The Autism Spectrum Disorder Service Guideline.pdf - CTE - Online ...
The Autism Spectrum Disorder Service Guideline.pdf - CTE - Online ...
The Autism Spectrum Disorder Service Guideline.pdf - CTE - Online ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
World Energy Outlook SeriesWorld Energy Outlook – 1993World Energy Outlook – 1994World Energy Outlook – 1995Oil, Gas & Coal Supply Outlook – 1995World Energy Outlook – 1996World Energy Outlook – 1998World Energy Outlook – 1999 InsightsLooking at Energy Subsidies: Getting the Prices RightWorld Energy Outlook – 2000World Energy Outlook – 2001 InsightsAssessing Today’s Supplies to Fuel Tomorrow’s GrowthWorld Energy Outlook – 2002World Energy Outlook – 2003 Insights (forthcoming)Global Energy Investment OutlookWorld Energy Outlook 2002
Some children will come to the system with a diagnosis of ASD. This diagnosis makesthe child automatically eligible for Birth to Three services, although it is important for allparties to realize that the law requires that the IFSP team determines appropriateservices for the child. Diagnosis of ASD by qualified personnel is a valuable service;“prescriptions” for Birth to Three service are confusing and may actually slow down theprocess of developing a quality plan and program for the child.When children over 16 months of age who do not have a diagnosis of autism are referredto the Birth to Three System, the receiving program will screen the child for ASD as partof the intake process, even if the parent and/or referral source have no concerns aboutautism. (All screening and evaluation done by Birth to Three is voluntary and requiresprior written consent.) Preferred screening instruments include the Brief Infant ToddlerSocial-Emotional Assessment (BITSEA) (7) and the Modified Checklist for <strong>Autism</strong> inToddlers (M-CHAT). (8) If there are questions about the child’s overall communicationdevelopment and the program chooses to use the Communication and Symbolic BehaviorScales Developmental Profile (CSBS DP Infant-Toddler Checklist), the results may beused in lieu of conducting an additional autism screening. This instrument is appropriatefor assessing potential risk for autism in children as young as six months. (9) <strong>The</strong>se threescreening tools can be found in Appendix 3.<strong>The</strong> American Academy of Pediatrics is recommending the administration of screening forASD twice for all children before their second birthday. If a child has had a recentscreening done as part of routine medical care, the screening results may be used in lieuof conducting an additional autism screening. (10)At this time there are no reliable screening instruments for children younger than 16months of age for ASD. As the field advances, many experts are anxious to be able toreliably identify autism in children younger than 16 months old, but until the screeningtools can accurately provide guidance about which children are appropriate for furtherevaluation, their use is unprofessional and can lead to harmful mislabeling of children orfalse assurance. When additional factors exist, such as older siblings or parents withASD, Birth to Three programs are encouraged to carefully observe the child’sdevelopment in the areas of social interaction, communication development and thepresence of stereotypical and/or repetitive behaviors and develop an appropriate plan ofservices. <strong>The</strong> CSBS DP Infant-Toddler Checklist may be used as an indicator of risk.When the screening tool indicates that the child may have ASD, the general Birth toThree Program will encourage the family to seek a determination of whether the childmeets the classification of autism under the IDEA. All of the autism-specific programs areequipped to carry make these determinations, but in some cases they may be made bythe general program that has assessed the child, or a referral might be made to anotherqualified expert. This determination consists of four parts:A. An in depth review of the autism screening to reduce the likelihood that “red flags”identified as part of the screening were not the result of factors other than ASD. Ifthe family and the reviewer(s) agree that the screening results probably do notindicate ASD, services can only be delivered by one of the general programs, andthese guideline does not apply, except insofar as it offers overall guidance on goodearly intervention practice;4CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
B. If it is determined that the screening does indicate the need for further assessment,the administration of a validated assessment measure such as the <strong>Autism</strong>Diagnostic Observation Schedule (ADOS) (11) (for children 12 months and older),the <strong>Autism</strong> Diagnostic Interview-Revised (ADI-R) (12) (for children 24 months andolder), or the Childhood <strong>Autism</strong> Rating Scale (CARS) (13) (2+ years) by aprofessional or professionals with appropriate training; andC. A review of other assessment materials to assure that the child demonstrates of adelay greater than 1 standard deviation below the mean in receptive language,expressive language, social-emotional or adaptive behavior skills.D. If parents and the assessors agree that the child’s overall behavior anddevelopment are at odds with the other information gathered in this determinationprocess, informed clinical opinion may be used to override the recommendationthat the child receive autism specific services. Typically, such a child would bereassessed in three months.This determination process will not only help the family understand their child’s needs butalso help define how Birth to Three services may be delivered to the child. Based onvarious scenarios (summarized below) the child can receive individualized autism specificservices as outlined in this <strong>Service</strong> <strong>Guideline</strong>.