacterialIvorian children Young European adultsgroupBacteroidesEnterobacteriaBifidobacteriaLactobacilliData for Ivorian childrenfrom reference Log numberbacteria/g feces1087.56.5from reference 3 <strong>and</strong> forLog numberbacteria/g feces9.25.99.26.7European adultsof enterobacteria by a further 100 million (log numbers 7.8 to8.3 bacteria/g feces) while reducing the proportion of lactobacilli(Figure 2). If these changes in enterobacteria <strong>and</strong> lactobacilliare expressed as percentages of the total number of bacteriain the microbiota, there is a four-fold increase in enterobacteriafrom 0.01 to 0.039%, while there is a fourfold fall in the proportionof lactobacilli from 0.004% to 0.001%. There was also afall in bifidobacteria, but this was not significant.Reasons why iron favored the growth ofenterobacteria over lactobacilliIron is a nutrient which is essential for the growth of most bacteria,but not in the case of most Lactobacilli spp (Table 3). Mostenteric gram-negative pathogens, including Salmonella spp,E.coli <strong>and</strong> Shigella spp, 18 take up iron-siderophore complexesby specific outer membrane receptors <strong>and</strong> display increasedvirulence in situations of increased iron availability. 32 It is alsointeresting to note that fecal lactoferrin is as good an indicatorof gut inflammation as calprotectin. 33 Lactoferrin is a powerfuliron-binding protein that is particularly effective under acid conditions<strong>and</strong> is derived from the polymorphonuclear neutrophilsthat are drawn into the gut lining at the onset of inflammation.Whether the neutrophil lactoferrin depresses pathogen growthat the mucosal lining is not known, but bacterial growth in themicrobiota will be limited by iron availability, <strong>and</strong> the additionaliron provided by the supplement may have provided a growthadvantage for the enterobacteria, which enabled them to increasecell numbers at the expense of the lactobacilli <strong>and</strong> possiblythe bifidobacteria.The potential hazards of iron loading are well recognized. 34Not only do we have the results of the recent study in Pemba 1but it has previously been noted that iron given to patients withquiescent tuberculosis appeared to reactivate the disease. 35 Inaddition, Murray <strong>and</strong> colleagues noted that, in areas of hyperendemicPlasmodium falciparum, patients with clinical irondeficiency enjoyed an attenuated incidence <strong>and</strong> severity of malariabut when such subjects were fed an iron-replete diet, manyexhibited a recrudescence of malaria 36 <strong>and</strong> when iron-deficientMaasai pastoralists were treated with iron, there was an increasein amebiasis in the iron group. 37The significant correlation between the increase in enterobacteria<strong>and</strong> fecal calprotectin concentrations (r = 0.32, P
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> IRON FORTIFICATION – NEW REVELATIONS? 5151Fecal Calprotectin μg/g fecesfigure 3: Profile of fecal bacteria in Ivorian childrenbefore iron supplementation80706050403020100Control 0Control 6Iron 0Iron 6Calprotectin concentrations were measured by immunoassay <strong>and</strong> expressedas μg/g feces. Median calprotectin level in healthy subjectswas described as 26 μg/g. 29 Concentration in the children who receivedadditional iron increased significantly (*, ANOVA with post hoc t-tests,P
52 IRON FORTIFICATION – NEW REVELATIONS?disease which was reported in 2004 to affect 1.4 million peoplein the United States, <strong>and</strong> 2.2 million in Europe. 39T reg cells are also derived from CD4 + T cells. Their importancelies in their ability to suppress the immune responses of othercells – that is, to keep the immune responses in check. The authorsshowed that the increase in Treg in response to oral inoculationwith Clostridia (spp) during the early life of conventionallyreared mice promoted anti-inflammatory immune responses<strong>and</strong> were more resistant to experimental models of allergy <strong>and</strong>experimental colitis – the murine equivalent of IBD. The paperis a fascinating piece of investigative murine microbiology but,unfortunately, there is not space to discuss it in detail. Interestingly,the ability to stimulate T regs was not blocked by SFBbacteria or Lactobacilli. A cocktail of 45 strains of Clostridia wasmore effective in raising T reg production than three strains indicating,possibly, that a number of stimuli is necessary for a fullresponse. 5 Clostridium species appear to be specialized in theirability to promote T reg cell accumulation in the colon. 25 Adherenceto the intestinal epithelium did not appear to be necessary,as in the case of SFB bacteria, possibly because Clostridia spppromoted the release of the transforming growth factor- thatstimulated CD4 + T cell differentiation. 25 The effects of these bacteriaon T-cell development give us a clear indication that, potentially,many fecal bacteria may have an important influenceon immune defenses in the gut <strong>and</strong> on the systemic health of thehost. We currently have little idea of the specific role of iron inthis “orchestra.”Concluding remarksThree papers have been discussed in this report, which describesinteractions between diet, the microbiota <strong>and</strong> the immune system.The paper by the Zimmermann group illustrates that anincrease in a poorly available form of iron was associated withalterations in the colonic microbiota <strong>and</strong> evidence of inflammationin the intestinal lining. 3 The two other papers illustrate thatspecific, or groups of, gram-positive bacteria can have stimulatoryeffects on the immune system <strong>and</strong> promote potentiallyinflammatory 4 <strong>and</strong> anti-inflammatory 5 immune responses. Theiron supplementation study identified an increase in the gramnegative,enterobacterial fecal fraction as being positively associatedwith calprotectin, a biomarker of inflammation. Therewere also increases in several species of pathogenic bacteria inthis group <strong>and</strong> some were identified in several of the children. Inaddition, there was a reduction in the gram-positive Lactobacillusgroup of bacteria.Host protection against bacterial pathogenicity is partly affordedby the large number of commensal bacteria in the microbiota,many of which will occupy important niches within theintestinal lining <strong>and</strong> so prevent occupancy by incoming pathogenicstrains. 40 Dietary requirements will also determine whichbacteria can propagate themselves at the expense of others. Ironis an important regulator of bacterial growth <strong>and</strong> pathogenicity.Supplemental iron may well have been responsible for the fourfoldincrease in the numbers of enterobacteria <strong>and</strong> the associatedinflammation. The particular bacterial species <strong>and</strong> mechanismcausing the inflammation are not known, but the markedeffects that SFB bacteria <strong>and</strong> Clostridia spp can have on T-cellregulation indicate the type of mechanism that may have beeninvolved. As the authors suggest, minimizing the inflammatoryeffects of supplemental iron may be possible with a lower doseof more bioavailable iron to promote iron uptake <strong>and</strong> reduce theamount available to the microbiota.In the last issue of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, Barbara Troesch, from thesame group, reported on the successful use of low-dose ironfrom NaFeEDTA, in combination with ascorbic acid <strong>and</strong> phytase,to increase body iron stores <strong>and</strong> reduce iron <strong>and</strong> zinc deficiencyin South African school children. 41 It should also be rememberedthat the study in Côte d’Ivoire was intended to show the potentialeffects of food fortified with iron. In fact, the iron load was18.2 mg/day, given in a biscuit four days/week. The equivalentdaily dose of fortified iron would have been 8.8 mg iron/day, butthis amount may not have had the same microbiological or inflammatoryeffects as the higher dose. Currently, the selection ofthe type <strong>and</strong> quantity of vitamins <strong>and</strong> minerals to add to flour,either as a voluntary st<strong>and</strong>ard or a m<strong>and</strong>atory requirement, lieswith national decision-makers in each country. As a result, thechoice of compounds as well as quantities should be viewed inthe context of each country’s situation. Recommended amountsof electrolytic iron are only given where the daily consumptionof flour is >150 g (60 ppm) or >300 g (40 ppm) for low extractionflour or 20 <strong>and</strong> 15 ppm resp. for those amounts of high extractionflour. 42 Three hundred grams of flour containing 40 ppm Fe isequivalent to a daily intake of 18 mg iron, i.e. comparable to theamount used in the Ivorian children. Thus, the effects of the ironsupplement reported by Zimmermann <strong>and</strong> colleagues 3 are applicableto those countries where flour is fortified with electrolyticiron, <strong>and</strong> there is a high consumption of wheat flour.Correspondence: David I Thurnham, 46 High Street,Little Wilbraham, Cambridge CB21 5JY, United KingdomE-mail: di.thurnham@ulster.ac.uk
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> IRON FORTIFICATION – NEW REVELATIONS? 5353References01. Sazawal S, Black RE, Ramsan M et al. Effects of routine prophylacticsupplementation with iron <strong>and</strong> folic acid on admission to hospital<strong>and</strong> mortality in preschool children in a high malaria transmissionsetting: community-based, r<strong>and</strong>omised, placebo-controlled trial.Lancet 2006;367:133-143.02. Suchdev PS, Leeds IL, McFarl<strong>and</strong> DA et al. Is it time to change theguidelines for iron supplementation in malarial areas?J Nutr 2010;140:875-876.03. Zimmermann MB, Chassard C, Rohner F et al. The effects of ironfortification on the gut microbiota in African children: a r<strong>and</strong>omizedcontrolled trial in Cote d'Ivoire. Am J Clin Nutr 2010;92:1406-1415.04. Ivanov II, Littman DR. Segmented filamentous bacteria take thestage. Mucosal Immunol 2010;3:209-212.05. Atarashi K, Tanoue T, Shima T et al. Induction of ColonicRegulatory T Cells by Indigenous Clostridium Species. Science<strong>2011</strong>;331:337-341.06. World Health Organization. Iron deficiency anaemia: assessment,prevention <strong>and</strong> control. A guide for programme managers. WHO/NHD/01.3. 2001. Geneva, World Health Organisation.07. Guidelines on food fortification with micronutrients. Geneva: WorldHealth Organisation & Food <strong>and</strong> Agricultural Organisation; 2006.08. Haas JD, Brownlie T4. Iron deficiency <strong>and</strong> reduced work capacity:a critical review of the research to determine a causal relationship.J Nutr 2001;131:676S-690S.09. Pollitt E. The developmental <strong>and</strong> probabilistic nature of the functionalconsequences of iron-deficiency anemia in children. J Nutr2001;131:669S-675S.10. Stoltzfus RJ. Iron-deficiency anemia: reexamining the nature <strong>and</strong>magnitude of the public health problem. Summary: implications forresearch <strong>and</strong> programs. J Nutr 2001;131:697S-700S.11. McFarlane H, Reddy S, Adcock KJ et al. Immunity, transferrin <strong>and</strong>survival in kwashiorkor. B M J 1970;4:268-270.12. United States Food <strong>and</strong> Drug Administration. US FDA Backgrounder.Preventing iron poisoning in children. 62 FR 2217. 1997.13. Chua AC, Klopcic B, Lawrance IC et al. Iron: an emerging factor incolorectal carcinogenesis. World J Gastroenterol 2010;16:663-672.14. Bastide NM, Pierre FH, Corpet D. Heme iron from meat <strong>and</strong> risk ofcolorectal cancer: a meta-analysis <strong>and</strong> a review of the mechanismsinvolved. Cancer Prev Res (Phila) <strong>2011</strong>; Jan 5 ahead of print.15. Baltussen R, Knai C, Sharan M. Iron fortification <strong>and</strong> iron supplementationare cost-effective interventions to reduce iron deficiencyin four subregions of the world. J Nutr 2004; 134:2678-2684.16. Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet2007; 370:511-520.17. Andrews SC, Robinson AK, Rodríguez-Quiñones F. Bacterial ironhomeostasis. FEMS Microbiol Rev 2003;27:215-237.18. Naikare H, Palyada K, Panciera R et al. Major role for FeoBin Campylobacter jejuni iron acquisition, gut colonization <strong>and</strong>intracellular survival. Infect Immun 2006; 74:5433-5444.19. Lee SH, Shine P, Choi J et al. Effects of dietary iron levels on growthperformance, hematological status, liver mineral concentration,fecal microflora, <strong>and</strong> diarrhea incidence in weanling pigs. Biol TraceElement Res 2008;126:S57-S68.20. World Health Organisation. Conclusions <strong>and</strong> recommendations ofthe WHO consultation on prevention <strong>and</strong> control of iron deficiencyin infants <strong>and</strong> young children in malaria-endemic areas. Food NutrBull 2007;28:S621-S627.21. Rohner F, Zimmermann MB, Amon RJ et al. In a r<strong>and</strong>omizedcontrolled trial of iron fortification, anthelmintic treatment, <strong>and</strong>intermittent preventive treatment of malaria for anemia control inIvorian children, only anthelmintic treatment shows modestbenefit. J Nutr 2010;140:635-641.22. Thurnham DI, McCabe GP, Northrop-Clewes CA et al. Effect ofsubclinical infection on plasma retinol concentrations <strong>and</strong> assessmentof prevalence of vitamin A deficiency: meta-analysis. Lancet2003;362:2052-2058.23. Thurnham DI, McCabe LD, Haldar S et al. Adjusting plasma ferritinconcentrations to remove the effects of subclinical inflammation inthe assessment of iron deficiency: a meta-analysis. Am J Clin Nutr2010; 92:546-555.24. Monira S, Alam NH, Suau A et al. Time course of bacterial diversityin stool samples of malnourished children with cholera receivingtreatment. J Pediatr Gastroenterol Nutr 2009;48:571-578.25. Barnes MJ, Powrie F. The gut's Clostridium cocktail. Science<strong>2011</strong>;331:289-291.26. Gisbert JP, McNicholl AG. Questions <strong>and</strong> answers on the role offaecal calprotectin as a biological marker in inflammatory boweldisease. Dig Liver Dis 2009;41:56-66.27. Fagerberg UL, Lööf L, Merzoug RD et al. Fecal calprotectin levels inhealthy children studied with an improved assay. J Pediatr GastroenterolNutr 2003;37:472468.28. Angriman I, Scarpa M, D'Incà R et al. Enzymes in feces: useful markersof chronic inflammatory bowel disease. Clin Chim Acta 2007;381:63-68.29. Tøn H, Br<strong>and</strong>snes, Dale S et al. Improved assay for fecal calprotectin.Clin Chim Acta 2000; 292:41-54.30. Hopkins MJ, Sharp R, Macfarlane GT. Age <strong>and</strong> disease relatedchanges in intestinal bacterial populations assessed by cell culture,16S rRNA abundance, <strong>and</strong> community cellular fatty acid profiles.Gut 2001;48:198-205.⇢
54 IRON FORTIFICATION – NEW REVELATIONS?31. Singhal A, Macfarlane G, Macfarlane S et al. Dietary nucleotides <strong>and</strong>fecal microbiota in formula-fed infants: a r<strong>and</strong>omized controlledtrial. Am J Clin Nutr 2008;87:1785-1792.32. Bullen J, Griffiths E, Rogers H et al. Sepsis: the critical role of iron.Microbes Infect 2000;2:409-415.33. Gisbert JP, McNicholl AG, Gomollon F. Questions <strong>and</strong> answers onthe role of fecal lactoferrin as a biological marker in inflammatorybowel disease. Inflamm Bowel Dis 2009;15:1746-1754.34. Weinberg ED. The hazards of iron loading. Metallomics2010;2:732-740.35. Weinberg GA, Boelaert JR, Weinberg ED. Iron <strong>and</strong> HIV infection. In:Friis H, editor. Micronutrients <strong>and</strong> HIV infection. 2002. 135-157.36. Murray MJ, Murray NJ, Murray AB et al. Refeeding malaria <strong>and</strong> hyperferremia.Lancet 1977;i:653.37. Murray MJ, Murray A, Murray CJ. The salutary effect of milk on amoebiasis<strong>and</strong> its reversal by iron. B M J 1980;2:1151-1152.38. Korn T, Bettelli E, Oukka M et al. IL-17 <strong>and</strong> Th17 Cells. Ann RevImmunol 2009; 27:485-517.39. Loftus EV Jr. Clinical epidemiology of inflammatory bowel disease:Incidence, prevalence, <strong>and</strong> environmental influences. Gastroenterology.2004 May;126(6):1504-17. Gastroenterol 2004;126:1504-1517.40. Borriello SP, Barclay FE. Protection of hamsters against Clostridiumdifficile ileocaecitis by prior colonisation with non-pathogenicstrains. J Med Microbiol 1985; 19:339-350.41. Troesch B. Optimized micronutrient powder containing low levels ofhighly bioavailable iron <strong>and</strong> zinc together with EDTA, phytase <strong>and</strong>ascorbic acid improves the nutritional status of children. <strong>Sight</strong> <strong>and</strong><strong>Life</strong> 2010;3:9–11.42. WHO, FAO, UNICEF et al. Recommendations on Wheat <strong>and</strong> MaizeFlour Fortification Meeting Report: Interim Consensus Statement.WHO/NMH/NHD/MNM/09.1. 2009. Geneva, WHO (http://www.who.int/nutrition/publications/micronutrients/wheat_maize_fort.pdf,accessed February <strong>2011</strong>).Erratum: OptimizedMicronutrient PowderIn the article Optimized MicronutrientPowder in <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> <strong>Magazine</strong>3/2010, the figures in Table 2 wereincorrect. The table to the right has thecorrect figures. We apologize for anyconfusion this error may have caused.table 2: Composition of the micronutrient powder usedin the intervention studyNutrient Pro serving Pro kg premixVitamin A (RAE) 400 μg 80 mgVitamin D 5 μg 1 mgVitamin E (TE) 5 mg 1 gThiamine 0.5 mg 100 mgRiboflavin 0.5 mg 100 mgPyridoxine 0.5 mg 100 mgFolic Acid 90 μg 18 mgNiacin 6 mg 1.2 gPantothenic acid 2 mg 400 mgVitamin B12 0.9 μg 180 μgVitamin C 60 mg 12 gIron (as NaFeEDTA) 2.5 mg 500 mgCalcium 200 mg 40 gCopper 0.34 mg 68 mgIodine 30 μg 6 mgSelenium 17 μg 3.4 mgZinc 2.5 mg 500 mgPhytase 190 FTU 38,000 FTUCarrier Ad 5g ad 1000g
