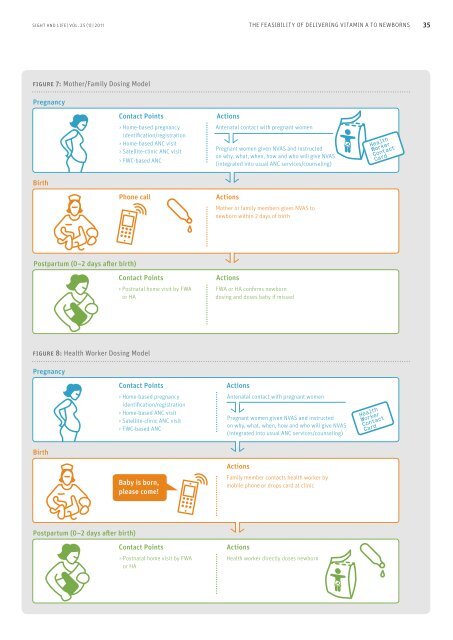
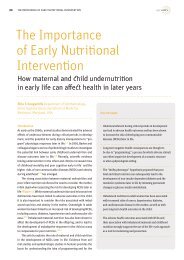
34 THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNSfigure 5: Map of districts in Bangladesh whereNVAS is being pilotedNilphamariJaldhaka<strong>and</strong> DimlaupazilasIndia(WestBengal)PirojpurSadar <strong>and</strong>Nesarabadupazilas0 25 50 KilometersTangailJaldhaka<strong>and</strong> DimlaupazilasIndia(Assam)India(Tripura)Myanmar(Burma)<strong>and</strong> home- or clinic-based antenatal (ANC) visits (Figure 7). Inaddition to key ANC services <strong>and</strong> messages, pregnant womenreceive an individually packaged dose of vitamin A (50,000 IU),<strong>and</strong> are instructed about why, when, <strong>and</strong> how to administer thedose to their newborns, <strong>and</strong> how to manage potential side effects.This information is accompanied by a counseling card<strong>and</strong> a “Health Worker Contact Card” that includes the name,cell phone number, <strong>and</strong> address of the local health worker. Thepotential advantage of this model is that the VA supplement isin the home at the time of delivery, <strong>and</strong> does not require thenotification of or waiting for the arrival of a health worker toadminister the dose.2. The “Health Worker Dosing” model also uses FWAs <strong>and</strong> HAs;however, the mother or a family member must contact the healthworker at the time of birth <strong>and</strong> the health worker must visit themother <strong>and</strong> her newborn to directly administer the vitamin A(Figure 8). To facilitate birth notification, health workers informpregnant mothers about the importance of early birth notificationso that the baby can obtain newborn vitamin A <strong>and</strong> otheressential newborn services. In this model, a “Health WorkerContact Card” is also provided to promote prompt <strong>and</strong> directcommunication with the health worker.Monitoring <strong>and</strong> evaluation. Monitoring the pilot activitiesinvolves a two-pronged strategy consisting of (1) routine datacollection within the MoHFW system; <strong>and</strong> (2) special monitoringinterviews <strong>and</strong> observations conducted by locally hired“extenders” to assess how well NVAS is being integrated intoexisting ANC <strong>and</strong> postpartum visits, <strong>and</strong> to assess communityacceptability (Figure 9). Two cross-sectional surveys in eachprogram upazila, or region, at baseline <strong>and</strong> at six months afterimplementation (i.e. end-line), will be conducted among recentlydelivered mothers to assess coverage <strong>and</strong> timeliness of thedelivery of newborn vitamin A. In addition, community healthworkers (CHW) will be surveyed at baseline <strong>and</strong> end-line toassess knowledge, attitudes, <strong>and</strong> practices about integratingNVAS into existing services.figure 6: NVAS design workshop participantsin Bangladeshdesign workshop, including national, district <strong>and</strong> sub-districtlevel health <strong>and</strong> family planning managers, was held in October2010 (Figure 6) <strong>and</strong> proposed two delivery platforms:1. The “Mother / Family Member Dosing” model in Bangladeshuses two cadres of community health workers: The “Female WelfareAssistant” (FWA) <strong>and</strong> the “Health Assistant” (HA), who integratesNVAS into routine home-based pregnancy surveillanceConclusionsBoth Nepal <strong>and</strong> Bangladesh have made important strides in bridgingthe research-to-program gap by examining scientific evidence<strong>and</strong> its relevance within each country’s context, establishingpolicies that permit feasibility testing of this new intervention,<strong>and</strong> closely monitoring <strong>and</strong> evaluating NVAS implementationbefore formulating a policy for national scale-up. From preliminarydata, implementation challenges facing NVAS are similar tothose faced by other interventions that target pregnant women<strong>and</strong> newborns. These include identifying <strong>and</strong> reaching a highproportion of pregnant women <strong>and</strong> their newborns in a timelymanner, overcoming geographic, travel <strong>and</strong> time constraints
SIGHT AND LIFE | VOL. 25 (1) | <strong>2011</strong> THE FEASIBILITY OF DELIVERING VITAMIN A TO NEWBORNS 3535figure 7: Mother/Family Dosing ModelPregnancyContact Points> Home-based pregnancyidentification/registration> Home-based ANC visit> Satellite-clinic ANC visit> FWC-based ANCActionsAntenatal contact with pregnant womenPregnant women given NVAS <strong>and</strong> instructedon why, what, when, how <strong>and</strong> who will give NVAS(integrated into usual ANC services/counseling)BirthPhone callActionsMother or family members gives NVAS tonewborn within 2 days of birthPostpartum (0–2 days after birth)Contact Points> Postnatal home visit by FWAor HAActionsFWA or HA confirms newborndosing <strong>and</strong> doses baby if missedfigure 8: Health Worker Dosing ModelPregnancyContact Points> Home-based pregnancyidentification/registration> Home-based ANC visit> Satellite-clinic ANC visit> FWC-based ANCActionsAntenatal contact with pregnant womenPregnant women given NVAS <strong>and</strong> instructedon why, what, when, how <strong>and</strong> who will give NVAS(integrated into usual ANC services/counseling)BirthPhone callBaby is born,please come!ActionsFamily member contacts health worker bymobile phone or drops card at clinicPostpartum (0–2 days after birth)Contact Points> Postnatal home visit by FWAor HAActionsHealth worker directly doses newborn