• A child may receive a diagnosis of ASD prior to referral. In that case, the familywill be offered a choice of one of the autism-specific programs or one of thegeneral programs serving their town of residence. Since the child is alreadyknown to be eligible because of a diagnosed condition, whichever programreceives the referral will perform an initial multi-disciplinary assessment in all fivedevelopmental domains and a family assessment prior to developing the IFSP.• A child may be referred directly to an autism-specific program from ChildDevelopment Infoline, because the referral source is concerned that the child mayhave ASD, but there has not been a diagnosis. In that case, the autism-specificprogram must determine 1) whether the child is eligible for Birth to Three basedon developmental delay and/or 2) whether the child has a DSM-IV TR diagnosisof ASD or meets the educational classification of autism under the IDEA. If a childis determined to have the DSM-IV TR diagnosis of ASD or meet that educationalclassification of autism, the parent will be offered the choice of remaining with theautism-specific program, choosing a different autism-specific program that servestheir town, or choosing one of the general Birth to Three programs that servestheir town, as long as the program they choose is open to accept new referrals. Ifthe child is eligible due to a developmental delay but is not determined to haveASD or meet the educational classification of autism under the IDEA, the familywill be offered a choice of one of the general Birth to Three programs that servestheir town. If the child is neither eligible due to a developmental delay nordetermined to meet the educational classification of autism under the IDEA, theparents will be told that the child is not eligible and offered resources outside ofthe Birth to Three System, such as Help Me Grow (a developmental monitoringand resource referral program for children at-risk funded by the Children’s TrustFund) or private services.• A child who has already been determined eligible by a general program may bereferred to an autism-specific program that serves the child’s town of residence toCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 20085
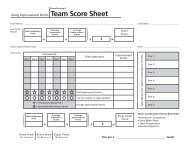
determine if the child meets the educational classification of autism under theIDEA. In this case, the autism-specific program will only need to assess the child,not evaluate the child to determine if the child has a significant developmentaldelay. If the child is determined to either have ASD or meet the educationalclassification of autism under the IDEA the parents will be offered the choice of: 1)transferring to the program that completed the ASD assessment, 2) choosing adifferent autism-specific program that serves their town and is open to accept newreferrals, or 3) choosing one of the general Birth to Three programs that servestheir town, as long as the program they choose is open to accept new referrals.Alternatively, the general Birth to Three program that conducted the initialassessment may carry out the determination.• Even though a child is not found to be eligible for Birth to Three services, thescreening indicates there is concern about ASD. In this case, the family will begiven the opportunity to have one of the autism-specific programs, do furtherassessment to determine if the child meets the educational classification ofautism. If so, then the child can receive individualized autism-specific services asoutlined in this <strong>Service</strong> <strong>Guideline</strong> from an autism-specific program.MAKING A CHOICE:Families may wonder why the Birth to Three System has both autism-specific programsand general programs. Assuring that we have the capacity to provide high qualityservices to children with ASD and their families is a priority of the system. <strong>Autism</strong>specificprograms were developed to assure that there were adequate resources to meetthis need throughout the state. Our general programs have traditionally served childrenwith ASD, and have expertise in this area as well. A family may already be enrolled in ageneral program or be familiar with one or make a strong positive connection with theevaluators from a general program who came to their home to conduct the Birth to <strong>The</strong>eevaluation. In any of these cases, developing an IFSP to receive services in accordancewith this <strong>Service</strong> <strong>Guideline</strong> with the general program may be the best choice. Parentsmay wish to contact autism-specific and general programs that serve their town in orderto make an informed choice about which program is best for their family.<strong>The</strong> chart on the next page illustrates many of the possible pathways that may be followedin the determination process.6CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Referral to Child Development InfolineChildalready diagnosedwith ASD orsuspected?YesNoParent selectsautism-specificprogram?GeneralEI ProgramYesNoPerforms initialevaluation andscreens for ASD<strong>Autism</strong>-Specific EIProgramPerforms initialmulti-disciplinaryassessmentYesChildeligible dueto delay?NoDevelopsIFSPScreeningIndicatesred flagsfor ASD?YesNo<strong>Autism</strong>-Specific EIProgram(if parent selects)If eligible,develop IFSP.If not, exit child andrefer to Help MeGrowYesChilddiagnosed w/ASDor determined tomeet educ.classification forautism?NoDevelops IFSPTransfer child to general program ifeligible. If not eligible, exit childand refer to Help Me GrowCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 20087