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> OPINION 1 5555Opinion 1: Comments on “Iron Fortification– New Revelations?”Glenn GibsonDepartment of Food <strong>and</strong> Nutritional Sciences,University of Reading, United KingdomThe decision to withdraw iron supplementation in certain malaria-affectedareas was the subject of David Thurnham’s objectiveassessment of recent science findings. David has outlined someof the thinking behind this decision <strong>and</strong> input his own evidencebasedviews.As with so many current nutritional concepts, the drift of attentionhas been drawn to the gut microbiota. This is not surprising,given the vast numbers of bacteria that use the human alimentarytract as their home <strong>and</strong> their concomitant major impactupon metabolism. I especially like David’s conclusion that it isnot enough nowadays to simply measure predominant gut floracomponents without an assessment of the functional or physiologicalimpact. Perhaps some bacteria not present in largenumbers can exert a major impact upon health. In this context,“It is not enoughnowadays to simplymeasure predominantgut flora componentswithout an assessmentof the functional orphysiological impact”I have always been struck by the fact that it is easily accepted,by science <strong>and</strong> medical communities, that just a few cells of apathogen like E. coli 0157 can exert destructive effects, yet theimpact of a larger number of probiotic microbes gets writtenoff, more often than not. The science of metabonomics recentlyentered the gut microbiology arena <strong>and</strong> offers a similar “revolution”in our underst<strong>and</strong>ing of the impact of gut microbes to thatgenerated by molecular-based assessments of composition inthe last decade. 1On that note, David cites an extensive study which led to thecontentious decisions on iron supplementation. High throughput<strong>and</strong> accurate PCR-based technologies were used to assessthe gut microbiota in Ivorian populations. 2 These were seen todiffer markedly from European profiles, although parallel studieswere clearly not feasible <strong>and</strong> differing techniques may havebeen used. That aside, it seemed that the Ivorians harboredhigher levels of enterobacteria <strong>and</strong> lesser populations of Grampositive bacteria said to be beneficial (bifidobacteria). The ironuse was said to fortify the enterobacteria, <strong>and</strong> that led to healthissues. It is worth noting that these are facultative, rather thanstrict, anaerobes whose enhanced growth rates are likely ableto allow better scavenging of iron. I was also struck by the detectionof salmonellae <strong>and</strong> shigellae. These are clear pathogenswhich often only exist in a transient manner. In European trialsthey are hardly ever reported unless in association with a foodsafety outbreak. Perhaps this is the key to the health difficultiesseen, <strong>and</strong> maybe those few probiotics that boost bifidobacteria<strong>and</strong> consequently decrease pathogens are worth trying. 3 Microbiotamodulation through probiotics or prebiotics is popular inEurope, North America <strong>and</strong> Asia, but it seems to me that theIvorian children studied here could be major benefactors of aharmless intervention.David also gives us an example of how functional microbialassessments are needed rather than just compositional. Theclostridia were seen to exert varying effects upon inflammation⇢
56 OPINION 1 / 2depending upon species type <strong>and</strong> experimental conditions. NotingDavid’s cited implications of some clostridia with IBD, thisstory could have an added twist. Research has shown elevatedlevels of microbially generated sulphides in the fecal stream ofulcerative colitis (UC) sufferers (one of two major types of IBD). 4Above a certain level, sulphides are destructive to colonocytefunction, resulting in typical inflammatory patterns of UC. Theyare also volatile, <strong>and</strong> can be rendered innocuous by binding tometals – such as iron!Correspondence: Glenn Gibson, Department of Food <strong>and</strong>Nutritional Sciences, University of Reading, Whiteknights, PO Box217, Reading, Berkshire, RG6 6AH, United KingdomE-mail: g.r.gibson@reading.ac.ukReferences01. Martin FP, Sprenger N, Montoliu I et al. Dietary modulation of gutfunctional ecology studied by fecal metabonomics. J Proteome Res2010; 9:5284–529502. Zimmermann MB, Chassard C, Rohner F et al. The effects of ironfortification on the gut microbiota in African children: a r<strong>and</strong>omizedcontrolled trial in Cote d’Ivoire. Am J ClinNutr 2010; 92:1406–1415.03. Saulnier DM, KolidaS, Gibson GR. Microbiology of the human intestinaltract <strong>and</strong> approaches for its dietary modulation. Curr PharmDesign 2009;15:1403–1444.04. Rowan FE, Docherty NG, Coffey JC et al. Sulphate-reducing bacteria<strong>and</strong> hydrogen sulphide in the aetiology of ulcerative colitis. Br JSurg 2009;96:151–158.Opinion 2: Venturing into the Jungle of MultipleInteractions between Iron, Modulating Influences,<strong>and</strong> Human HealthKlaus SchuemannTechnische Universität München, Zentralinstitutfür Ernährung und Lebenswissenschaften, GermanyOver the last 10 years it has become a truism that iron is a double-edgedsword. It is essential for bacteria, parasites <strong>and</strong> hostorganisms, but can also cause oxidative damage. Dr Thurnham’scontribution is on the crest of present day efforts to widen thescope from such direct iron effects to the increasing number ofmutual interactions <strong>and</strong> cross-talks, such as those between iron,the composition of intestinal flora, <strong>and</strong> the well-being of thehost. We congratulate <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> on recognizing this newtrend <strong>and</strong> inviting this article.We must stay aware, however, that the subject under discussionhere is only the tip of an iceberg which might be termed“modulation of health-related iron effects.” Some examplesmay illustrate how complex the scene has become. Extracellularbacteria, indeed, merrily hijack each other’s iron-fishing siderophoresby imitating the siderophore-receptors of competingspecies. The host organism does the same in trying to recuperatepart of its iron. Playing this game more or less successfullymodulates the expansion of, for example, pathogenic germs <strong>and</strong>thus the prevalence of corresponding disease. Some bacteriaeven hijack entire heme molecules to an extent permitting themto abolish endogenous heme biosynthesis. 1Another major player in the multidimensional contest foriron supplies is the host’s homeostatic regulation of iron-absorption<strong>and</strong> distribution kinetics. 2 In the Pemba trial, 3 irondeficientchildren profited from iron supplementation, whileiron-adequate children suffered from more severe clinical malariacourses. This may seem paradoxical at first glance, as theabsorption of potentially harmful iron increases iron deficiency.However, iron drainage to hematopoiesis seems to be increasedto an even higher extent in terms of iron deficiency, so that lessiron circulates with the plasma.By contrast, iron concentration in the gut lumen is not homeostaticallyregulated. It depends on iron ingestion <strong>and</strong> inducesoxidative stress, the extent of which is modulated by dietaryantioxidants. The results of this interaction can be determinedin the stool. 4 Correspondingly, low dietary iron content reducedthe extent of Crohn-like intestinal bowel disease in a murinemodel. 5 This concurred with increases in endoplasmic reticulum(ER) stress in the ileal mucosa such as the impaired regulation
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> OPINION 2 5757of protein folding. Injecting the missing dietary iron quantitiesparenterally did not re-induce ileal Crohn symptoms, showingthat the underlying pathology depends on luminal iron concentrations.Iron also mutually interacts with immunological responsesin multiple ways, as illustrated in Crohn’s disease in a correspondingcomment. 6 All these events illustrate that the role of iron in theunderlying pathology is extensively modulated by a considerablenumber of interfering processes.With the wide application of powerful genetic <strong>and</strong> biochemicaltools, the number of examples of such interactions is likelyto exp<strong>and</strong> exponentially in the near future. Their clinical implicationswill serve to judge the relevance of such novel modulatingeffects. Some of these may be academic in nature, but othersmay yield ground-breaking new therapeutic principles or impulsesfor public health <strong>and</strong> nutrition. We hope that <strong>Sight</strong> <strong>and</strong><strong>Life</strong> will continue to report on such developments.Correspondence: Klaus Schuemann, Zentralinstitut fürErnährung und Lebensmittelwissenschaft, Technische UniversitätMünchen,Gregor-Mendelstr 2, D-85350 Freising-Weihenstephan,Germany E-mail: kschuemann@schuemann-muc.deReferences01. Nairz M, Schroll A, Sonnweber T et al. The struggle for iron – a metalat the host-pathogen interface. Cell Microbiol 2010;12:1691–702.02. Hentze MW, Muckenthaler MU, Galy B et al. Two to tango: regulationof mammalian iron metabolism. Cell 2010;142:24–38.03. Sazawal S, Black RE, Ramsan M et al. Effects of routine prophylacticsupplementation with iron <strong>and</strong> folic acid on admission to hospital<strong>and</strong> mortality in preschool children in a high malaria transmissionsetting: community-based, r<strong>and</strong>omised, placebo-controlled trial.Lancet 2006;367:133–43.04. Orozco M, Solomons NW, Schümann K et al. Antioxidant-rich oralsupplements attenuate the effects of oral iron on in situ oxidationsusceptibility of human feces. J Nutr 2010;149:1105–10.05. Werner T, Wagner SJ, Martinez I et al. Depletion of dietary ironprevents Crohn’s disease-like ileitis affecting epithelial stressrepression <strong>and</strong> the gut microbial ecology. Gut 2010, on line,10.1136/gut.2010.216929. February <strong>2011</strong>.06. Weiss G. Iron in the inflamed gut: another pro-inflammatory hit?Gut 2010, on line, 10.1136/gut 2010 229047. February <strong>2011</strong>.
58A DAY IN THE LIFE OF JOHANN C JERLING<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>InterviewA Day in the <strong>Life</strong> of Johann C JerlingJohann C Jerling (PhD)is the Director of TReNDS – Centre of Excellence forNutrition at North-West University (PotchefstroomCampus), South Africa. He talks about his work atTReNDS, as well as his involvement in initiatives suchas the African Nutrition Leadership Program (ANLP).<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> (SAL): Johann, what does your work as the Directorof TReNDS involve?Johann Jerling (JJ): I became the director fairly recently, onJanuary 1, <strong>2011</strong>. I see my role as developing <strong>and</strong> leading a team,which in this case is a team of nutrition scientists. In general,as a group, we spend 40 percent of our time on undergraduatestudent training, 40 percent on research, <strong>and</strong> 20 percent on theimplementation of expertise.SAL: What do you do in the course of a working day, <strong>and</strong> whatimpact does it make?JJ: I aim to create an environment where team members excelat what they do. I also believe that we should really enjoy whatwe do, which is something that is sometimes neglected in ourworld. I aim to create an environment where people enjoy whatthey are doing. I try to achieve this on different levels; the firstthing is to listen to what people have to say, <strong>and</strong> to try <strong>and</strong> solveproblems. I have access to resources, so I try to use these wisely.If you can throw money at a problem, that’s fine, but very oftenit’s about supporting someone, creating energy, <strong>and</strong> then, sometimes,putting a little bit of fun into it, so we don’t take ourselvestoo seriously!We are a group of about 18 academic staff members, as wellas about 30 graduates <strong>and</strong> postgraduates, who form a centralpart of our research effort. We carry out research in variousfields at a level ranging from molecular to societal. The first isin the area of diet <strong>and</strong> hemostasis, or blood clotting. We have aresearch program in nutrigenetics that is fairly new <strong>and</strong> togetherthey form the basis of our molecular work. We also do researchin the area of micronutrients <strong>and</strong> cognition; in body composition,both overweight <strong>and</strong> underweight; <strong>and</strong> we have a research programon nutrition transition, which is an overriding theme thatwe have. As with most parts of the developing world, in SouthAfrica nutrition transition already has a huge impact on thehealth systems of our <strong>and</strong> other countries. We also have a verystrong research program in fatty acids <strong>and</strong> lipids, which is linkedto cognition, micronutrient status, <strong>and</strong> under- <strong>and</strong> over-nutrition.Another theme is best described as nutrition in exercise<strong>and</strong> sport. This is fairly new <strong>and</strong> we are investigating the possibilityof a postgraduate specialization degree in this area.We try to develop track records in all of these areas. I reallybelieve in teamwork. I don’t believe that, as academics, we c<strong>and</strong>o everything well – I’m a big fan of getting strong teams together<strong>and</strong> pooling the expertise that is necessary to do the job <strong>and</strong> doit well. We develop trans-disciplinary research teams around importanthealth themes <strong>and</strong> steer clear from developing researchareas focused on individual capabilities. Sometimes you are ateam member, sometimes you are a leader; it all depends onwhere you are at.SAL: Is there such a thing as a “normal” day for you?JJ: Not at all! Every once in a while, I wish I could have a daywhere I could say, “Now it’s finished,” but that’s not the case inmy role. I work long hours, <strong>and</strong> every day is a mixture of all sortsof things. Some are administrative, others might be researchrelated,but a lot of them are people-related. People come to me⇢
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>59“Although it’s something thatI haven’t done for three or fouryears, I really enjoy fl y fi shing, asit takes my mind off everything.”A stunning sunset – taken by a team member of theAfrican Nutrition Leadership Program (ANLP)
60 A DAY IN THE LIFE OF JOHANN C JERLINGmany African countries. Above all, it’s great to see how peopledevelop <strong>and</strong> progress in their careers, <strong>and</strong> as part of this Africawidenetwork. I find it really satisfying.SAL: What does <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> mean to you in the context of theglobal fight against malnutrition?Johann Jerling <strong>and</strong> the ANLP team, from left to right:Violet Mugalavai, Marlien Pieters, Victor Owino, Nyagosya Range,Namukolo Covic, Johann Jerling, Mercy Achu, Charles Mokoena,Olympia Keino, Chrissie Thakwalakwa.for advice <strong>and</strong> a chat, so I do spend a lot of my time on this. If theteam is doing well, I’m happy <strong>and</strong> think I’ve done my bit.SAL: What do you look forward to in your working day, <strong>and</strong> whatdo you find challenging?JJ: Seeing people grow gives me a huge amount of satisfaction.I enjoy solving problems, <strong>and</strong> seeing the end result of solvinga problem. I also greatly enjoy discovering new things, whichmight be really complex … or really simple. Overall, I really enjoythe enthusiasm in the group. We have some more senior researchers,plus a fairly large batch of 30-somethings, who arefun to work with, as they are all developing careers, <strong>and</strong> are energetic,adaptable <strong>and</strong> eager to try to do things in a new way. Itreally adds to the feeling of the whole job being worthwhile.SAL: Which aspect of your work is most important to you?JJ: The activity I find most rewarding is the leadership developmentprogram that I am director of – the African NutritionLeadership Program, or ANLP. Every year about 120 c<strong>and</strong>idatesapply from all over Africa. Thirty get selected <strong>and</strong> join a 10-dayleadership development course. To me, this is the single mostworthwhile thing that I have done in my whole life. It’s a lot ofreally hard work, but the rewards that I get in many ways arejust fantastic. It’s great to see how people discover things aboutthemselves that they never knew before, how they change in environmentswhere they are challenged in all sorts of ways. It’salso wonderful to see how we can get 30 people together from17 different countries for 10 days, <strong>and</strong> discover how irrelevantthe differences between nations become. I can see how stronglyreligious Christians <strong>and</strong> devout Muslims can work together, despitethe fact that we have seen conflict along religious lines inJJ: Maybe six years ago, if I heard someone talk about <strong>Sight</strong> <strong>and</strong><strong>Life</strong>, I would have thought about vitamin A. Now, however, I thinkit is about people who create awareness, stir, <strong>and</strong> build capacity.For me, the whole transition that has been undergone by <strong>Sight</strong><strong>and</strong> <strong>Life</strong>, at least in my lifetime, has built that enthusiasm. Thisis an organization that gets all sorts of things done. Although Ido not believe that there is one single organization that will everwin the battle against malnutrition, <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> plays a reallyimportant role in the whole movement. I have great respect forit because it actually delivers.As for the magazine, it contains articles, inspiring stories, <strong>and</strong>news, <strong>and</strong> its content is strikingly different from what manyother organizations do. I also appreciate that it is not simplyso focused that it’s only interested in its own small area, perhapsbecause it is positioned to be fairly broadly interested inmalnutrition. I get the impression that it’s an organization that’sgenuinely interested in solving issues.SAL: How do you switch off from work? Do you have interestsoutside your professional existence?JJ: Although it’s something that I haven’t done for three or fouryears, I really enjoy fly fishing, as it takes my mind off everything.I also enjoy mountain biking <strong>and</strong> photography. I’m probablysomething of an undercover artist! I can’t do it very well, butI do have the urge to create… I love putting together slide shows,manipulating photographs <strong>and</strong> video editing.SAL: Thank you, Johann, <strong>and</strong> good luck with everything you do.JJ: Thank you.Interview by Susie Lunt
Growingthe evidencebase formicronutrients.