This process is not one that only happens at the time a child is referred to Birth to Three.If, at any time, a parent, a Birth to Three provider, the referral source, a care provider, orsomeone else who knows the child observes that a child is having difficulty withdeveloping meaningful communication or is regressing in communication skills, hasissues with social reciprocity, and/or is limited in development by repetitive behaviors, itis essential that the team have a discussion with the family about the advisability ofrepeating the ASD screening. This may be a more difficult discussion than the one thatwas held initially, since it will arise as the result of concerns rather than as a routineprocedure. Birth to Three staff must be prepared to have a well-thought-out, helpful,professional, and supportive conversation with a family about a challenging topic.Postponing this conversation, not allowing adequate time for the parent to reflect on it,excluding family members, or being equivocal can have serious negative consequencesfor the child, family, and program.<strong>The</strong> purpose of this determination process is to assure that children who meet theeducational classification of autism under the IDEA have access to services provided byautism-specific programs (when the system grows to have adequate capacity throughoutConnecticut) or, if families prefer, by general programs. It is expected that theadministration of these tools by qualified professionals will provide adequate clinicalinformation about a child’s ASD to develop an IFSP.PURSUING A MEDICAL DIAGNOSIS OF ASDIt will be common for there to be interplay between the potential identification of a childmeeting the educational classification of autism under the IDEA and the medicaldiagnosis of autism, which occurs in consultation with the child’s primary care physician.<strong>The</strong> Connecticut Birth to Three System strongly supports working with the child’s healthcare provider around issues of autism. <strong>The</strong> American Academy of Pediatrics hasprovided pediatricians extensive and specific guidance on autism screening anddiagnosis. (14)Pediatric practices may have resources to carry out further screening and comprehensiveevaluation, and/or may wish to refer the child to appropriate specialists. <strong>The</strong>ir choice of apractitioner, along with the payment source, should be reflected on the IFSP in the “OtherChild Related <strong>Service</strong>s” section.<strong>The</strong> Birth to Three System recommends that a developmental pediatrician, neurologist,child psychiatrist, or a licensed clinical psychologist complete the diagnostic evaluation.<strong>The</strong> American Speech-Language-Hearing Association (ASHA) policy is that aspeech/language pathologist with expertise in ASD’s may perform autism diagnosticevaluations. Regardless of the area of specialty, an accurate diagnosis requires that theprofessional has training and experience in the area of ASD.8CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Components of a Medical Diagnostic AssessmentMedical assessment for ASD should confirm the diagnosis as well as provide informationabout the strengths and learning challenges of the child. It can be helpful in planning forintervention. <strong>The</strong> components of an evaluation for ASD should include:1. Developmental, medical (see Appendix Five), and three generation familyhistory2. Careful physical and neurological examination3. Developmental evaluation4. Assessment of social interaction, verbal and nonverbal communication, andrepertoire of activities and interests and play behavior against the DSM IV TRcriteria for autism5. Audiological evaluation6. Assessment of family functioning including strengths, resources, stressors andsupport needs, both emotional and financial.7. If there is global developmental delay, the child should have chromosomeanalysis and DNA testing for Fragile X.8. Additional targeted medical assessment is based on clinical presentation. Thisincludes additional laboratory studies, EEG, MRI, etc.A specific autism assessment tool is highly recommended but not required to make thediagnosis. Examples of some assessment tools are included in Appendix Four. Foryoung children identified with ASD, timelines for a re-evaluation should be determined. Achild who is assessed at 16-24 months should be reassessed in one year.Decisions about additional medical evaluations or referrals for medical follow-up mustoriginate from the child’s primary health care provider. Appendix Five lists the types ofBirth to Three System encourages families to work with their health care provider toobtain medical diagnostic services (See Appendix Five). Medical follow-up is not aservice covered by Birth to Three. When a child is identified as meeting the educationalclassification of autism, Birth to Three will seek parent permission to share thisinformation with the child’s medical provider because medical follow up is very importantfor children with autism.Additional information on early indicators of ASD is found in Early Indicators forScreening - Appendix Two. Additional assessment tools for ASD are listed in AppendixFour.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 20089