62ewsFourth AfricaNutritional EpidemiologyConference (ANEC 4)Nutrition <strong>and</strong> Food Security:Successes <strong>and</strong> Emerging ChallengesMaffo Tazoho GhislainUniversity of Dschang, CameroonLast year, courtesy of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, I attended the Fourth AfricaNutritional Epidemiology Conference (ANEC 4) on Nutrition <strong>and</strong>Food Security: Successes <strong>and</strong> Emerging Challenges. The five-dayevent took place from October 4 – 8, 2010 in Nairobi, Kenya <strong>and</strong>provided me with an excellent opportunity to share, learn <strong>and</strong>network.security, food availability, food access, food use, food safety,food quality, <strong>and</strong> food utilization.The evidence of the impact of food on health <strong>and</strong> human productivityis well established in infants <strong>and</strong> young children, <strong>and</strong>scientific data shows the impact of malnutrition on infant <strong>and</strong>young children’s growth. Given the complexity of food security,nutritionists, food scientists <strong>and</strong> healthcare workers must worktogether to fight malnutrition in developing countries.Adequate nutrition is key to health<strong>and</strong> general well-beingIn recent decades, nutritional science has clearly demonstratedthe importance of nutrition for health <strong>and</strong> general well-being.Adequate nutrition means when people have access to, <strong>and</strong> consumeenough, food which their body is then able to absorb tomeet all its nutritional requirements. It is a combination of food“ANEC 4 was an importantopportunity for researchers to discussthe best strategy for overcomingmalnutrition in Africa<strong>and</strong> other developing regions”Maffo Tazoho Gislain in front of his poster at the Fourth AfricaNutritional Epidemiology Conference (ANEC), held in Nairobi,Kenya in October 2010
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> FOURTH AFRICA NUTRITIONAL EPIDEMIOLOGY CONFERENCE (ANEC 4) 6363“Attending this outst<strong>and</strong>ing scientificevent was an opportunity to learn <strong>and</strong>be updated on what is happening inthe field of nutrition on a global scale”The Fourth Africa Nutritional Epidemiology Conference wastherefore an important opportunity for researchers to discussthe best strategy to overcome malnutrition <strong>and</strong> promote foodsecurity in Africa <strong>and</strong> other developing regions.As a young researcher, attending this outst<strong>and</strong>ing scientificevent was an important opportunity for me to present the latestfindings from our research group in the area of nutrition <strong>and</strong>food security. It was also an opportunity for me to learn howothers are contributing to this field in their own countries, <strong>and</strong>to be updated on what is happening in the field of nutrition on aglobal scale.The discussion around the theme <strong>and</strong> sub-theme of thisconference was to be instrumental in helping me improve myknowledge of food security, <strong>and</strong> equipping me in better orientingmy efforts to contribute to the fight against malnutrition asan inevitable cause of disease.Participation with fascinating insightsOn Day 1, after registration, I took part in a sponsored preconferencesymposium entitled “Iron interventions in malarious areas:where are we now?” This was followed by the opening ceremony,during which the chair <strong>and</strong> the co-chair of the local organizingcommittee presented their welcome message <strong>and</strong> a summary ofthe co-organizer of the conference, the Africa Nutrition Society(ANS).The following day, I participated in several plenary sessions,including the parallel oral session “Climate change, food security<strong>and</strong> nutrition”. This was followed by a Nestlé symposium <strong>and</strong>a poster session, during which I presented my research work on“Effect of folere juice (dried calyx of Hisbiscus sabdariffa L) onsome biochemical parameters in humans”. The results showedhemoglobin increased significantly (P=0.021), suggesting a potentiallypositive effect of folere juice consumption in increasinghemoglobin concentration. Serum iron, however, decreased(P=0.042), suggesting the utilization of iron in the synthesis ofhemoglobin.The third <strong>and</strong> fourth days brought much, in the form of sessionson “Maternal <strong>and</strong> child heath <strong>and</strong> nutrition”, “Schoolhealth <strong>and</strong> nutrition”, “Nutrition, immunity <strong>and</strong> communicablediseases in developing countries”, “Current management strategiesfor nutritional disorders”, <strong>and</strong> “Nutrition, immunity <strong>and</strong>communicable diseases in developing countries”. There werealso fascinating symposia from Unilever <strong>and</strong> World Vision.Finally, on Day 5, after a couple of plenary sessions focusingon “Nutrition in emergency situations” <strong>and</strong> “ANS capacitybuilding for nutrition in Africa”, I enjoyed the closing ceremonyduring which the Nairobi declaration was read.The week was not all work. A number of social events wereorganized, including a gala dinner at the Nyama Chioma Ranch,during which traditional African music was played, <strong>and</strong> a safariNjema lunch.“My research work showedthe effects of folere juice in humans:increasing hemoglobinbut decreasing serum iron”A valuable visit with future implicationsOverall, the Fourth Africa Nutritional Epidemiology Conferenceenabled me to meet <strong>and</strong> talk with leading scientists <strong>and</strong> expertsin nutrition, as well as other students working in my field of research.I also made many new contacts whom I plan to stay intouch with as I continue my studies – in particular Ngozi Nnamof the University of Nigeria Nsukka, who is working on the samebiological material as me.Such contacts, <strong>and</strong> the knowledge I gained will be translatedto other researchers in my institutions for the scientific developmentof our young university in Cameroon.Correspondence: Mr Ghislain Maffo Tazoho, University ofDschang Department of Biochemistry, Dschang, CameroonE-mail: maghis2006@yahoo.fr
64 THE FIRST GLOBAL CONFERENCE ON BIOFORTIFICATIONReport from theFirst Global Conferenceon BiofortificationHannah GuedenetHarvestPlus, Washington, USAThe First Global Conference on Biofortification was the first in aseries of potentially three biofortification-focused conferencesover the next few years. HarvestPlus convened the conference tobring together the many organizations <strong>and</strong> individuals conductingbiofortification research over the past decade.The conference took place in Washington, DC on November9–11, 2010, attended by 300 scientists, researchers,practitioners, decision-makers, <strong>and</strong> students. Its mainobjectives were to:> determine the current state of biofortification, takingstock of research, global investment, <strong>and</strong> experience in biofortification;> raise the visibility of biofortification as a promising agriculturalintervention for public health; <strong>and</strong>> chart the future for biofortification, identifying synergies<strong>and</strong> gaps in knowledge <strong>and</strong> how to forge partnerships <strong>and</strong>collaborations.“Biofortification, <strong>and</strong> its potentialbenefits to those who aremalnourished, clearly should havea prominent place in our research,in our advocacy, <strong>and</strong> in our globaldevelopment goals”Spanning two <strong>and</strong> half days, it featured a keynote address <strong>and</strong>panel discussion each morning <strong>and</strong> technical symposia in theafternoons. The gala dinner, on the first evening, included biofortifiedmaize on the menu <strong>and</strong> a keynote address by DavidNabarro, Special Representative on Food Security <strong>and</strong> Nutritionto United Nations Secretary-General Ban Ki-moon. The dinneralso featured a letter from Senator George McGovern of the US, astrong supporter of hunger <strong>and</strong> nutrition issues for the past fourdecades, who has shown interest in biofortification. He wrote,“Biofortification, <strong>and</strong> its potential benefits to those who are malnourished,clearly should have a prominent place in our research,in our advocacy, <strong>and</strong> in our global development goals.”Summary of keynote speakersThe conference opened with a keynote address by AmbassadorWilliam Garvelink, US Government Deputy Coordinator for Developmentat the Feed the Future Initiative, who focused hisCredit: Neil Palmer (CIAT)Ambassador William J Garvelink, US Government DeputyCoordinator for Development, Feed the Future: Global Hunger<strong>and</strong> Food Security Initiative, opens the First Global Conferenceon Biofortification, Washington DC, USA
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE FIRST GLOBAL CONFERENCE ON BIOFORTIFICATION 6565remarks on the need to build momentum around linking agriculture<strong>and</strong> nutrition to address food insecurity. While fundingfor agricultural interventions has been on the decline in recentdecades, Ambassador Garvelink reiterated the US Government’srecent commitment to increasing funding for agricultural <strong>and</strong>nutrition interventions, <strong>and</strong> to continuing the advancement ofbiofortified crops.Dr Howarth Bouis, Director of HarvestPlus, presented anoverview of biofortification progress. He identified fivemajor challenges:1. Identifying optimal delivery strategies for gettingbiofortified foods to people;2. Ensuring <strong>and</strong> measuring the public health impactof biofortification;3. Developing a better underst<strong>and</strong>ing of how foodsimpact human nutrition;4. Getting the agricultural sector to prioritize improvingnutrition; <strong>and</strong>5. Getting the nutrition community to prioritize agriculturein order to improve nutrition.Figure 1 shows a proposed framework for establishing biofortificationas a sustainable solution for micronutrient malnutrition.Conference participants were encouraged to provide their feedbackon the framework through an online forum:http://biofortconf.ifpri.info/figure 1: Broad categories for investments to establishbiofortification as a sustainable strategy$ MidstreamBreeding& NutritionResearch (2)$IncreaseBreedingEffectiveness<strong>and</strong> Capacity(5a)Ownershipby AGDecisionMakers (5b)UpstreamResearch (1)Downstream”Pilot“Delivery (3)MeasureImpact (4)Internat.& RegionalAdvocacy (7)$Increase Bioavailability<strong>and</strong> EfficacyEvidence(6a)Ownershipby Nutrition/Public HealthDecisionMakers (6b)Nicholas Kristof, Pulitzer Prize-winning columnist for the NewYork Times, delivered day two’s keynote address. He encouragedparticipants to think about ways to raise the visibility ofmicronutrient malnutrition in the media, by doing a better jobof “selling their story” <strong>and</strong> building emotional connections tothe issues.Navyn Salem from Edesia Global Nutrition Solutions deliveredthe keynote address on day three. She focused on the linkbetween the private <strong>and</strong> public sectors, given Edesia’s work ondelivering ready-to-use therapeutic foods for the treatment ofacute malnutrition. Her comments provided potential strategies“Biofortification must use multipledisciplines <strong>and</strong> channels to promote<strong>and</strong> disseminate crops”on how biofortification must use multiple disciplines <strong>and</strong> channelsto promote <strong>and</strong> disseminate crops.Commissioned papers <strong>and</strong> moderated panel discussionsTwo papers had been commissioned for the conference. The first,From HarvestPlus to harvest driven: How to realize the elusive potentialof agriculture for nutrition? by Lawrence Haddad of theUK’s Institute of Development Studies, focused on how agriculturecan be used, more effectively, to improve nutrition.He answered three questions: 1) What are the pathwaysbetween agriculture <strong>and</strong> nutrition? 2) Is the potential being realized?<strong>and</strong> 3) What can be done to increase the realization ofthis potential? After presenting his paper, Roger Beachy of theUSDA, Shenggen Fan of the International Food Policy Research⇢
66 THE FIRST GLOBAL CONFERENCE ON BIOFORTIFICATIONInstitute, Iain MacGillivray of the Canadian International DevelopmentAgency, <strong>and</strong> Ruth Oniang’o of the African Journal of Food,Agriculture, Nutrition, <strong>and</strong> Development discussed his findings<strong>and</strong> took questions from the audience.Keith West of the Johns Hopkins Bloomberg School of PublicHealth presented the second commissioned paper, Biofortificationas a complementary approach to controlling micronutrientdeficiencies in the developing world. This discussed how biofortificationfits into already existing nutritional strategies of dietarydiversification, food fortification, <strong>and</strong> supplementation.Panelists included Shawn Baker of Helen Keller International,Mahabub Hossain of the Bangladesh Rural Advancement Committee,MG Venkatesh Mannar of Micronutrient Initiative, <strong>and</strong>Meera Shekar of the World Bank.On the final day, Dr Bouis summarized the conference keynotes,panel discussions, <strong>and</strong> symposia, looking back at theframework proposed on day one (Figure 1). A panel discussionfollowed, including Pamela Anderson of the InternationalPotato Center, Arun Joshi of the International Wheat <strong>and</strong> MaizeImprovement Center, Denis Kyetere of the National AgricultureResearch Organisation – Ug<strong>and</strong>a, <strong>and</strong> Francisco Reifschneider ofEmbrapa (Brazil). Panelists discussed ideas for moving biofortificationforward. The conference concluded with a strong callto action by moderator Roger Thurow of the Chicago Council onGlobal Affairs.table 1: The afternoon symposia presented findings on:> Progress, challenges, <strong>and</strong> the way forward in nutrition researchon biofortified crops: vitamin A> Progress, challenges, <strong>and</strong> the way forward in nutrition researchon biofortified crops: iron <strong>and</strong> zinc> Progress, challenges, <strong>and</strong> the way forward in breeding <strong>and</strong> genedevelopment for vitamin A: taking stock, gaps, <strong>and</strong> solutions> Progress, challenges, <strong>and</strong> the way forward in breeding <strong>and</strong> genedevelopment for iron <strong>and</strong> zinc: taking stock, gaps, <strong>and</strong> solutions> Delivering vitamin A crops: a visible nutrient> Delivering iron <strong>and</strong> zinc crops: an invisible nutrient> Biofortification for the developed world: progress withantioxidants <strong>and</strong> other nutrients> Biofortification through agronomic practices> Breeding for bioavailability> Building public trust in transgenic biofortified crops: a dialogue> Climate change <strong>and</strong> the nutritional quality of foods> Orange-fleshed sweet potato is making a difference> Weaving biofortification into the global development agenda> What about protein?Credit: Neil Palmer (CIAT)New York Times columnist Nicholas Kristof during his keynoteaddress on the second day of the First Global Conference onBiofortification, Washington DC, USA.The afternoon symposia (Table 1), featuring the work of 50scientists <strong>and</strong> researchers, focused on the technical aspects ofbreeding, nutrition, <strong>and</strong> delivery of biofortified crops. It also focusedon biofortification through agronomic practices, buildingtrust around transgenic biofortified crops, <strong>and</strong> climate change’srole in diminishing the nutritional quality of foods.Highlights included a session on a recent project that disseminatedorange-fleshed sweet potato to 24,000 householdsin Ug<strong>and</strong>a <strong>and</strong> Mozambique. By researchers from HarvestPlus<strong>and</strong> the International Food Policy Research Institute, this alsopresented strategies used by the project to promote new sweetpotato varieties.All videos, presentations, <strong>and</strong> papers from the conferencecan be downloaded at: http://biofortconf.ifpri.info.http://www.flickr.com/photos/48533839@N05/sets/Correspondence: Hannah Guedenet, HarvestPlus, c/o IFPRI,2033 K Street, NW Washington, DC 20006-1002, USAE-mail: HarvestPlus@cgiar.org
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> NEW DEVELOPMENTS IN CAROTENOIDS RESEARCH 6767New Developmentsin Carotenoids ResearchConference at Tufts University, Boston, USA,11–12 March <strong>2011</strong>Peter EngelDSM Nutritional Products on behalf of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>,Basel, Switzerl<strong>and</strong>IntroductionWith its copious research <strong>and</strong> development (R&D) activities <strong>and</strong>passion for innovation, DSM is an authority on nutrition science,supporting multiple activities dedicated to the field of nutrition.The company regularly brings together scientists from academia<strong>and</strong> industry, as well as experts from health authorities, to communicate<strong>and</strong> advocate for the role of micronutrients in humanhealth. In March <strong>2011</strong>, an international group of leading researchersin the growing field of carotenoids met at Tufts University,Boston, USA, for an information-packed, two-day conference on“New Developments in Carotenoids Research.” Jointly organizedby Tufts University <strong>and</strong> DSM, <strong>and</strong> presented by The Jean MayerUSDA Human Nutrition Research Center on Aging (HNRCA), theconference featured keynotes from global experts on the roleof -carotene, lycopene, lutein <strong>and</strong> zeaxanthin, as well as vitaminA in human health. The about 150 participants experienceda high-level conference where the “Who’s Who” in carotenoid<strong>and</strong> vitamin A science shared latest research findings.DSM is continuing to support carotenoid science events withthe “Macular Carotenoids & AMD” conference in Cambridge,UK (www.macularcarotenoids.org) <strong>and</strong> the “16th InternationalSymposium on Carotenoids” in Krakow, Pol<strong>and</strong> (www.carotenoid.pl).more instances of unnecessary death <strong>and</strong> blindness every year.-carotene is an important, but insufficient source of vitamin Aamong poor populations, which accounts for the widespreadnature of vitamin A deficiency. It has only recently become apparentthat the bioconversion of traditional dietary sources of-carotene to vitamin A is much less efficient than previouslysupposed. The other major carotenoids, particularly lycopene,lutein <strong>and</strong> zeaxanthin, have been found to have important“The use of systematic reviews willbe essential to provide harmonization<strong>and</strong> transparency in the process ofdeveloping intake recommendations”Summary of selected key lecturesIn his keynote lecture, Alfred Sommer (Johns Hopkins University,USA) gave a global clinical overview on vitamin A <strong>and</strong> carotenoids.The clinical importance of vitamin A as an essentialnutrient has become increasingly clear. Adequate vitamin A isrequired for normal organogenesis, immune competence, tissuedifferentiation <strong>and</strong> the visual cycle. Deficiency, widespreadthroughout the developing world, is responsible for a million orCo-Chair, Dr Simin Meydani welcomingeveryone to HNRCA