PRINCIPLES OF INTERVENTION FOR YOUNG CHILDREN WITHAUTISTIC SPECTRUM DISORDER<strong>The</strong> following principles should be used when developing an intervention program forchildren who have been identified as meeting the educational classification of ASD.Because there is such variation in this disorder, it is unlikely that one interventionapproach will benefit all children equally. Two children with ASD can perform verydifferently from one another. Likewise, two families who have children with ASD havevery different needs. <strong>The</strong> following information is organized according to a list of basicprinciples of intervention that will apply to all young children with characteristics of autisticspectrum disorders. (15)Principle 1: <strong>The</strong> earliest possible start to intervention is essential.Principle 2: <strong>Service</strong>s must be individualized for children and families.Principle 3: Children with ASD require intensive engagement.Principle 4: Family involvement and participation is critical.Principle 5: Intervention is based on a developmental curriculum designed toaddress the specialized needs of a child with ASD.Principle 6: Intervention is planful and systematic.Principle 7: Challenging behaviors are addressed using positive behavioralsupport.Principle 8: Intervention should focus on developing communication skills.Principle 9: <strong>The</strong> development of social relationships is based on a child’s abilityto play and interact with others.Principle 10: <strong>The</strong> transition from the Birth to Three System to preschool specialeducation and related services should be well planned.Principle 1<strong>The</strong> earliest possible start to intervention is essential.Children who receive appropriate services earlier achieve better results. One of the mostexciting accomplishments in the field of ASD is the ability to recognize and treat thedisorder at a very early age. Routine screening can identify risk for ASD in children whoare 16 months and older. <strong>The</strong> earlier children receive intervention, the more positive theoutlook for their future. Research on treatment for ASD is encouraging. Althoughcharacteristics of ASD may be life-long, having ASD is no longer considered a barrier to afull and happy life. Today people with ASD, including those with complex challenges, canbe found living in communities, attending neighborhood schools, and working as adults.Principle 2<strong>Service</strong>s must be individualized for children andfamilies.“Individualization” means that each child and family’s services are based on that child’sneeds, strengths and interests and the family’s concerns, priorities and resources. Thisis different for each child and family because each child and family is different. <strong>The</strong>development of the intervention plan known as the Individualized Family <strong>Service</strong> Plan(IFSP) and ongoing changes in the plan will be done with the family. Families have adecision-making role as members of the intervention team. <strong>The</strong> team will determine whowill be involved in the program, when services will take place and what will be the focus10CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
of the services. This guideline introduces families to the framework for intervention toguide them in this discussion. Families will determine how they will be involved inimplementing their child’s IFSP. Even though the intervention may have a specificcurriculum, the daily activities and routines are individualized step by step andcustomized for each family. However, it is not possible for families to assign the processof “treating” ASD to the Birth to Three staff. Research on child development has shownthat toddlers do almost all of their learning between early intervention visits as theyinteract with their caregivers in a variety of social and physical environments (16) .Principle 3Children with ASD require intensive engagement.By the very nature of the disorder, we know that children with ASD spend little of theirown time engaged in purposeful, appropriate, goal directed behavior. <strong>The</strong>ir tendency isto be either disconnected from their surroundings or fixated on specific aspects of objectsor people. This restricts children with ASD from discovering and learning. Most childrenlearn from interacting with their environment through observation and imitation. <strong>The</strong>seopportunities may be lost to children with ASD.Engagement refers to the amount of time a child is attending to and actively interactingwith others. This happens during the time that the early intervention staff is working witha child. However, most of the engaged time occurs with family members, caretakers,friends, and peers outside of the time when Birth to Three is present. <strong>The</strong> earlyintervention staff works with the family to develop ways to keep a child with ASDengaged. <strong>The</strong> goal of intervention for the child with ASD is to increase the amount oftime he or she is engaged throughout the day in order to achieve the outcomes identifiedon the IFSP. <strong>The</strong> most intensive intervention program is of limited benefit if it does notresult in active engagement in the times when the child is not receiving services.In the past, the Birth to Three System has recommended 15-20 clock hours per week ofBirth to Three services for children with ASD. However, there is no research that we areaware of that has specifically been done with children in this age range that shows thatthis amount of service leads to the best possible outcomes. Existing researchemphasizes the importance of engaged time for the child, not the amount of hours ofservice provided by programs. (17) A poorly structured intervention plan may providemany hours of service that is in a one to one setting with an interventionist but is isolatedfrom the child’s family, peers, and everyday routines. A more effective plan may havefewer interventions, or interventions of shorter duration that allow full participation offamily members, caregivers, and peers. A plan like this will provide opportunities toreflect upon strategies to assure engaged time in multiple settings throughout the courseof the child’s day and week. Research demonstrating the effectiveness of massed trialshas been carried out on children older than three. Research about toddler learning stylesshows that they are not well equipped to generalize learning from massed trials inteaching settings to other settings. (18) This is not to say that the Birth to Three Systemrecommends low intensity plans for children with ASD. Rather, the point is that all tenprinciples articulated in this guideline are considered to be essential to creating andmaintaining good intervention programs for young children with ASD. An emphasis on aparticular number of hours of direct intervention in lieu of assuring a systematic approachemphasizing communication, social engagement, family involvement, positive behavioralsupport, and so on will likely not achieve the optimum outcome. Very young children,recently identified children, or children exhausted by overexposure to a variety ofCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200811
therapies and constant teaching will not be doing their best learning. Gradual introductionof intensive services, assuring that the child is comfortable with the early interventionistsand that that the proposed interventions are suitable is an essential component ofbuilding an intensive program. Finally, a family need not feel guilty if they find they arecomfortable with a lower intensity of services they may have heard about. In sum, for achild approaching the age of three who has been receiving early intervention for sometime, a program of 15-20 hours a week may be a reasonable rule of thumb, but it is onlyone of many considerations in service planning and implementation. And, to the extentthat the intensity of the intervention has the unintended consequence of diverting thechild’s caregivers from focusing on their role as the child’s primary teachers, intensiveprograms may actually impede the rate of developmental progress for the child.Programs in excess of twenty hours are not recommended because they are likely toprevent the child from having appropriate opportunities to experience essential learningwith family, caregivers, and peers within the context of natural routines andenvironments.Consistency is important and the team planning process should strive to assure thatintervention will occur on a predictable and routine schedule with attention to the numberof hours per day and week, number of weeks per year and the number of environmentswhere intervention occurs. <strong>Service</strong>s should take place 12 months a year. Vacations,holidays, inclement weather, staff illness, or other variations in the service calendarshould be discussed with a family well in advance and there should be writtendocumentation that the family understands and agrees with any scheduling changes thatare made.<strong>Service</strong> intensity should be based on the needs of the child and family. <strong>The</strong>determination that a child meets the educational classification of autism does not predictwhat frequency and mix of visits will most suit a particular child and family. Teammeetings are an important adjunct to Birth to Three services for children with ASD. <strong>The</strong>team may need to strike a balance between meeting time and time working directly withthe child, based on the realities of the family’s schedule, the child’s readiness andwillingness to receive intervention. Family members need to talk to their servicecoordinator if they feel there is too much time spent at meetings and not enough spentworking directly with the child. It must be emphasized that the intense early interventionservice is directed as much at caregivers and family members to assure that families canand will continue to use the same strategies throughout the child’s day.Intensive engagement takes place across many different natural learning environments.This includes the home as well as community settings where the child spends his or hertime. Families and Birth to Three staff must work together as a team to identify ways toexpand learning opportunities in a variety of settings and activities.Principle 4Family involvement and participation is critical.<strong>The</strong> mission of the Connecticut Birth to Three System is to help families meet thedevelopmental needs of their infants and toddlers (See Appendix One). Families arethe first and most important teachers for their child. <strong>The</strong>y are the constant in a child’s life.Infants and toddlers learn as they experience life with their families. Birth to Three canhelp make sure that this learning is designed to meet the child’s developmental needs.<strong>Service</strong> systems and personnel will change over time, but families maintain the continuity12CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