68 NEW DEVELOPMENTS IN CAROTENOIDS RESEARCHRoundtable discussion from left to right: Rob Russell, Helmut Sies,Cathy Ross, Johannes von Lintig, Marjorie Haskell, Al Sommerbiologic properties, including antioxidant <strong>and</strong> photo-protectiveactivity. In observational studies, high intake of these has beenlinked with the reduced risk of a number of chronic diseases.Focusing on the role of -carotene as a safe source for vitaminA, Robert M Russell (National Institutes of Health, USA)gave perspectives on vitamin A <strong>and</strong> carotenes with regard todefining their dietary requirements. In 2001, the old ratio of 6:1-carotene to vitamin A equivalence (1 retinol equivalent = 6 μgof -carotene) was jettisoned in the US for a new ratio of 12:1,based on new <strong>and</strong> reproducible stable isotope data. However,there is great variation of the bioconversion equivalence, dependingon the food being tested (e.g., for green leafy vegetables>20:1 <strong>and</strong> for carrots ~15:1). In addition, there is new evidencethat foods with a simple, digestible matrix have an equivalencethat is much better than 12:1. The tolerable upper level for vitaminA is set at 3,000 μg per day in the US <strong>and</strong> EU, based uponliver toxicity <strong>and</strong> teratogenicity among women of reproductiveage. In the UK, it is recommended that people not consumemore than 1,500 μg per day. The US <strong>and</strong> EU panels concludedthat there was not enough data on which to base a tolerableupper level for -carotene. However, in the UK an upper levelfor -carotene was set at 7 mg per day. In future, the use ofsystematic reviews will be essential to provide harmonization<strong>and</strong> transparency in the process of developing intake recommendations.chronically insufficient in meeting needs imposed by life stage,infection <strong>and</strong> other metabolic stresses. Preventing such deficiencycan be achieved through an adequate diet of preformed(e.g., liver, dairy products, egg, etc) <strong>and</strong> provitamin A carotenoidfood sources (e.g., dark green leaves, yellow-orange fruits <strong>and</strong>vegetables). Dietary -carotene is the most important precursorof vitamin A <strong>and</strong> has the potential to fill dietary vitamin A gaps.The challenge in attaining nutritional adequacy for vitamin A<strong>and</strong> -carotene was discussed by Marjorie J Haskell (Universityof California, USA). The bioavailability <strong>and</strong> vitamin A equivalencyof -carotene from foods is highly variable <strong>and</strong> can be affectedby food <strong>and</strong> diet-related factors (such as the food matrix,food processing techniques) <strong>and</strong> also by characteristics of thetarget population, such as vitamin A status, other nutrient deficiencies,gut integrity <strong>and</strong> genetic polymorphisms associatedwith -carotene metabolism. Thus, the variability in estimatesof vitamin A equivalency is high across studies, as is the variabilityin vitamin A equivalency ratios between individuals withinstudies. Hans Konrad Biesalski (University of Hohenheim, Germany)emphasized that consensus among experts in the field ofcarotenoids holds that -carotene is a safe source of vitamin A“Retinoids influence, <strong>and</strong> in somecases appear to be principal driversof, immune cell differentiation that, inturn, affects a number of processes”Nutritional relevance <strong>and</strong> challengesKeith P West (Johns Hopkins Bloomberg School of Public Health,USA) outlined the nutritional relevance of -carotene as provitaminA. Vitamin A deficiency can arise when dietary intake isListening intently from left to right Yoav Sharoni, Adrian Wyss,Georg Lietz, Johannes von Lintig, Catherine Ross
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> NEW DEVELOPMENTS IN CAROTENOIDS RESEARCH 6969expert key messages-caroteneLuteinZeaxanthinLycopeneis a safe source of vitamin A. Its pro-vitamin A function is a crucial contribution to the required totalvitamin A intake in both developed <strong>and</strong> developing countries. Vitamin A is essential for normal growth <strong>and</strong>development, the immune system, vision <strong>and</strong> other functions in the human body. The intake of preformedvitamin A from animal products is not sufficient in major parts of the population all over the world, includingEurope, the US <strong>and</strong> Asia. Recent studies suggest that suboptimal levels of vitamin A <strong>and</strong> -carotene, evenlevels well above those causing clinical defi ciency syndromes, can be a contributing risk factor in chronicdiseases. An appropriate intake of -carotene in diets, forti fied foods <strong>and</strong>/or dietary supplements couldsafely compensate for the lack of vitamin A.is a natural pigment <strong>and</strong> potent antioxidant present in the macula of the eye <strong>and</strong> in the skin. It acts as afilter, shielding against the damaging near-to-UV blue light of the sun. Higher dietary intake of foods rich inlutein <strong>and</strong> zeaxanthin is being discussed for its potentially positive, preventive effects on macular degeneration<strong>and</strong> cataracts, as well as improved visual performance. Based on a wealth of scienti fic literature, luteinis considered an eye health nutrient, supporting healthy eyes <strong>and</strong> vision as people age.is, in addition to lutein, the only other major carotenoid specifically located in the macula of the eye.Zeaxanthin, found in the retina, also protects the eye from damage caused by the near-to-UV blue light of thesun. Higher dietary intake of foods rich in lutein <strong>and</strong> zeaxanthin has been associated with a reduced risk ofmacular degeneration <strong>and</strong> cataracts.is one of the strongest antioxidants among the carotenoids. Scientifi c evidence suggests that lycopene helpsprotect cells against oxidative damage, <strong>and</strong> it is discussed <strong>and</strong> researched in the scienti fic community for itsbenefi ts to cardiovascular health.intake, <strong>and</strong> that the provitamin A function of -carotene is essentialto achieve vitamin A intake recommendations in bothdeveloped <strong>and</strong> developing countries.Summarizing the results of epidemiological <strong>and</strong> human supplementationstudies with -carotene in chronic disease prevention,Susan T Mayne (Yale Schools of Public Health <strong>and</strong> Medicine,USA) concluded that intervening in populations with low-carotene status in order to improve it may be a more promisingapproach than intervening in populations with adequatestatus in order to raise it to a “supra” adequate status. However,this more personalized approach to nutrient-based interventionis critically dependent on the availability of biological markersof status – in this case, carotenoid status. Recent advances inthe development of promising new methods for rapidly <strong>and</strong> noninvasivelyassessing carotenoid status suggest that it is increasinglyfeasible to identify the persons most likely to benefit fromcarotenoid interventions, allowing for future intervention trialswith a greater likelihood of demonstrating beneficial effects thanseen to date.L<strong>and</strong>mark findingsFrancine Grodstein (Harvard Medical School, USA) reported onclinical studies evaluating the effect of antioxidant -carotenesupplements on cognitive decline in older persons. Most notably,in the Physicians’ Health Study II 6,000 older men were r<strong>and</strong>omizedto 50 mg of -carotene supplementation on alternatedays, ranging from one to up to 18 years. For participants withlong-term supplementation, cognitive function was significantlybetter compared to long-term placebo. Other research in thisarea has been inconsistent with these l<strong>and</strong>mark findings. Theexplanation for these discrepant findings is not clear, although itis possible that some combination of the appropriate dose <strong>and</strong>
70 NEW DEVELOPMENTS IN CAROTENOIDS RESEARCHduration of -carotene exposure is necessary for brain health.Future research needs to better consider these questions of dose<strong>and</strong> duration.Study results showing -carotene- <strong>and</strong> lycopene-rich diet orsupplementation to provide protection against skin damage fromsunlight were presented by Helmut Sies (Heinrich Heine University,Germany). Although photoprotection through individualcarotenoid intake is considerably lower than that achieved usingtopical sunscreens, optimal supply of antioxidant micronutrientsto the skin increases basal dermal defense against UVirradiation, supports longer-term protection <strong>and</strong> contributes tothe maintenance of skin health <strong>and</strong> appearance.In a second keynote lecture, A Catharine Ross (PennsylvaniaState University, USA) comprehensively outlined the effects ofvitamin A <strong>and</strong> retinoic acid on the immune system. Retinoidsinfluence, <strong>and</strong> in some cases appear to be principal drivers of,immune cell differentiation that, in turn, affects a number ofprocesses. Vitamin A’s active metabolite all-trans-retinoic acidseems to exert effects on the immune system by heighteningantibody responses through promotion of antibody production,regulating T-cell differentiation, <strong>and</strong> programming precursorT cells for innate immunity. In addition, the retinoic acid induciblegene-1 is a major factor in the response to viral infections<strong>and</strong> other stimuli.The lycopene effectXiang-Dong Wang (Tufts University, USA) discussed the importanceof lycopene for human health. A high intake of tomatoes<strong>and</strong> tomato products have been found to reduce the risk of certainchronic diseases in many epidemiological studies, yieldingevidence that lycopene (a major carotenoid in tomatoes) is amicronutrient with important health benefits, such as chronicdisease prevention (e.g., various types of cancer). Whether theeffect of lycopene on various cellular functions <strong>and</strong> signalingpathways is a result of the direct actions of intact lycopene orits derivatives remains unknown. Steven K Clinton (Ohio StateUniversity, USA) noted that epidemiologic studies suggest lycopeneas a way to reduce risk or slow the progression of prostatecancer. Human studies focus upon the distribution of lycopeneto the human prostate <strong>and</strong> the potential impact upon biomarkersrelated to prostate cancer progression.Paul S Bernstein (University of Utah, USA) elucidated the roleof macular pigment carotenoids. Abundant epidemiological evidencesuggests that the macular pigment carotenoids lutein <strong>and</strong>zeaxanthin play key roles in the prevention <strong>and</strong> treatment of agerelatedmacular degeneration (AMD), a leading cause of irreversiblevisual loss in the elderly in the developing world. Evidencethat lutein <strong>and</strong> zeaxanthin also seem to improve visual performancein healthy subjects was highlighted by B R<strong>and</strong>y Hammond(University of Georgia, USA). Finally, Elizabeth J Johnson (TuftsUniversity, USA) reviewed these carotenoids’ effects on cognitiveperformance in older adults: Cognitive decline in the elderlyis a significant public health issue. Oxidative stress <strong>and</strong> inflammationare believed to be involved in the pathogenesis of cognitivedecline. Epidemiological studies suggest that intake ofdietary carotenoids may be of benefit in maintaining cognitivehealth. Given their role as antioxidants <strong>and</strong> anti-inflammatoryagents, lutein <strong>and</strong> zeaxanthin may play a role in the preventionor delay of cognitive decline. Among all of the carotenoids, onlythese two cross the blood-retina barrier to form macular pigmentin the eye.Correspondence: Peter Engel, Scientific Communications,Human Nutrition <strong>and</strong> Health, DSM Nutritional Products Ltd,PO Box 2676, 4002 Basel, Switzerl<strong>and</strong>E-mail: peter.engel@dsm.com
Promotingpartnerships<strong>and</strong> capacitybuilding.
72Reportfrom GogounouBlessings at the I-DomarouHealth CenterPhilippe Bani MoraDomarou Health Centre, Gogounou, BeninOne of the Millennium Development Goals is to reduce the childmortality rate via people’s access to primary healthcare. Withthis in mind, in April 2010 the I-Domarou health care center wasestablished in Gogounou, thanks to financial support from ourfaithful partner <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>. The center’s fame quickly spread<strong>and</strong> it soon set consultation records for the whole community.I-Domarou, which means blessings in the local language, iscompetitive in terms of its quality of care, affordability <strong>and</strong> hospitality.Providing a full range of care, it is run by three people,including a senior public health technician/nutritionist, whoalso acts as center manager; a social assistant; <strong>and</strong> a caregivertrained at the center.Nutritional, preventative <strong>and</strong> educational workNutritional recovery is made on the basis of a “food square” consistingof a source of cereal (starch or tuber); a source of protein(vegetable or animal); a source of mineral complexes <strong>and</strong> vita-Curative workI-Domarou is an integrated health center <strong>and</strong> its activities arepatient-driven. Cases include childhood illnesses, nutritionaldiseases, <strong>and</strong> many others, including skin infections, cuts, injuries<strong>and</strong> deficiencies in micronutrients. The center initiallytreated 328 cases in April 2010; however, numbers have risen<strong>and</strong> a gr<strong>and</strong> total of 2,927 patients were seen over a period ofsix months. At a community level, the center received 150 patientswhose parents did not even have one franc to support theirchildren – most of whom were seriously ill. It also received fourorphans <strong>and</strong> assisted with their medical care. In addition, it hasseen 10 cases of night blindness.Philippe Bani Mora, manager of the Domarou Health Centre,Gogounou, Benin, established in 2010 with the financial supportof <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> REPORT FROM GOGOUNOU 7373mins (dried Moringa leaves); <strong>and</strong> an energy supplement (sugaror oil). The center is in contact with Niger’s Office of PharmaceuticalProducts, which provides it with chocolate products rich invitamins <strong>and</strong> minerals. It also carries out minor surgery, such assuturing wounds, draining abscesses <strong>and</strong> applying b<strong>and</strong>aging.We raise awareness about various topics, from the importanceof exclusive breastfeeding, best weaning practices, foodsupplements <strong>and</strong> vaccinations to the need to monitor childrenfor a healthy infancy. The center also distributes vitamin A tovulnerable groups <strong>and</strong> home visits are arranged.In future, the center might grow to include a laboratory. However,the need for maternity facilities is also evident <strong>and</strong> mother <strong>and</strong>child protection is in great dem<strong>and</strong>. Prenatal consultation <strong>and</strong>pregnancy monitoring could be carried out in liaison with thearea hospital. We need to increase staff with qualified personnel<strong>and</strong> to obtain a means of transport to enable us to raise awarenessin Fula camps <strong>and</strong> settlements far from the town center <strong>and</strong>ensure the transportation of medication from the central vendorto our remote workstation 175 km away.Progress <strong>and</strong> prospectsSince its inception, we have made good progress in a numberof areas, ranging from collaboration with the state structure tocooperation with the commune’s elected officials. We have submittedan application to the town hall for more l<strong>and</strong>, to enablethe future expansion of the center, including the constructionof a clinic.Correspondence: Philippe Bani Mora,Domarou Health Centre, Gogounou Alibori Department, BeninE-mail: banimorap@yahoo.fr“An integratedhealth centerwith patient-drivenactivities”
74 REPORT FROM KATHMANDUReportfrom Kathm<strong>and</strong>uA Project Report on Training of AdolescentGirls for Prevention <strong>and</strong> Control of Iron DeficiencyAnemia 2009/10Utpal ChaliseYouth Volunteer Group,Kathm<strong>and</strong>u, NepalThe continuation of a previous projectsupported by <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>This is the final report on the training of adolescent girls workingin the mining <strong>and</strong> stone quarrying industries in rural hillyareas of eastern Nepal, in the prevention <strong>and</strong> control of anemia.This activity was implemented in different locations withinKavrepalanchok district to create awareness among mine <strong>and</strong>quarry workers. In order to do so <strong>and</strong> bring taught subjects tolife, adolescent girls from different locations were first trained toidentify people with iron deficiency anemia (IDA), provide nutritioneducation, <strong>and</strong> change behavior in terms of utilizing existinghealth care service centers early on. After training, during theirleisure time these adolescent girls were involved in identifyingIDA among pregnant women, nursing mothers <strong>and</strong> adolescentgirls, in order to achieve the stated objectives for the periodof 10 months to compare the results of IDA prevalence amongthese high-risk populations. This project is part of a continuationof a previous project supported by <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>.Project rationaleIDA is the most common nutritional problem in Nepal <strong>and</strong> hasprofound economic <strong>and</strong> social consequences. Many activitieshave been implemented by different organizations to combatthis. However, some groups or pockets of the population havesignificant problems <strong>and</strong> still need to be reached with specialpackages.Adolescent girls who are employed in the mines <strong>and</strong> stonequarries of rural eastern Nepal are being trained to identifypeople with anemianot aware of the problem <strong>and</strong> do not utilize available healthcare facilities. More attention needs to be paid to them to reducethe existing burden of IDA.> As the government does not have a program to reach thesegroups, there is a strong need for regular outreach health careactivities. One-off activities do not help reduce the presentproblem.> Mine <strong>and</strong> quarry owners need to support regular healthcheck-ups, <strong>and</strong> the provision of nutritious food, especially forpregnant <strong>and</strong> nursing mothers. Currently, whenever someonewants a check-up, he or she loses pay. Leave facilities shouldtherefore be provided when health check-ups are required.> Specific target groups require extra efforts <strong>and</strong> therefore needspecial attention.> Although mine <strong>and</strong> stone quarry workers live in communitiesthat are comparatively similar, it has been found that they are
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> REPORT FROM KATHMANDU 7575table 1: IDA in the first health check camptable 2: IDA in the second health check campDescription No. examined IDA detected %Description No. examined IDA detected %Pregnant women 64 27 42.2Nursing mothers 52 17 32.7Adolescent girls 80 24 30.0Pregnant women 57 11 19.3Nursing mothers 48 9 18.8Adolescent girls 86 16 18.6Overall objectiveTo create awareness of the consequences of micronutrient deficiencies,with a special focus on iron deficiency anemia amongpregnant <strong>and</strong> lactating mothers <strong>and</strong> adolescent girls of reproductiveage working as mine <strong>and</strong> stone quarry workers.Specific objectives> Organize one batch of peer educator training for 25 adolescentgirls at different mining <strong>and</strong> stone quarrying work sites.> Identify, keep records of <strong>and</strong> treat pregnant women, lactatingmothers, <strong>and</strong> adolescent girls of reproductive age with IDA.> Raise awareness of the need for <strong>and</strong> importance of iron supplementationfor pregnant women, lactating mothers, <strong>and</strong>adolescent girls of reproductive age.> Raise awareness among pregnant women of the importance ofiron supplementation during pregnancy.> Motivate pregnant women to take iron-coated tablets regularlyduring pregnancy.> Create awareness among pregnant women, lactating mothers,<strong>and</strong> adolescent girls of reproductive age about the importanceof daily, sufficient consumption of foods containing vitamin A<strong>and</strong> iron <strong>and</strong> the importance of vitamin C rich food to increasedietary iron absorption.The activity was implemented at 10 different locations in Kavrepalanchokdistrict, 46 km from central Kathm<strong>and</strong>u, the Nepalesecapital. The majority of people in the project areas are from specialethnic, marginalized, socio-economically poor <strong>and</strong> underprivilegedgroups. Three hundred <strong>and</strong> twenty-four families, or2,231 people, were covered of whom 1,530 were mine <strong>and</strong> stonequarry workers <strong>and</strong> the remaining 701 from a village near thework site.AchievementTwo meetings were conducted with those in charge of healthposts, female community health volunteers (FCHVs), socialworkers, <strong>and</strong> NGO representatives in program areas.Two general health check-up camps were held at the beginning<strong>and</strong> end of the 10-month period for all quarry <strong>and</strong> mineworkers’ family members <strong>and</strong> people from the community, witha special focus on pregnant women, lactating mothers, <strong>and</strong> adolescentgirls. Health check-up camps to detect IDA among thetarget groups were organized at the work place at 10 sites tomake them accessible <strong>and</strong> save workers’ time, so that they couldreturn to work quickly.The heart of the program was to identify <strong>and</strong> train adolescentgirls from among the quarry <strong>and</strong> mine workers <strong>and</strong> developthem as motivators to early identify people with IDA <strong>and</strong> referthem to nearby health care units for treatment, followed bynutritional education. The prevalence of IDA is summarized inTables 1 <strong>and</strong> 2.Nutrition educationAfter the selection process, three-day nutrition orientation trainingwas organized. It focused on the magnitude of the problem,the target group, nutrition deficiency disorders, early identificationof problems, selection <strong>and</strong> preparation of foods, timely useof available health care units, etc.Health check-ups are held at the beginning <strong>and</strong> end ofa 10-month period for all quarry- <strong>and</strong> mine-workers’ familymembers <strong>and</strong> people from the community⇢