from day to day and year to year. Families become lifelong advocates for their child.<strong>The</strong> partnership between Birth to Three and the family begins when the family places acall to Child Development Infoline because of concerns about their child’. Throughout theeligibility determination process and the developing of outcomes for the IFSP, the familyidentifies how their child functions in family life and routines and what areas are mostimportant to work on. <strong>The</strong> IFSP process describes the roles of service providers, familymembers, and others in achieving the family identified outcomes. <strong>The</strong> Birth to ThreeSystem will provide families with education, support, and guidance to help them developthe skills necessary to help their child with ASD reach his or her potential.<strong>The</strong> provision of Birth to Three services is only a small part of the process of helping achild with ASD develop. Family members and early interventionists work togetherconstantly to connect what the child is doing with family life to the content of the visits.Active dialogue between interventionists and parents, modeling and practicing duringvisits, tailoring carry-over strategies to changes in the family and child’s life, designingand carrying out manageable record keeping systems are all parts of the Birth to Threeexperience. Family members and team members together can determine when it is timeto consider revising the IFSP, what to work on next, and how to change activities orstrategies that have not been as successful as hoped. Visits need to be scheduled attimes and in ways that family members can fully participate. <strong>The</strong> content of all visits mustbe directed to assuring that family members and other caregivers acquire the skills andresources to help the child develop. It is almost certain that progress toward outcomeswill be slower if families are not an active part of every part of the Birth to Three processincluding home visits. Families need to be actively involved in their child’s program in thefollowing ways:1. planning and deciding what services their child will receive.2. evaluating child progress.3. training and assisting with activities of daily living and developing strategies foraddressing the IFSP during daily routines.Principle 5Intervention is based on a developmental curriculumdesigned to address the specialized needs of the childwith ASD.Curriculum for children with ASD is based on widely accepted principles of childdevelopment. <strong>The</strong> instructional program builds on these principles and the child’sindividual strengths while also addressing their weaknesses. <strong>The</strong> curriculum for a childwith ASD needs concentrated or specialized instruction to address the areas of language,social interaction, play skills and interests. <strong>The</strong> essential areas for a specializedcurriculum for a child with ASD include:1. attending to and staying engaged in the environment, especially to otherpeople and learning opportunities;2. imitating others, including both verbal and motor imitation. Imitation is seen asa fundamental tool for learning;3. using verbal and non-verbal communication such as gestures, vocalizationsand words;4. understanding and using language to communicate;5. playing appropriately with toys;6. playful interaction with others;CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200813
7. reciprocal interactions;8. spontaneous interactions;9. making choices and,10. following daily routines and variations in routines.Principle 6Intervention is planful and systematic.Systematic intervention or instruction is carefully planned and consistent. It involvesassessing, planning, teaching and measuring progress with each intervention step. Eachstep is coordinated toward a meaningful set of outcomes or goals. <strong>The</strong> only reliable wayto determine if our teaching is effective is to be systematic and to measure progress on aregular basis. It is important to note that many indicators that are easiest to measure,such as vocabulary, intelligibility of words, or duration of eye contact may not be asmeaningful or important to the family as the sense of the over all quality of the child andfamily’s quality of life such as reduced frequency or tantrums, ease of transition betweenhome and other settings, or the ability of family members to spend quality time together.Systematic instruction relies on intervention decisions that are driven by data collection.Data is used to measure the change in a behavior over time. Data may be taken on thefrequency (how often) a behavior does or does not occur, the duration (how long) abehavior does or does not occur, and the range of a behavior (how much support orprompting a child needs). In order to use data in reviewing the effectiveness ofintervention the following must happen:1. An assessment is completed prior to