76 REPORT FROM KATHMANDUPregnant women <strong>and</strong> nursing mothers are identified to visithealth care units <strong>and</strong> adopt preventive measuresRecords of existing health care units have shown that thoseadolescent girls, pregnant women, <strong>and</strong> nursing mothers referred<strong>and</strong> detected as having IDA have been found to have visited thehealth units. Pregnant women <strong>and</strong> nursing mothers have beenfound to have adopted preventive measures as suggested, <strong>and</strong>improved the practice of planning <strong>and</strong> consuming iron-richfoods. Vitamin A capsules were distributed at all 10 sites, <strong>and</strong>100 percent of children aged 6 – 59 months received vitamin Acapsules. This was mainly thanks to the trained adolescent girls,aided by female community health volunteers who visited eachhouse. However, the majority of the target groups did not utilizethe health care units as expected, despite regular motivation bytrained persons. This was mainly for fear of losing their dailywages. Making the service accessible <strong>and</strong> providing regular motivationby family members can help reduce the problem of IDAin such target populations.Each trainee was provided with a kit bag containing a recordbook to record details of people with nutritional anemia <strong>and</strong> vitamindeficiency disorders, nutrition posters, iron tablets, <strong>and</strong>referral slips. As a preventive measure for the whole target population,nutrition education was delivered with the help of pictorialprinted materials.Trained adolescent girls took responsibility in their respectiveworkplaces <strong>and</strong> health educators delivered nutrition educationto a group every two months. Due consideration was givento the importance of micronutrient supplements for safe delivery,safe motherhood, prevention <strong>and</strong> control of childhood blindness,<strong>and</strong> mortality. Nursing mothers were encouraged to breastfeedtheir children up to at least two years of age, <strong>and</strong> to feed childrenfood rich in iron <strong>and</strong> vitamin A from six months.Correspondence: Uptal Chalise, Youth Volunteer Group,c/o GPO Box 1144 Kathm<strong>and</strong>u, Banepa, Kavrepalanchok, NepalE-mail: vg87@hotmail.com“IDA is the mostcommon nutritionalproblem in Nepal”
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> REPORT FROM LEMBA 7777Report from LembaCentre de Lutte Contre la Malnutrition de LembaGeorges Nicks TsimbaBoma, Bas-CongoAnne-Catherine Frey<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, Switzerl<strong>and</strong>Strategies for proper diagnosisWe were then in a position to diagnose <strong>and</strong> treat. Two strategieswere used to ensure proper diagnosis: door-to-door visits <strong>and</strong>diagnosis at community sites. Several diagnostic materials wereused (anthropometric kit) <strong>and</strong> we diagnosed 342 cases of malnutrition.Once diagnosed, three courses of action were taken.The Centre de Lutte Contre la Malnutrition de Lemba (Center forthe Fight Against Malnutrition in Lemba) is located on avenueMambu N°20, in the settlement of Kinsundi-Lemba, Bas-Congoprovince. It is 40 km from the port town of Boma in the southwest of the Democratic Republic of Congo <strong>and</strong> 540 km fromKinshasa. The settlement of Kinsundi-Lemba is home to 21,935inhabitants including 3,729 children aged up to 59 months. Themajority of the population farms, while the remainder is madeup of traders, teachers, craftsmen <strong>and</strong> the unemployed.The creation of the center began on September 11, 2009 onthe initiative of Georges Nicks Tsimba, senior ophthalmologist<strong>and</strong> nutritionist at the NGO Foyer d’Encadrement pour le DéveloppementFED-ASBL. He had the excellent idea to set up a healthfacility to combat malnutrition <strong>and</strong> its effects on vulnerable people(children <strong>and</strong> others).Dietary treatment: First, we needed food. Since our center islocated in a farming area, we carried out a survey to find out whichfoodstuffs are most commonly consumed <strong>and</strong> how, as well as themethods of producing them. From the results, we determined thebest foodstuffs to be consumed. A parallel study was conductedto identify the components <strong>and</strong> nutritional values of each foodstuff,with most having been processed into flour, juice or pulp. Thesewere mixed to increase the nutritional strength, then packaged <strong>and</strong>stored. Treatment depended on the degree of malnutrition.Medical treatment: Consisting of vitamin A, folic acid, Vermox,Amoxicillin, <strong>and</strong> eye <strong>and</strong> dental products.Preventative treatment: Including nutritional educationabout exclusive breastfeeding, feeding a sick child, food hygiene,culinary principles <strong>and</strong> personal hygiene, <strong>and</strong> teachingmothers about vegetable growing.A year of actionFrom September 11, 2009 to September 11, 2010 there was anextensive program of activities.The training of community liaison staff was the first task tobe carried out, since it enabled us to gain the facilities to raisepeople’s awareness about malnutrition, micronutrients <strong>and</strong> nutritionalanemia. We trained five community liaison staff: threemen <strong>and</strong> two women.Taking into account the difficult access to the most remotevillages, we then created three diagnostic sites. Each of thesehas a representative to deal with cases of malnutrition.A need to raise awareness followed <strong>and</strong> was addressed bymaking use of the community liaison staff as well as posters,radio <strong>and</strong> word of mouth.The challengesNumerous problems were encountered, including difficulties inaccessing people, solid meals given to parents of sick childrenbeing consumed by the whole family, seasonal food out of stock,untimely power cuts, lack of transport, rental difficulties <strong>and</strong> insufficientfunds.Despite this, the center achieved most of its goals, with fivestaff trained, four sites created, 36 visits undertaken <strong>and</strong> 342children diagnosed <strong>and</strong> treated. All this was assisted in part bythe US $6,600 that was received from <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>.Correspondence: Georges Nicks Tsimba,BP 111 Boma, Bas-Congo E-mail: georgesnickst@yahoo.frAnne-Catherine Frey <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>, Basel, Switzerl<strong>and</strong>E-mail: Anne-Cath.Frey@sight<strong>and</strong>life.org
78 REPORT FROM RATANAKKIRIReport from RatanakkiriSchool Health WatchJanie Rose Ilustre,Pen Sarouen <strong>and</strong> Kim Chhay SotheavyVoluntary Service Overseas,CambodiaThe School Health Watch government-initiated project provideshealth <strong>and</strong> nutrition guardianship in schools, <strong>and</strong> aims to targetthe prevention, treatment <strong>and</strong> control of health <strong>and</strong> nutritionproblems among school children.The province of Ratanakkiri, in northeast Cambodia, clearlyillustrates a higher prevalence in malnutrition, in comparisonwith the data of malnutrition for the entire country (see Table 1).It is for this reason that the School Health Watch project wasinitiated.table 1: Cambodian Demographic <strong>and</strong> Health Survey (CDHS)(children 6–59 months old)Anthropometrics Cambodia RatanakirriStunted 37% 54%Underweight 36% 52%Wasting 7% 8%2005; National Institute of Public Health <strong>and</strong>National Institute of Statistics.The problems of undernutrition remain particularly severe incountries recovering from recent wars <strong>and</strong> civil unrest, whereimprovements in economic conditions tend to benefit the advantagedgroups <strong>and</strong> result in widespread inequalities. Also, inCambodia, after the tragedy of losing millions of children, women<strong>and</strong> men in the “killing fields”, the lack of people to attendthe physical <strong>and</strong> overall wellness of the children aggravated thesituation, <strong>and</strong> the country is still engaged in mobilizing resourcesto rebuild <strong>and</strong> strengthen its society.School Health Watch was conceptualized in order to assess thehealth <strong>and</strong> nutrition status of school children <strong>and</strong> provide interventionsfor prevention <strong>and</strong> control by building the capacityof teachers <strong>and</strong> parents, <strong>and</strong> strengthening its linkages. Theproject’s aim is to improve the quality of health <strong>and</strong> nutritionalstatus of primary school children through early <strong>and</strong> proper diagnosis,treatment <strong>and</strong> prevention interventions in schools.Ground-breaking changesAfter the implementation of the project, a Health <strong>and</strong> NutritionManual was developed to serve as reference material <strong>and</strong> nationaltrainers from the School Health Department were identifiedas core trainers for possible expansion in future.A total of 70 primary school teachers from five differentschools were trained in health <strong>and</strong> nutrition skills <strong>and</strong> the knowledgeto implement the project effectively. In addition, eachschool received water filters, first aid kits, hygiene sets, weighingscales, <strong>and</strong> height boards.Anthropometric data on 1,572 primary school children wererecorded. The results revealed that 23.2% were severely underweight;62.8% were moderately underweight; <strong>and</strong> 14% weremildly underweight. Two hundred <strong>and</strong> fifty malnourished childrenwere therefore identified to receive 15-day supplementalfeeding, <strong>and</strong> among them 176 showed significant improvement(70.4%). Furthermore, the parents of these children attended anutrition orientation workshop to ensure continued rehabilitationat home. The Ministry of Education, Youth <strong>and</strong> Sport rectifiedthe School Health Policy Guidelines that were developed toensure the sustainability <strong>and</strong> adaptability of the project amonginterested partners <strong>and</strong> stakeholders. To date, the project hasbecome a successful benchmark for other partners. Belgium’sH<strong>and</strong>icapped International supported a rolling-out of the projectin two of their targeted provinces in Takeo <strong>and</strong> Battambang,Cambodia, <strong>and</strong> the World Food Programme has shown an interest,with initial discussions taking place.Correspondence: Janie Rose Ilustre, Pen Sarouen <strong>and</strong>Kim Chhay Sotheavy, Voluntary Service Overseas, Cambodia,School Health Department, Ministry of Education, Youth <strong>and</strong>Sports, Cambodia E-mail: jrilustre@hotmail.com
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> REPORT FROM RATANAKKIRI 7979Cambodia is engaged in mobilizing resources to strengthen <strong>and</strong> rebuild its society,including the health <strong>and</strong> nutritional status of its schoolchildren“The project has becomea successful benchmarkfor other partners”
80nd <strong>Life</strong> Special Research Grant 2010 Awarded01l For <strong>2011</strong> GrantThe theme for the 2010 <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> Special Research Grantwas “Assessing vitamin A dietary intake <strong>and</strong> status in developingcountries where fortified foods are commercially available.”Seventeen applications were received <strong>and</strong> two groupsof researchers were selected. The first grant was awarded tothe South African Medical Research Council (MRC), underthe aegis of lead researcher Dr Mieke Faber. The research willdetermine the vitamin A intake <strong>and</strong> status of a representativesample of r<strong>and</strong>omly selected South African children agedtwo to five years <strong>and</strong> their caregivers in each of five diversegeographical sites. The second grant was awarded to theUniversity of California, Davis, <strong>and</strong> Helen Keller International,Cameroon, with the lead researcher being Dr Kenneth Brown.The theme of the research is “Vitamin A fortification02N Keeps on RisingSpeakers from the 1,000 Days conference join Mr Shah,USAID administratorof refined cooking oil in Cameroon: Optimization of fortificationlevels using dietary intake data <strong>and</strong> use of biologicalindicators of vitamin A status for program impact evaluation.”We look forward to sharing the results from both researchprograms.The <strong>2011</strong> Special Grant theme will be “Examining theoptimal formulation of micronutrient powders <strong>and</strong> the effectof their use on anemia, micronutrient status, <strong>and</strong> physicalgrowth in malaria endemic settings.”For details on the theme <strong>and</strong> how to apply, visitwww.sight<strong>and</strong>life.orgThe nutrition world is abuzz with activity as, now that boththe Framework <strong>and</strong> the Road Map have been developed, theScaling Up Nutrition (SUN) process moves from its talk phaseto its action phase. The SUN concept has been reinforcedby political interest in nutrition among leaders of nationalgovernments <strong>and</strong> development partners alike – some 14 countrieshave already been enlisted as “Early Risers”. However,there is still much work to be done. In <strong>2011</strong>, the focuswill be on translating the Road Map into actions with a viewto helping countries affected by malnutrition to achieve longtermreduction in undernutrition, realize the first MillenniumDevelopment Goal, <strong>and</strong> start demonstrating this impactwithin three years.The ongoing development of SUN is being led by a TransitionTeam <strong>and</strong> six inter-linked Task Forces, while the overall
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW81process is chaired by Dr David Nabarro the Special Representativeof the UN Secretary General for Food Security <strong>and</strong> Nutrition.The three principlesguiding the SUN movement are:1. Efforts are led from countries <strong>and</strong> external supportprocesses must add value to this country-led action <strong>and</strong>must be dem<strong>and</strong>-driven;2. Ongoing initiatives to improve nutrition should be linkedtogether for greater coherence, efficiency, <strong>and</strong> impactwherever possible; <strong>and</strong>3. A combination of networks <strong>and</strong> movements are needed toenable a range of stakeholders to work together <strong>and</strong>contribute to lasting results.The Transition Team is made up of <strong>and</strong> working closelywith individuals from the UN’s St<strong>and</strong>ing Committee on Nutrition(SCN) <strong>and</strong> a wide range of organizations that includesthe FAO, UNICEF, WHO, WFP <strong>and</strong> the World Bank, the REACHinitiative, the African <strong>and</strong> European Unions, other regionalbodies, civil society, farmers’ organizations, the research community,private companies, development partners <strong>and</strong> philanthropicfoundations. The Transition Team is focusing onarrangements through which national authorities can request,<strong>and</strong> then access, support for actions to Scale Up Nutrition.The team has begun to consider how best to ensure that supportis responsive to country needs <strong>and</strong> requests, coordinated,of high technical quality <strong>and</strong> effective.Four outcomes are being pursuedby the Transition Team:1. Rapid increase in support for “Early Riser” countries thatseek immediate help with their efforts to Scale Up Nutritionthrough encouraging links between the national authoritiesthat want to get going now <strong>and</strong> those development partnersthat are ready to help them. This support will take stockof existing efforts <strong>and</strong> implementation gaps <strong>and</strong> willfacilitate the development (or strengthening) of nationalmulti-stakeholder nutrition platforms.2. Ensure the development of long-term systems that providesupport to Scaling Up Nutrition in all countries affectedby undernutrition. These systems will enable nationalauthorities to better connect <strong>and</strong> engage with key nutritionstakeholders from both civil society <strong>and</strong> the private sector,in ways that are effective, credible <strong>and</strong> accountable.3. Foster the SUN Movement with effective advocacy <strong>and</strong> leadership.A durable multi-audience advocacy campaign willbe built that encourages the emergence of effective<strong>and</strong> self-sustaining nutrition leadership at community,national, regional <strong>and</strong> global levels. The accomplishmentsof the SUN movement throughout its first three years <strong>and</strong>beyond will be documented <strong>and</strong> communicated, in closecoordination with the 1,000 Days movement.4. Agreement on transparent <strong>and</strong> accountable institutionalarrangements for the SUN effort, once the Transition Teamhas completed its work. This will require analysis of neededfeatures, organizational arrangements, <strong>and</strong> availableoptions. It is intended that countries will be engaged as fullpartners <strong>and</strong> that key stakeholders wishing to contributeto country-led SUN actions will be able to do so. This workis being taken forward in conjunction with efforts toreform the SCN.Each of the six Task Forces is responsiblefor the development of more detailed aspects ofgiving SUN life <strong>and</strong> cover:> Task Force A: Country capability development. Thisfocuses on developing <strong>and</strong> strengthening country capabilitiesfor Scaling Up Nutrition. It includes the provision of supportto multi-stakeholder platforms, the development of managementsystems <strong>and</strong> increased access to knowledge, st<strong>and</strong>ards<strong>and</strong> harmonized policies.> Task Force B: Communication for Scaling Up Nutrition. Thisis responsible for communications <strong>and</strong> advocacy for ScalingUp Nutrition, with the 1,000 Days movement at its core. TheTask Force also encourages the emergence of “Nutrition Leaders”at community, national, regional <strong>and</strong> global levels.> Task Force C: Civil society participation. The focus is on waysto ensure inclusive civil society participation in the SUNprocess, at local, country, regional <strong>and</strong> global levels, ensuringthe rights <strong>and</strong> well-being of those at risk of malnutrition <strong>and</strong>promoting the accountability of decision makers.> Task Force D: Engagement of development partners. Developingways in which development partners, includingbilateral agencies, development banks <strong>and</strong> philanthropic organizations,can be fully engaged in a coordinated response<strong>and</strong> the effort to Scale Up Nutrition <strong>and</strong> can takea leading role in work with national governments.> Task Force E: Engagement of the business community. Workingon ways in which the business community can be betterengaged in the effort to Scale Up Nutrition at all levels inways that have the potential to be sustainable,<strong>and</strong> explore market-based responses at a national level.> Task Force F: Monitoring <strong>and</strong> reporting on in-countryprogress. This focuses on multi-country <strong>and</strong> multi-stakeholderaction to monitor <strong>and</strong> report on progress on Scaling UpNutrition at country level; working with authorities<strong>and</strong> with the other Task Forces identifying the need for moreeffective approaches that could be the subject ofin-depth analysis.