intervention;2. outcomes and objectives are written in measurable terms. <strong>The</strong>re must be aspecific description of the desired behavior;3. data on outcomes and objectives are taken prior to intervention and used as abaseline for intervention;4. steps or tasks towards outcomes are analyzed and defined;5. instructional strategies and supports are identified (e.g. where, when, withwhom, level of support);6. methods for motivating or reinforcing the desired behaviors are identified;7. methods and timelines for measuring progress are determined;8. data is taken and analyzed on a routine basis; and,9. adjustments in intervention plans are made based on analyzing progress onthe IFSP.Sometimes when teams are eager to assure that a child is receiving intensive services,they develop service plans with many hours of service without following the processoutlined above. An IFSP that is developed after a child has met the IDEA classification ofautism may be a very short term plan that focuses on finishing any assessments,developing outcomes and objectives, gathering preliminary data, and identifying stepsand tasks that will be carried out to meet the outcomes. At this point (step five above) theteam would meet again and identify what the intensive intervention would look like. <strong>The</strong>IDEA requires that IFSPs be reviewed at least every six months, but in most cases it isexpected that these more complex plans will be revisited more frequently as part of theteam meeting process.14CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Ongoing collaboration between the family and service providers in the analysis of dataand flexibility in adjusting strategies is a key to successful teaching and learning.Continuation of ineffective strategies or relying on techniques merely because they havebeen shown to be effective with other children may be harmful. Many intervention teamsfind that a regularly scheduled meeting of all team members (including the family) isimportant to review data, maintain consistency in intervention, and make timely changesin the intervention.Principle 7Challenging behaviors are addressed using positivebehavioral support.Positive behavioral support is a set of principles that frame the way we think about andrespond to children and their behavior. <strong>The</strong> principles are grounded in the appreciationof each child’s strengths and challenges. To practice positive behavioral support meansgetting to know the whole child and assuming his or her behavior has meaning and thatthe behavior is a form of communication. It requires recognizing that children developand respond best when they are respected and supported to enjoy relationships andmake choices. Challenging behaviors displayed by children with ASD are complex andmay create frustration and confusion for those who interact with the child. Behavior mayrange from aggression, tantrums, or self-injury to withdrawal or repetitive, stereotypicalactions. Some of these behaviors also occur in children who are typically developing.For children with ASD we see behaviors that are extreme, occur more frequently, or aremore disruptive to development. Although some behaviors occur for medical or otherreasons the majority of challenging behaviors occur because of:1. social misunderstanding;2. communication frustration;3. discomfort with the physical environment;4. anxiety;5. intense preoccupations or interests.Before developing a plan to address problem behavior, a thorough assessment of thebehavior must take place. This assessment, which may be referred to as a “functionalbehavioral analysis” is completed by the intervention team and helps them to understandwhat happens before the behavior occurs. <strong>The</strong> assessment is designed to answerquestions such as “Why is the behavior happening?” “When does the behavior occur?”“What function does the behavior serve?” “Is the behavior preceded by any biological,environmental, sensory, and/or emotional conditions?” <strong>The</strong> assessment will also look atwhat happens after the behavior occurs. “How do people respond to the behavior?” <strong>The</strong>assessment helps the family understand how their response to the child’s behavior mayincrease or decrease the behavior.Once the assessment is completed, a positive behavioral support plan is developed. <strong>The</strong>plan includes developing strategies to keep the behavior from occurring, providing thechild with new skills to replace the undesirable behavior, and assisting caretakers torespond to the behavior in new ways. <strong>The</strong> ultimate goal of the plan is to help the childand family gain access to new environments, have positive social interactions, developfriendships, and learn new communication skills. <strong>The</strong> result of the support should be thatthe child has fewer problem behaviors and more ways of interacting with others. (19)CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200815