82 WHAT'S NEWEach Task Force is finalizing its specific terms of referenceas well as an action plan <strong>and</strong> many are doing this at the sametime as beginning to deliver on specific projects.<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> is represented on Task Force B by Jane Badham.We will ensure that we give regular updates on the variousSUN activities, as its aim is to be transparent <strong>and</strong> include asmany stakeholders as possible.SUN is currently consolidating <strong>and</strong> building stakeholderalliances <strong>and</strong> aligning donor commitments with country-ledplans for improving nutrition. In a recent article by DavidPelletier et al, published in Health Policy <strong>and</strong> Planning(<strong>2011</strong>;1–13) <strong>and</strong> entitled “Nutrition agenda setting, policyformulation <strong>and</strong> implementation: lessons from the MainstreamingNutrition Initiative”, the authors highlight the realitythat we face. While undernutrition is the single largest contributorto the global burden of disease <strong>and</strong> can be addressedthrough a number of highly efficacious interventions, ingeneral it has not received commensurate attention in policyagendas at global <strong>and</strong> national levels. Implementing theseefficacious interventions at a national scale has also provendifficult. This is an important fact that has to be considered<strong>and</strong> overcome as SUN rolls out at a country level.setting, policy formulation, capacity building for operations,<strong>and</strong> all other aspects of a long-term nutrition agenda atcountry level.> These conclusions are especially relevant for major globalinitiatives currently under development that seek to addressnutrition through country-led processes <strong>and</strong> convergencebetween multiple organizations.> The extensive investments in documenting the efficacy ofnutrition interventions are unlikely to produce sustainablereductions in undernutrition unless or until these weaknessesin the policy spectrum are better understood <strong>and</strong>addressed.SUN <strong>and</strong> the 1,000 Days movement are the start of alarger movement that hopes to address these real globalnutrition issues by focusing attention, aligning <strong>and</strong> increasingresources, <strong>and</strong> building partnerships. The SUN must shineif nutrition is to take its rightful place <strong>and</strong> deliver to alleviatethe suffering caused by undernutrition among millions ofpeople around the world – especially pregnant women <strong>and</strong>children under two years of age.Key messages include:> Strengthening the full spectrum of policy activitiesis necessary if large-scale <strong>and</strong> sustained reductions inundernutrition are to be achieved.> Within this policy spectrum, high priority should be givento strengthening strategic capacities because these arefundamental to advancing commitment building, agendaComing soon will be a SUN websitewatch for the link from www.sight<strong>and</strong>life.orgnd <strong>Life</strong> <strong>and</strong> Vitamin AngelsImproving Lives in India03er<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> <strong>and</strong> the non-profit organization Vitamin Angels, live in India, making addressing vitamin A deficiency inwhose mission is to mobilize <strong>and</strong> deploy private sector resourcesto advance availability, access <strong>and</strong> use of vitamin A micronutrient deficiencies. While the Government of IndiaIndia a critical component of the global challenge to eliminateby newborns, infants <strong>and</strong> children most in need, have recentlysigned a Memor<strong>and</strong>um of Underst<strong>and</strong>ing. The partnership a large proportion of infants, children <strong>and</strong> lactating womenfully supports initiatives for vitamin A supplementation <strong>and</strong>will work together to build on their individual strengths to receive supplementation, there remains a significant portionfoster local ownership of the problem of vitamin A deficiency of the population that has yet to be reached.in India, <strong>and</strong> catalyze a locally sustainable supply <strong>and</strong> distributionsystem in India.technical expertise <strong>and</strong> Vitamin Angels’ successful implemen-“Through this partnership, <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>’s advocacy <strong>and</strong>Fifty-one percent of the 190 million children under five tation of universal vitamin A supplementation projects aimwho suffer from moderate <strong>and</strong> severe vitamin A deficiency to reach millions of those in India who have to date not
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW83had access to life-saving vitamin A,” says Dr Klaus Kraemer,Director of <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>.In signing this Memor<strong>and</strong>um of Underst<strong>and</strong>ing, both partnershope to engage other international <strong>and</strong> Indian for-profit,not-for-profit <strong>and</strong> government entities. The aim is to mobilizesupport <strong>and</strong> participate in this initiative, in order to harnessinnovative public-private partnerships to sustainably tacklethe vitamin A deficiency epidemic in India <strong>and</strong> improve thelives of millions of infants, children <strong>and</strong> women.For more information on Vitamin Angels go towww.vitaminangels.orgUNICEF Workshop on Scaling Up the Useof Micronutrient Powders to Improve the Quality04lementary Foods for Young Children<strong>and</strong> the Caribbean04AmericaPeruvian children are among those to be impactedby plans to scale up MNPsIn June <strong>2011</strong>, UNICEF <strong>and</strong> the US Centers for Disease Control<strong>and</strong> Prevention (CDC) co-hosted a four-day workshop inMexico to discuss the role of micronutrient powders (MNPs)in improving the quality of complementary feeding in LatinAmerica <strong>and</strong> the Caribbean <strong>and</strong> to support countries in theirplans to introduce <strong>and</strong> scale up MNP programs. Extensiveresearch shows that MNPs are safe, efficacious, acceptable,easy to use <strong>and</strong> do not alter the taste or appearance of food.MNPs are particularly useful to improve the quality of complementaryfoods prepared at home. Based on current evidence,MNPs can easily <strong>and</strong> cost-effectively be administered underprogrammatic conditions <strong>and</strong> implemented at scale. Successfulpublic health scale-up of MNPs does require that they areintegrated within Infant <strong>and</strong> Young Child Nutrition (IYCN)<strong>and</strong> Early Child Development (ECD) programs. Under theseconditions, MNPs have the potential not only to improve themicronutrient content of complementary food <strong>and</strong> decreasethe burden of anemia, but also to improve complementaryfeeding <strong>and</strong> care practices of young children that will, in turn,lead to better growth <strong>and</strong> development outcomes for youngchildren.Many countries in Latin America <strong>and</strong> the Caribbean (LAC)are poised to scale up the use of MNPs as part of integratedIYCN <strong>and</strong> ECD strategies. Furthermore, a unique aspect of theLatin American experience is the use of MNPs as part of an integratedpackage of services included under social protectionschemes such as Conditional Cash Transfer (CCT) programs toreduce social inequities.The comprehensive workshop covered relevant topics,including the current status of MNP interventions in LatinAmerica <strong>and</strong> the Caribbean; the evidence base for MNPs;relevant recommendations regarding MNPs; MNPs in nationalpolicies; MNPs integrated in nutrition strategies; the design ofMNP interventions; MNPs <strong>and</strong> other interventions to improvemicro-nutrient intake; choice of MNP formulation; target⇢
84 WHAT'S NEWgroups; distribution channels; MNPs in acute emergencies;schedules of administration; communication; supply <strong>and</strong>procurement; <strong>and</strong> monitoring <strong>and</strong> evaluation. The workshopconcluded by looking at the challenges <strong>and</strong> areas for followup. Information exchange <strong>and</strong> support mechanisms werediscussed <strong>and</strong> a number of suggestions were made includinginter-country exchange of information through informationcirculars, websites, inter-country exchange visits, tailoredcountry support <strong>and</strong> documentation of best practices <strong>and</strong> lessonslearned through ad hoc consultation.The workshop was attended by participants representing15 countries in LAC, who had the opportunity to engage in <strong>and</strong>discuss the current status of MNP activities in their respectivecountries <strong>and</strong> improve the design of these interventions.Countries exchanged experiences in a way that contributedto strengthening their program design, which in turn had thepotential to substantially contribute to the body of evidenceon the effectiveness of MNPs in programmatic settings.05stDollar05ll Ever SpendIn an excellent on-line article (www.slate.com/id/2281097⁄)originally from Project Syndicate, Copenhagen ConsensusCentre Director Bjørn Lomborg writes: “Micronutrient deficiencyis known as ‘hidden hunger’. This is a fitting description,because it is one of the global challenges that we hearrelatively little about in the developed world. It draws scantmedia attention or celebrity firepower, which are often crucialto attracting charitable donations to a cause. But there is alarger point here: Billions of dollars are given <strong>and</strong> spent onaid <strong>and</strong> development by individuals <strong>and</strong> companies each year.Despite this generosity, we simply do not allocate enough resourcesto solve all of the world’s biggest problems. In a worldfraught with competing claims on human solidarity, we havea moral obligation to direct additional resources to wherethey can achieve the most good. And that is as true of ourown small-scale charitable donations as it is of governments’or philanthropists’ aid budgets. In 2008, the CopenhagenConsensus Center asked a group of the world’s top economiststo identify the ‘investments’ that could best help the planet.The experts – including five Nobel laureates – compared waysto spend US$75 billion on more than 30 interventions aimedat reducing malnutrition, broadening educational opportunity,slowing global warming, cutting air pollution, preventingconflict, fighting disease, improving access to water <strong>and</strong>sanitation, lowering trade <strong>and</strong> immigration barriers, thwartingterrorism, <strong>and</strong> promoting gender equality. Guided by theirconsideration of each option’s costs <strong>and</strong> benefits, <strong>and</strong> settingaside matters such as media attention, the experts identifiedthe best investments: those for which relatively tiny amountsof money could generate significant returns in terms of health,prosperity, <strong>and</strong> community advantages. These included:increased immunization coverage, initiatives to reduce schooldropout rates, community-based nutrition promotion, <strong>and</strong>micronutrient supplementation.”The article goes on to ask: “How could US$ 10 best be spent?Should we, say, buy carbon offsets, or donate to a charityproviding micronutrient supplements? By putting all benefitsto individuals, communities, <strong>and</strong> countries in monetary terms,we can compare the two options. Expert researchers forthe Copenhagen Consensus found that carbon offsets are arelatively ineffective way of reining in global warming <strong>and</strong>reducing its effects – US$ 10 would avoid about US$ 3 ofdamage from climate change. By contrast, US$10 spent onvitamin A supplements would achieve more than US$ 170of benefits in health <strong>and</strong> long-term prosperity. One lesson wecan draw is that while global warming may exacerbateproblems like malnutrition, communities bolstered by adequatenutrition will generally be less vulnerable to climatebasedthreats. Overall, we can typically best help throughdirect interventions, including micronutrient supplements,fortification, biofortification, <strong>and</strong> nutritional promotion.”
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW8527th UNAIDS Programme Coordinating06iscusses Food <strong>and</strong> Nutrition Security in06grammingMichel Sidibé, Executive Director UNAIDS(photo: by courtesy of UNAIDS)“Food <strong>and</strong> nutrition security <strong>and</strong> HIV: how to ensure food <strong>and</strong>nutrition security are integral parts of HIV programming” wasthe theme of the 27th meeting of the UNAIDS Programme CoordinatingBoard meeting held in Geneva in December 2010.The day was organized by representatives of the three UNAIDSconstituencies <strong>and</strong> included a range of expert speakers, aswell as speakers with experience of working in countries <strong>and</strong>programs. It aimed to provide a stimulating opportunity fordialog, exchange, <strong>and</strong> learning, in order to identify pragmaticpolicy <strong>and</strong> programmatic strategies to ensure that food <strong>and</strong>nutrition become integral parts of HIV programming – supportingprevention, treatment care <strong>and</strong> support measures.Experience <strong>and</strong> evidence are mounting that an effective responseto the HIV/AIDS epidemic, including the achievementof universal access to prevention, treatment, care <strong>and</strong> support,requires issues of food <strong>and</strong> nutrition security to be addressed.Adequate nutrition is crucial for good health outcomes ingeneral <strong>and</strong> a strong immune system in particular. For HIV<strong>and</strong> frequent co-infection tuberculosis (TB), as with any otherinfection, good nutrition is critical to keeping the immunesystem strong. Good nutrition can impact the pace of eitherdisease, but will not eliminate the infection. Good nutrition isnot only a critical adjunct of any treatment regimen, butis also important at all stages of the disease.Before the initiation of treatment, good nutrition is critical inorder to maximize the chances of slowing down disease progression.At around the start of antiretroviral therapy (ART),nutritional support is necessary to minimize side effects <strong>and</strong>metabolic challenges, thereby improving adherence. In lowresource settings, HIV <strong>and</strong> frequent co-infection TB oftenstrike where malnutrition is already prevalent <strong>and</strong> compoundit. Additionally, malnutrition is associated with high mortalityin the early months of treatment. The faster the achievementof nutritional recovery through a combination of ART orTB treatment <strong>and</strong> nutritional support, the better the chancesof reducing early mortality.People living with HIV (PLHIV) are at high risk of weightloss <strong>and</strong> wasting, which may compound existing malnutrition.Symptomatic HIV-positive children, for example, have calorieneeds that are 50–100% greater than those of HIV-negativechildren. However, young children often struggle to consumethe amount of calories required, especially when they donot have access to energy dense foods.Although advances in ART have enabled many people tolead relatively normal lives <strong>and</strong> have significantly reducedHIV-related mortality <strong>and</strong> morbidity, fewer than half of thepeople living with HIV had access to treatment in 2010. Whilesupply-side issues are part of the reason for this, many failto seek treatment or show poor adherence. The reasonsbehind the lack of uptake <strong>and</strong> adherence are not always wellunderstood, but evidence suggests that food insecurity <strong>and</strong>the cost of transport may be partially responsible. For thosewho have access to treatment, weight loss or malnutritionmay affect the efficacy of ART.⇢
86 WHAT'S NEWFood <strong>and</strong> nutrition security is also an essential element of effectivecare <strong>and</strong> support in HIV-affected households <strong>and</strong> communities.In low-income countries, HIV contributes to foodinsecurity <strong>and</strong> malnutrition <strong>and</strong> has consequences for entirecommunities <strong>and</strong> societies, with the potential to significantlyslow down economic development. Livelihoods are disruptedas PLHIV lose the ability to work, which exacerbates food insecurity,<strong>and</strong> they <strong>and</strong> their families are often excluded frominformal safety nets because of the stigma associated withthe disease.Food insecurity frequently places people, especially women<strong>and</strong> girls, in situations that make them more vulnerableto transmission. It can lead to behaviors that have negativeconsequences, such as selling assets, removing children fromschool, migrating <strong>and</strong> engaging in transactional sex. Thesebehaviors exact a substantial price in the long term, includingincreased exposure to HIV. Mitigating food insecurity can,therefore, contribute to a reduction in the risk of transmission.All these elements highlight the importance of appropriatepolicy <strong>and</strong> programs to ensure the integration of food <strong>and</strong>nutrition in HIV <strong>and</strong> co-infection program design <strong>and</strong> implementation,with reference to the related reality that effectivefood <strong>and</strong> nutrition security programming must also beHIV-sensitive.All aspects of UNAIDS work are directed bythe following guiding principles:> aligned to national stakeholders’ priorities;> based on the meaningful <strong>and</strong> measurable involvement ofcivil society, especially people living with HIV <strong>and</strong>populations most at risk of HIV infection;> based on human rights <strong>and</strong> gender equality;> based on the best available scientific evidence <strong>and</strong>technical knowledge;> promoting comprehensive responses to AIDS that integrateprevention, treatment, care <strong>and</strong> support; <strong>and</strong>> based on the principle of non-discrimination.To access the UNAIDS Strategy <strong>2011</strong>-2015, go towww.unaids.org/en/strategygoalsby2015/International Food Policy Research Institute– Making the Link between Agriculture07tritionEconomic growth, which many assume has a natural positiveimpact on nutritional status through increased incomes <strong>and</strong>food expenditures, has not translated into improved nutritionin a number of developing countries. Considering this disconnect,IFPRI has released an important paper entitled “Thenexus between agriculture <strong>and</strong> nutrition – Do growth patterns<strong>and</strong> conditional factors matter?” This seeks to provide anoverview of the complex <strong>and</strong> dynamic relationship betweennutrition <strong>and</strong> growth, examine how different growthpatterns lead to different nutritional outcomes, <strong>and</strong> identifythe factors that influence the magnitude of this relationship.It aims to offer researchers insights on areas for future research<strong>and</strong> analysis <strong>and</strong> to provide policymakers withknowledge regarding potential development strategies <strong>and</strong>investment policies that will increase the likelihood ofpositive nutritional outcomes.As globally we try to break down the individual silos thatnutrition <strong>and</strong> agriculture have built <strong>and</strong> functioned within,<strong>and</strong> in light of the growth of the Scaling Up Nutrition (SUN)movement, this paper is important. It will hopefully lead tomany meaningful discussions <strong>and</strong>, more importantly, agriculturalgrowth that leads not only to increased production <strong>and</strong>reduced poverty, but also to improved nutrition.The paper can be accessed at www.ifpri.org/publication/nexus-between-agriculture-<strong>and</strong>-nutrition-0
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW87ure of Food <strong>and</strong> Farming: Challengesfor Global Sustainability08icesThe report is comprehensive <strong>and</strong> coversfive specific challenges:1. Balancing future dem<strong>and</strong> <strong>and</strong> supply sustainably, <strong>and</strong>ensuring that food is affordable;2. Ensuring adequate stability in food supplies, <strong>and</strong> protectingthe most vulnerable from any volatility that does occur;3. Achieving global access to food, <strong>and</strong> an end to hunger;4. Managing the contribution of the food system to themitigation of climate change; <strong>and</strong>5. Maintaining biodiversity <strong>and</strong> ecosystem services whilefeeding the world. The report emphasizes the need to buildin greater resilience to future food price shocks, highlightsthe vulnerability of the global food system <strong>and</strong> is a mustreadfor anyone interested in the food system.The UK Government Office for Science recently publishedthe Foresight Project Global Food <strong>and</strong> Farming Futures report,which provides an overview of the evidence <strong>and</strong> discussesthe challenges <strong>and</strong> choices for policy makers pertaining to allaspects of the global food system. The impetus for the developmentof the document was the question of how to balancethe competing pressures <strong>and</strong> dem<strong>and</strong>s on the global foodsystem. The project brought together evidence <strong>and</strong> expertisefrom a wide range of disciplines across the natural <strong>and</strong> socialsciences to assess what might enable or inhibit future change.The full report <strong>and</strong> executive summary can be found atwww.bis.gov.uk/foresight/our-work/projects/current-projects/global-food-<strong>and</strong>-farming-futures/reports-<strong>and</strong>-publications
88 WHAT'S NEWricesYet Again …09RiseGlobal food prices rose to a fresh high in February <strong>2011</strong> –the eighth consecutive month of rising prices. Averaging236 points, prices were up 2.2% from January <strong>and</strong> were thehighest since January 1990, the inception date of the index.With the exception of sugar, the prices of all othercommodity groups monitored registered gains in February,with dairy products <strong>and</strong> cereals climbing the most. TheFood <strong>and</strong> Agriculture Organization of the United Nations(FAO) index measures monthly price changes for a food basketcomposed of dairy, meat <strong>and</strong> sugar, cereals <strong>and</strong> oilseeds.With the current global unrest <strong>and</strong> recent naturaldisasters, it is unclear where prices will go in <strong>2011</strong>. This iscause for real concern, especially given that the last crisispushed 100 million additional people into hunger <strong>and</strong>, in addition,that rising food prices have the greatest impact on poorcountries, where food <strong>and</strong> energy are people’s majorspending focus.To monitor the index, visitwww.fao.org/worldfoodsituation/wfs-home/foodpricesindex/en/The Hungrier the Louder250200KazakhstanTunisiaThe government announced a rise of6 % of the food prices in 2010, which bearslittle relation to the reality experienced bythe populationRates of cereal self-sufficiency (in %)150100500RussiaUkraineBelarusAlbaniaSouth Africa TurkeyEgyptMoroccoGeorgiaArmeniaIsrael TunisiaAlgeriaJordan10 20 30 40 50 60Weighting of food in calculation of inflation (in %)MoroccoThe country lays out an agriculturalsystem which makes it a little less fragilethan its neighbors’EgyptFood price rises make up 55% ofoverall increases - a burden for familieson modest incomesAlgeriaNational production covers only14% of annual cereal requirementsSource: Challenges, March 3,<strong>2011</strong>
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW89Launches Valuable Resources:10n Update 2010With the exception of reported data on Guatemala (whichcomes from the 2008-09 Encuesta Nacional de Salud MaternoInfantil (ENSMI), a Regional Health Survey), the studysummarizes data from the results of Demographic <strong>and</strong> HealthSurveys (DHS) providing population level estimates of keynutrition indicators <strong>and</strong> carried out between 2003 <strong>and</strong> 2009in 35 countries in Sub-Saharan Africa, South/Southeast Asia,Latin America, <strong>and</strong> the Caribbean. The majority of thesecountries are among those identified in the 2008 LancetSeries on Maternal <strong>and</strong> Child Nutrition as having the greatestburden of undernutrition. All the data presented in this documentwere re-run for comparative purposes <strong>and</strong> thus somenumbers in the report might not be an exact match with theDHS final country reports.With nutrition gaining more visibility at all levels internationally,regionally <strong>and</strong> nationally, the USAID NutritionUpdate 2010 is an important resource. The 36-page documentprovides information on nutritional status, anemia status,breastfeeding, the introduction of solid, semi-solid or softfoods, minimum dietary diversity, minimum meal frequency,minimum acceptable diet, women’s dietary diversity, <strong>and</strong>micronutrient supplementation among pregnant <strong>and</strong> postpartumwomen <strong>and</strong> infant <strong>and</strong> young children (less thanfive years).The English document is available atwww.measuredhs.com/pubs/pdf/NUT4/NUT4.pdf
90 WHAT'S NEWA2Z: The USAID Micronutrient <strong>and</strong> ChildBlindness Project Releases Five New Publicationsed to Support Food Fortification EffortsBank11WestA2Z: The USAID Micronutrient <strong>and</strong> Child BlindnessProject consolidates, builds, <strong>and</strong> exp<strong>and</strong>s on USAID’s longterminvestment in micronutrients, child survival, <strong>and</strong> nutrition.Food fortification is viewed by A2Z as an important strategyin achieving its goal <strong>and</strong> focus countries have includedBangladesh, Cambodia, the ECSA region, India, Nepal,Philippines, Tanzania, Ug<strong>and</strong>a <strong>and</strong> the West Bank. A2Z haveprovided technical assistance to the Palestinian Authority inorder to increase the provision of essential micronutrientsin the Palestinian diet, thereby reducing the risk of micronutrientdeficiencies in the West Bank.> Manual of Methods for Determining Micronutrientsin Fortified Foods> Inspection Manual for Monitoring Salt <strong>and</strong>Flour Fortification> Analysis of Inspection Results from Salt <strong>and</strong>Wheat Flour SamplesAll five publications are available athttp://a2zproject.org/node/89In line with this, it recently released five publicationsfocused on the West Bank:> Determining the Dietary Patterns <strong>and</strong> BiochemicalMarkers among Women <strong>and</strong> Children in Hebron<strong>and</strong> Gaza City> The Dem<strong>and</strong> for Locally ManufacturedComplementary Food Products among PalestinianCaregiversWHO Launch a Set of Recommendations onrketing of Food <strong>and</strong> Non-Alcoholic Beverages12drenAccording to the WHO, non-communicable diseases(NCDs) represent a leading threat to human health <strong>and</strong> socioeconomicdevelopment. Eighty percent of NCD deaths occurin low- <strong>and</strong> middle income countries. And, while deathsfrom NCDs primarily occur in adulthood, the risks associatedwith an unhealthy diet begin in childhood <strong>and</strong> build upthroughout life.“The already heavy burden caused by NCDs, along with thefact that the majority of these deaths are premature <strong>and</strong>could be averted, provide a strong public health <strong>and</strong> policyimperative to act,” states Dr Ala Alwan, the Assistant Director-General Non-communicable Diseases <strong>and</strong> Mental Health ofthe WHO, in the foreword to a new WHO publication entitled“Set of recommendations on the marketing of food <strong>and</strong> nonalcoholicbeverages to children.”
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW91Considering that it is estimated that in 2010 more than42 million children under the age of five years were overweightor obese, of whom nearly 35 million were livingin developing countries, these recommendations are timely.Their purpose is to guide efforts by UN Member States indesigning new <strong>and</strong>/or strengthening existing policies onfood marketing communications to children.The recommendations can be accessed in a number oflanguages from www.who.int/dietphysicalactivity/publications/recsmarketing/en/A Cochrane Review of Vitamin ASupplementation for Preventing Morbidity <strong>and</strong>y in Children from Six Months13YearsThis review by Aamer Imdat <strong>and</strong> coworkers includes 43r<strong>and</strong>omized trials representing 215,633 children <strong>and</strong> showsthat giving vitamin A capsules to children aged six monthsto five years can reduce death <strong>and</strong> some diseases. The resultsof 17 of the studies have been summarized <strong>and</strong> indicate thatvitamin A reduces the overall risk of death by 24%. Death dueto measles, respiratory infections or meningitis was not specificallyreduced, but vitamin A could reduce new occurrencesof diarrhea <strong>and</strong> measles. When people took very large dosesof vitamin A, they were more likely to vomit within two days.In the author’s opinion, given the evidence that vitaminA supplementation (VAS) causes a considerable reductionin child mortality, further placebo-controlled trials of VASin children between six months <strong>and</strong> five years of age are notrequired. There is, however, a need for further studies thatcompare different doses <strong>and</strong> delivery mechanisms (for example,fortification). In addition, as the effects of VAS on relevantpathogens <strong>and</strong> disease pathways are not well understood,these could be further researched, together with the elucidationof the relationship (if any) between vitamin A <strong>and</strong> growth.The reviewers also give implications for practice, giventhat national <strong>and</strong> regional programs of VAS are in placein over 70 countries worldwide <strong>and</strong> may be among the mostcost-effective public health interventions. As more than190 million children are vitamin A deficient around theglobe, a reduction in their risk of mortality by 24% could savealmost 1 million lives a year. These interventions respondto an immediate need for adequate nutrition; however, theyare not ideal long-term solutions to the underlying problem.Fortification, food distribution programs <strong>and</strong> horticulturaldevelopments may provide more permanent relief.Furthermore, if vitamin A reduces mortality by preventingmeasles, widespread vaccination will reduce the relativecontribution of vitamin A supplementation. Until such longtermsolutions are in place, supplementation should continue.The researchers also recommend that, as access to vitamin Aincreases, it will be important to continue to identify at-riskgroups <strong>and</strong> deliver supplements to them. They strongly recommendvitamin A supplementation to children under five inareas at risk of VAD. The exact nature of how these programsshould be structured <strong>and</strong> administered – the dose, frequency,<strong>and</strong> duration of intervention – is less certain. The researchersalso suggest that VAS for pregnant <strong>and</strong> lactating mothers <strong>and</strong>other efforts to promote the delivery of vitamin A (such asincreased rates <strong>and</strong> duration of breastfeeding) may requirefurther attention.Finally, it is worth noting that two additional Cochranereviews recently investigated the effects of vitamin A duringthe neonatal period (infants aged one to six months) <strong>and</strong> willbe available shortly.For the full review, go tohttp://onlinelibrary.wiley.com/o/cochrane/clsysrev/articlesCD008524/frame.html
92 WHAT'S NEW4ne Collaboration JoinsHealth Assembly14ldThe Cochrane Collaboration was recently accepted as aNon-Governmental Organization in Official Relations with theWorld Health Organization (WHO). In formalizing the relationshipwith the WHO, the Collaboration has been awarded aseat as an observer at the World Health Assembly, allowingthe Cochrane Collaboration to provide input on WHO healthresolutions <strong>and</strong> formalizing the communications betweenthe two bodies.The partnership will allow the Cochrane Collaboration tosignificantly influence the way research evidence is created<strong>and</strong> used by the WHO, by improving the collection of reliablehealth information <strong>and</strong> promoting intersectoral collaboration<strong>and</strong> high-quality research to produce the necessary evidenceto ensure policies in all sectors contribute to improvinghealth <strong>and</strong> health equity.Current plans for continued partnership between theCochrane Collaboration <strong>and</strong> the World Health Organizationinclude the development of the WHO e-Library of Evidencefor Nutrition Actions (eLENA). Cochrane contributors haveidentified relevant Cochrane Reviews <strong>and</strong> are updating orconducting new Cochrane Reviews in response to the WHO’spriorities. This process will facilitate the development ofsound, evidence-informed guidelines on nutrition issuesrelevant to WHO Member States <strong>and</strong> other partners.For more information on the Cochrane Collaboration, visitwww.cochrane.orgns New York AcademyNutrition Council15nces’From left to right: Manfred Eggersdorfer, Michael Burney,Jim Hamilton, Bruce Cogill, Grace Xu, Hugh Welsh, Jim Elliott<strong>and</strong> Jon PetersDSM, of which <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> is the humanitarian initiative,officially joined the Leadership Council of the New York Academyof Sciences’ Global Nutrition Science Research Initiativeduring the Academy’s gala dinner. DSM is the only food ingredientcompany to be among the more than 20 organizationscoming from government, academia <strong>and</strong> the non-profit <strong>and</strong>private sectors that comprise the Council.This l<strong>and</strong>mark move will bring together the best scientificresearch <strong>and</strong> development competences available on nutritionto address global hidden hunger in rich <strong>and</strong> poor countriesalike. In collaboration with the World Health Organization,this initiative will shape the global nutrition scienceresearch agenda <strong>and</strong> facilitate a multi-sector action plan. Theobjective is for this body of research to be used to help donorcountries, development organizations, <strong>and</strong> governmentsto design <strong>and</strong> implement more effective nutrition programs.“I am excited <strong>and</strong> honored to be part of such an ambitious <strong>and</strong>one-of-a-kind initiative <strong>and</strong> [to have] the opportunity to workwith such a prestigious group of experts,” commented
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>WHAT'S NEW93Manfred Eggersdorfer, Senior Vice President NutritionScience & Advocacy, DSM Nutritional Products. “The design<strong>and</strong> implementation of successful nutrition programs requiresserious research <strong>and</strong> I hope that our work can help scientists,governments <strong>and</strong> organizations around the world tackle oneof the most serious global health problems which, until recently,has been underappreciated <strong>and</strong> often misunderstood.”CeSSIAM – Center for Studies ofy Impairment, Aging <strong>and</strong> Metabolism25 Years16tesCeSSIAM began in Guatemala as a non-profit organizationdedicated to nutrition research <strong>and</strong> education <strong>and</strong> has as itsmission the improvement of human health <strong>and</strong> well-being inunderprivileged societies through better nutrition. It worksin partnership with the Hildegard-Grunow-Foundation forNutrition Research (HGF) <strong>and</strong> the Nevin Scrimshaw InternationalNutrition Foundation (INF). The current Executive <strong>and</strong>Scientific Director is Dr Noel Solomons, who was awarded theNational Science <strong>and</strong> Technology Medal for 2010 in recognitionof his scientific research in the area of nutrition, <strong>and</strong> itssignificant contribution to health in Guatemala. His researchhas also had a significant impact on child nutrition policies atboth national <strong>and</strong> international levels. <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> has hada long relationship with CeSSIAM <strong>and</strong> presented Dr Solomonswith a certificate to mark its 25th Anniversary at a celebrationat the World Public Health Nutrition Congress in Porto inOctober 2010.To find out more about CeSSIAM, visitwww.hgrunowfoundation.org/cessiamKlaus Kraemer presents Noel Solomons with a certificatethat commemorates his long-st<strong>and</strong>ing commitment to fightingmicronutrient deficiencies
94WHAT'S NEW17Atmala’s Medal of Science <strong>and</strong> Technology17ded to CeSSIAM’s Dr Noel SolomonsNoel Solomons is awarded the Medal of Science<strong>and</strong> Technology by the National Council of Science <strong>and</strong>Technology of Guatemalatheir fourth regular meeting in 2010, the National Councilof Science <strong>and</strong> Technology of Guatemala (CONCYT) reviewedthe proposals for the 2010 competition for the award of theMedal of Science <strong>and</strong> Technology, or “Medalla de la Cienciay Tecnología.” The medal is the highest annual recognition ata national level for a scientist who has made a transcendingsocial impact.The Guatemalan Academy of Medical, Physical <strong>and</strong> NaturalSciences submitted a proposal for the award to go to Dr NoelW Solomons of the Center for Studies of Sensory Impairment,Aging <strong>and</strong> Metabolism (CeSSIAM). As a result, CONCYT decidedto name Dr Solomons as the winner of this award, on thebasis of his contribution to nutrition research in Guatemala.The medal was presented at a ceremony held in conjunctionwith the Congress by Dr Rafael Espada, Vice President ofthe Republic of Guatemala.tional Year of Chemistry:18C Molecule on Swiss Stamp<strong>2011</strong> having been declared by the United Nations to be“International Year of Chemistry”, the Swiss Post has releaseda special issue stamp that features a vitamin C molecule.Synthetic vitamin C was first developed by Tadeus Reichsteinin 1933 at the Swiss Federal Institute of Technology (ETH)Zurich.Swiss Post is commemorating the International Yearof Chemistry with a special issue stamp showing a vitamin Cmolecule
Advocatingbetter nutritionfor brighterfutures.
96Comments on the Comparison of the Effectsof Organic <strong>and</strong> Conventional Food on Health in<strong>Sight</strong> And <strong>Life</strong> 2/2010Tsige-Yohannes Habte, Michael KrawinkelUniversity of Giessen, GermanyWe read the article on Organic vs Conventional Food 1 in <strong>Sight</strong>And <strong>Life</strong> <strong>Magazine</strong> 2/2010 with interest. It states that the nutritionalquality of organic food is not different from conventionalfood, <strong>and</strong> that there is no evidence of any difference that mighthave an impact on health. At a certain point, the argument veersto the subject of epidemiological studies that show that a diethigh in fruit <strong>and</strong> vegetables reduces mortality from cardiovasculardiseases, but there is scant evidence on the effects of cancer.We have no reservations about the health advantages of recommendedlevels of fruits <strong>and</strong> vegetables. However, the comparisonof conventional <strong>and</strong> organic food impact on health appearsto require further revision.What is conventional food?We underst<strong>and</strong> the term “conventional food” to mean the foodstuffsthat are produced by intensive agricultural systems whereconsiderably improved technology, particularly in the form ofagrochemicals, is applied to enhance productivity. However, amarked level of uncertainty about health risk still attaches tothis sort of conventional food.When conventional food is compared with organic food, nutrientcomposition is not a major concern with regard to healthrisks. Indeed, varying foodstuffs are different in terms of theircomposition, which is why diverse sources of nutrients are used“The major health concern aboutconventional food is its contaminationwith agrochemicals”to balance a healthy diet. No foodstuff is complete on its own,<strong>and</strong> diversity <strong>and</strong> complementarities are the order of nutrition.The major health concern about conventional food is itscontamination with agrochemicals, particularly those related topesticides, hormones <strong>and</strong> antibiotics. A large number of studiesreveal that people consuming a conventional diet are more exposedto pesticide residues than those who consume an organicdiet; some examples are cited below.Recent studies in the US show that children fed organic dietshad significantly lower exposure to organophosphorus pesticidethan children with primarily conventional diets. The mediantotal methyl metabolite concentration in their urine was aboutsix times higher for those children on a conventional diet than itwas for children on organic diets (0.7 vs 0.03 μmol/L; P=0003),<strong>and</strong> mean concentration differed by a factor of nine (0.34 vs0.04 μmol/L). 2 At present, the pesticides that are most commonly<strong>and</strong> widely used are organophosphate pesticides. They are normallyeliminated from the body after three to six days, <strong>and</strong> thedetection of this compound indicates continuing exposure.Assessments conducted on more than 90,000 samples of20 major crops, grown organically or conventionally, indicatedthat the frequencies of residue detection <strong>and</strong> residue levels wereconsiderably higher in conventional than in organic foods. Conventionalfood contained pesticide residues in more than 75%of the cases. 3 Not all of the organic foods were, however, totallyfree from pesticide residue. They were also adulterated, but toa markedly lesser extent <strong>and</strong> frequency than conventional food.Most of the residues in organic foods are explained as the unavoidableresults of environmental contamination by post-pesticideuse, or drift (sprays blown in from adjacent, non-organicfarms).
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>LETTERS TO THE EDITOR97Pesticide exposure around the worldHuman beings can be exposed to pesticides in a variety of ways,at different dose levels, <strong>and</strong> for varying periods of time. In thedeveloped world, the problem of acute pesticide poisoning haslargely been controlled; major health problems arise from exposureto low levels of pesticide residues in food over a long periodof time. In developing countries, however, the main healthproblem arising from pesticides is that due to acute poisoning.A minimum of 25 million agricultural workers in developingcountries suffer an episode of pesticide poisoning each year. 4It has become evident in the last few years that acute pesticidepoisoning is mainly the concern of the developing world, whichlacks appropriate protection <strong>and</strong> management mechanisms dueto low levels of awareness <strong>and</strong> inadequate infrastructures.Exposure to pesticides can potentially affect human health.Controlled studies on animals indicate substantial toxicologicalevidence showing that repeated low-level exposure to organophosphatepesticides affects neural development <strong>and</strong> growthin developing animals. Some of these studies indicate the impairmentof maze performance, locomotion <strong>and</strong> balance in neonatesexposed in the uterus <strong>and</strong> early in postnatal life. Possiblemechanisms leading to these effects include inhibition of brainacetylcholinesterase, down-regulation of muscarinic receptors,decreased brain DNA synthesis, <strong>and</strong> reduced brain weight. It isalso possible that exposure to organophosphate pesticides relatesto respiratory diseases in children through improper regulationof the autonomic nervous system. 5Studies of the effects of pesticide exposure on children’shealth have been limited to birth defects. Several case-controlstudies have associated parental exposure to pesticides or pesticideuse in the home with childhood brain tumors, leukemia,lymphomas, <strong>and</strong> testicular cancer. 6,7A small number of ecological studies have examined whetherthe low-level chronic exposure of children to pesticides can leadto adverse health consequences. A study in Mexico found thatchildren of four to five years of age living in an agricultural valleywith presumably higher pesticide exposure had deficits whentested for stamina, coordination, <strong>and</strong> recall, as compared to childrenliving in the foothills where there was mainly ranching. 8“Chronic, low-level exposureto pesticides may affect neurologicalfunctions, neurodevelopment,<strong>and</strong> growth”Advantages of organic food over conventional foodIn general it can be said that, despite the paucity of informationconcerning the potential health effects in children of chronic, lowlevelexposure to pesticides, substantial evidence from rodents<strong>and</strong> limited information from adult humans shows that chronic,low-level exposure to pesticides may affect neurological functions,neurodevelopment, <strong>and</strong> growth. The preference for organic foodover conventional food appears advantageous in view of the lowerexposure to insecticide residues <strong>and</strong> minimizing health risks.Correspondence: Michael Krawinkel,Institute of Human Nutrition, University of Giessen,Wilhelmstrasse 20, 35392 Giessen, GermanyE-mail: michael.krawinkel@ernaehrung.uni-giessen.deReferences01. Thurnham DI. Should Organically Produced Foods be Healthierthan Conventionally Grown Foods? <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> <strong>Magazine</strong>2010;2:30–38.02. Curl CL, Fenske RA, Elgethun K. Organophosphorus PesticideExposure of Urban <strong>and</strong> Suburban Preschool Children with Organic<strong>and</strong> Conventional Diets. Environmental Health Perspectives2003;111:377–382.03. Baker BP, Benbrook CM, Groth E et al. Pesticide residues in conventional,IPM-grown <strong>and</strong> organic foods: Insights from three US datasets. Food Additives <strong>and</strong> Contaminants 2002; 19:427–446.04. Jeyaratnam J. Acute Pesticide Poisoning: A Major Global HealthProblem. World Health Statistics Quarterly 1990:43:139–144.05. Eskenazi B, Bradman A, Castorina R. Exposure of Children toOrganophosphate Pesticides <strong>and</strong> Their Potential Adverse Effects.Environmental Health Perspectives 1999;107:409–419.06. Blair A, Zahm SH, Pearce NE et al. Clues to cancer etiology fromstudies of farmers. Sc<strong>and</strong> J Work Environ Health 1990;18:209–215.07. Buckley JD, Robison LL, Swotinsky R et al. Occupational exposureof parents of children with acute nonlymphocytic leukaemia: areport from the Children’s Cancer Study Group. Cancer Research1989;49:4030–4037.08. Guillette EA, Meza MM, Aquilar MG et al. An anthropologicalapproach to the evaluation of preschool children exposed to pesticidesin Mexico. Environ Health Perspect 1998;106:347–353.
98Editor’s note: <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> reviews recent publications whichmay be of particular interest to our readers. However, no publicationsother than <strong>Sight</strong> <strong>and</strong> <strong>Life</strong> publications are available fromus, nor do we have any privileged access to them.Folate inHealth <strong>and</strong> Disease2nd EditionMore than a decade has passed since the first edition ofFolate in Health <strong>and</strong> Disease was published. During this time,there have been thous<strong>and</strong>s of new research studies related tofolate <strong>and</strong> its link to disease <strong>and</strong> birth defect risk, thus providingthe impetus for an updated interpretation of this largebody of scientific evidence. The public health implicationsof these new findings are enormous; therefore, the secondedition bridges basic science with clinical medicine <strong>and</strong>public health.The first chapters provide background knowledge relatedto folate chemistry, metabolism, bioavailability, <strong>and</strong> the influenceof genetic polymorphisms. Folate’s role in reproduction<strong>and</strong> birth defect prevention is then reviewed, followed by aseparate chapter in which epidemiological evidence linkingspecific birth defects <strong>and</strong> folate status is evaluated. Chronicdisease is covered in a similar manner to that of birth defects.The interrelationships between folate <strong>and</strong> other nutrientsrequired for normal one-carbon metabolism are then coveredin several chapters, <strong>and</strong> the biochemical <strong>and</strong> clinical ramificationsof alterations in status are highlighted. The interactionbetween folate <strong>and</strong> vitamin B₁₂ is addressed from abiochemical <strong>and</strong> public health perspective. The complexitiesof diagnosis <strong>and</strong> treatment of a clinical folate deficiency arediscussed, followed by a related chapter on the effect ofalcohol on folate <strong>and</strong> methionine metabolism. Choline iscovered in a separate chapter.Dietary intake recommendations for select countries worldwideare compared with an overview of the approaches usedby the Institute of Medicine’s committee to estimate theDietary Reference Intakes. Changes in folate status over timewithin the US population are a focus of this chapter, withattention given to the influence of folic acid fortification <strong>and</strong>supplement use on folate status. Estimated dietary folate intakesfor the US population <strong>and</strong> specific population subgroupsare presented.For more information, please visithttp://www.routledge.com/books/details/9781420071245/
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>PUBLICATIONS99CarotenoidsA Colorful <strong>and</strong>TimelyResearch FieldBecause carotenoids are widely consumed <strong>and</strong> their consumptionis a modifiable health behavior (via diets or supplements),health benefits for chronic disease prevention, if real,could be very significant for public health.This book spans the breadth of ongoing work by researchersaround the world, ranging from basic studies to advancedapplied biomedical research. As in many fields of research,new tools <strong>and</strong> techniques for measuring carotenoids in varioussystems are critical to support research progress. Severalchapters discuss new methodologies to measure carotenoids,carotenoid metabolites/radicals, or carotenoids in vivo incomplex biological systems, especially in the human eye. Otherchapters describe the oxygenase enzymes that are essentialcomponents of carotenoid metabolism to active metabolites.How carotenoids behaveCarotenoids are highly lipophilic: an active area of researchconcerns how carotenoids interact with <strong>and</strong> affect membranesystems. Also, the lipid solubility of these compounds hasimportant implications for carotenoid intestinal absorption:models such as the Caco-2 cell model are being used to conductdetailed studies of carotenoid absorption / competitionfor absorption. The lipid solubility of these carotenoids alsoleads to the aggregation of carotenoids. Carotenoids aggregateboth in natural <strong>and</strong> artificial systems, with implications forcarotenoid excited states. This in turn has implications for anew indication for carotenoids, namely, serving as potentialmaterials for harnessing solar energy.In summary, the amazing breadth <strong>and</strong> depth of researchin carotenoids are reasons why it draws investigators to thisfascinating field of research. The research spans the continuumfrom detailed studies of the roles of photoprotectivecarotenoids in plants to the potential application in the preventionof disease in humans. This is translational researchat its best <strong>and</strong> I commend the editor, Dr John L<strong>and</strong>rum, forassembling such an interesting <strong>and</strong> informative collection ofcurrent research.Reviewed bySusan T Mayne Yale University School of MedicineFor more information, please visithttp://www.routledge.com/books/details/9781420052305/
100 PUBLICATIONSOmega-3Fatty Acids <strong>and</strong>the DHA PrincipleThe physical <strong>and</strong> chemical properties of the omega-3fatty acid DHA (docosahexaenoic acid) enable it to facilitatebiochemical processes in the membrane. This effect hasnumerous benefits, including those involved in the growthof bacteria, rapid energy generation, human vision, brain impulse,<strong>and</strong> photosynthesis, to name but a few. However DHAalso carries risks that can lead to cellular death <strong>and</strong> disease.Omega-3 Fatty Acids <strong>and</strong> the DHA Principle explores theroles of omega-3 fatty acids in cellular membranes, rangingfrom human neurons <strong>and</strong> swimming sperm to deep seabacteria, <strong>and</strong> develops a principle by which to assess theirbenefits <strong>and</strong> risks.The DHA Principle states that the blending of lipids toform cellular membranes is evolutionarily honed to maximizebenefit while minimizing risk, <strong>and</strong> that a complex blendingcode involving conformational dynamics, energy stress,energy yield, <strong>and</strong> chemical stability underlies all cellularmembranes.shifting to a practical discussion on applications. Theauthors discuss the DHA Principle as applied to petroleumdegradation, winemaking, global warming, molecular farming,aging, neuro-degenerative diseases, <strong>and</strong> the prevention ofcolon cancer.A reflection on the increased public interest to haveemerged over the years, this volume uses an integrativeapproach to explain the complex roles of omega-3s inthe membrane. Incorporating principles from chemistry,cellular biology, evolution, <strong>and</strong> ecology, this work givesresearchers in a variety of fields the building blocks tostimulate further study.For more information, please visithttp://www.routledge.com/books/details/9781439812990/Underst<strong>and</strong>ing the codeThis book lays the groundwork to underst<strong>and</strong>ing this code.It examines the evolution of DHA <strong>and</strong> the membrane, <strong>and</strong>explores the general properties of omega-3s <strong>and</strong> othermembrane lipids. It then focuses on cellular biology before
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong>PUBLICATIONS101NutritionBooks Availablefrom TALC Valuablefor NutritionPractitioners <strong>and</strong>TrainersTALC (Teaching Aids at Low Cost) is a unique charity providing<strong>and</strong> developing educational material which promotesthe health of children <strong>and</strong> advanced medical knowledge <strong>and</strong>teaching in the UK <strong>and</strong> throughout the world.The organization was founded in 1965 by David Morleywhen he was lecturer at the Institute of Child Health, in responseto many requests from overseas students for teachingequipment to use in their own countries.TALC believes good health provision should be availableto all – especially those in the poorest communities in Africa,Asia, <strong>and</strong> Latin America – <strong>and</strong> has been working for over40 years to achieve this. They currently supply over 10,000health workers with health materials, ranging from text books<strong>and</strong> videos to CDs <strong>and</strong> weight charts.Below is a list of nutrition books, CD-ROMs <strong>and</strong> accessoriesavailable from TALC, as recommended by Ann Burgess<strong>and</strong> Marko Kerac (* indicates the book is available in otherlanguages besides English).> Community Nutrition: a h<strong>and</strong>book for health <strong>and</strong> developmentworkers; 2009 Burgess, Bijlsma & Ismael; £5.50.> Infant <strong>and</strong> Young Child Feeding – model chapter fortextbooks for medical students <strong>and</strong> allied healthprofessionals; 2009 WHO; £1.30.> Caring for Severely Malnourished Children; 2003Ashworth & Burgess; £4.10 (also available at the same priceas a PDF download).> <strong>Sight</strong> And <strong>Life</strong> Manual on Vitamin A Deficiency Disorders(VADD); (2nd ed 2001) <strong>Sight</strong> And <strong>Life</strong>; £1 (*French, Spanish).> The Politics of Breastfeeding (3rd edition);2009 Palmer; £7.70.> Protein-Energy Malnutrition; 2006 Waterlow; £7.50.> Hospital Care for Children – Guidelines for theManagement of Common Illnesses with LimitedResources; 2005 WHO; £4.50 (*French, Russian).> ABC of Nutrition (4th edition); 2003 BookPower; £6.00.> Nutrition for Developing Countries (2nd edition);1993 Savage King & Burgess; £12.00.> Community Nutrition CD-ROM; TALC 2006. Free to healthprofessionals who have limited access to the internet,Community Nutrition is a new CD-ROMcontaining hundreds of nutrition resources includingmanuals, training courses, academic papers, briefs,practical guidelines, pictures, presentations, <strong>and</strong> a video.> Topics in International Health – Nutrition CD-ROM;2000 Wellcome Trust; £5.00. Twelve interactive tutorialsthat provide an illustrated introduction to the causes,epidemiology, treatment, <strong>and</strong> prevention of malnutritionin developing countries.> e-TALC Health Development CD-ROMs. The e-TALC projectprovides a reliable <strong>and</strong> regular source of free healthinformation, aimed at healthcare workers in developingcountries who have no or limited access to the internet.Small colored insertion tape (MUAC); 115mm; £0.25.> Hemoglobin color scale; £24.00. A simple devicefor estimating hemoglobin, for use when laboratoryhemoglobinometry is not available.TALC is based in the UK. To order any of these items, visithttp://www.talcuk.org/index.htm or e-mail info@talcuk.org or call+44 (0)1727 853869. Prices do not include postageIf you know of any other recent, good value nutritionrelatedbooks that TALC might add to its catalogue, pleaselet them know.
Sharingknowledgefor improvednutrition.
SIGHTANDLIFE|VOL.25(1)|<strong>2011</strong>IMPRINT 103Imprint<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> <strong>Magazine</strong>Layout <strong>and</strong> graphics:<strong>Sight</strong> <strong>and</strong> <strong>Life</strong>Incorporating theS1 Studio for Graphic Design,Dr Klaus KraemerXerophthalmia Club BulletinAugsburgDirectorPO Box 2116Publisher: <strong>Sight</strong> <strong>and</strong> <strong>Life</strong>Printer: Burger Druck,4002 Basel, Switzerl<strong>and</strong>Editor: Klaus KraemerWaldkirchPhone: +41 (0) 61 815 8756Carbon-neutral productionEditorial team:Fax: +41 (0) 61 815 8190Jee Rah, Anne-Catherine Frey,Language services:Email: info@sight<strong>and</strong>life.orgSvenia Sayer-Ruehmann,transparent, Berlinwww.sight<strong>and</strong>life.orgJane BadhamOpinions, compilationsISBN 978-3-906412-65-8Communication consultancy<strong>and</strong> figures contained in<strong>and</strong> text writing:the signed articles doThe Corporate Storynot necessarily representthe point of view of<strong>Sight</strong> <strong>and</strong> <strong>Life</strong> <strong>and</strong> aresolely the responsibilityof the authors.Photo creditscover: Mike BloemPhotographypage 4,5: Mike BloemPhotographypage 11,17: Mike BloemPhotographypage 64,66:Neil Palmer (CIAT)page 85: UNAIDS
Buildingbridgesfor betternutrition.