<strong>The</strong> plan will often include strategies to address communication. A child whosecommunication skills are limited will be frustrated due to the inability to convey needs andwants. This is a cause for socially unacceptable or challenging behaviors. <strong>The</strong>refore, theintervention plan will include development of an effective communication system for thechild (See Principle 8.)<strong>The</strong> plan may also include strategies to address sensory problems that may co-occurwith autism. Many individuals with ASD display different or atypical reactions to commonsensory experiences. <strong>The</strong>re may be an over-reaction or under-reaction to sights,sounds, touch, movement, body position/awareness and the pull of gravity. Due to this,the individual may become over-aroused, display discomfort, complain, withdraw orengage in some sensory related behavior. This results in problem behavior.Intervention to address sensory related behaviors is called Sensory Integration (SI)<strong>The</strong>rapy. Individuals who have difficulty processing and regulating sensory informationare challenged by difficulties with attention, learning, and social interaction. <strong>The</strong>re is noresearch that indicates that sensory integration therapy has any direct impact on ASD.However, sensory issues may be particularly overwhelming to children with ASD, sotreatment that addresses them may prove to be helpful. Sensory Integration therapystrives to reduce the child’s preoccupation with his/her sensory needs by satisfying thesensory craving, reducing the stimuli in the environment and increasing the tolerance forsensory stimulation. Once able to regulate the sensory input, the child is more availablefor engagement and learning opportunities. (20)Principle 8Intervention should focus on developingcommunication skills.<strong>The</strong> importance of having an effective communication system cannot be underestimated.A first step in addressing communication issues with children who are suspected ofhaving ASD is to assure that their hearing has been reliably tested. Hearing or analternative to hearing is a critical component of communication. An observer may notknow if a hearing loss is causing autistic behavior, autism makes it seem as if a child hashearing loss, or if a child has both autism and communications issues. Obtaining anaccurate hearing assessment of a child with ASD can be challenging.Communication is much broader than simply talking to one another. A goodcommunicator uses verbal as well as non-verbal behavior to engage a listener. Childrencommunicate to let their needs known long before they can talk. As children develop,their non-verbal communication (i.e. pointing to desired object, lifting their hands to bepicked up) becomes natural and is understood by others. Children with ASD, whetherverbal or non-verbal, must develop some type of communication system in order to besuccessful socially. <strong>The</strong>y must be able to communicate in a manner that others willunderstand. Toddlers with autism may often have large vocabularies or imitate spokenlanguage well, but lack joint attention skills or functional use of language tocommunicate.16CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Alternative or augmentative communication systems are one way to assist children whohave limited verbal language. <strong>The</strong> type of communication system used will varydepending on the child and the activities and environments in which he or she spendstime. <strong>The</strong> system may include simple gestures, sign language, objects, pictures, or anelectronic communication device. <strong>The</strong> use of an alternative system does not mean thatthe child does not develop verbal language skills or speech. <strong>The</strong> communication systemis used as an aid to improve communication and speech, increase social interactions,and provide structure to daily activities or routines. Children with ASD are oftensuccessful with picture communication systems because they tend to have strong visualskills. If a child has difficulty understanding spoken communication, pictures are oftenused to give more information. For example, a child may be offered a choice of what hewants to play with by showing him two pictures. <strong>The</strong> child will choose what he or shewants by pointing to the picture or handing it to the adult. <strong>The</strong> purpose of an alternativesystem is to expand the ways in which the child can interact with and be understood by avariety of people.One of the more common alternative communication systems used with children withASD is the Picture Exchange Communication System (PECS). (21) PECS was developedto allow children and adults with ASD and other communication deficits to initiatecommunication. PECS begins by teaching a child to exchange a picture of a desireditem with an adult to request something. <strong>The</strong> system goes on to teach discrimination ofsymbols and then puts them all together in simple "sentences." Many young childrenusing PECS also begin developing speech. <strong>The</strong> same is true for children who learn signlanguage. <strong>The</strong>re are some who conclude that signs are even more likely to promotespeech, since each word has its own motor movement, whereas the motor movementwith every picture is the same, a point. (22)Whether a child is using an alternative communication system or not, the following skillsshould be included in a communication curriculum for children with ASD:1. look at person when name is called;2. look at objects when they are labeled;3. attend to a speaker;4. use eye contact to maintain interaction;5. imitate simple actions, sounds words, songs or finger plays;6. gain someone’s attention;7. manipulate a person or object to ask for something;8. point;9. combine pointing with looking at a person to ask for something;10. request “more”;11. tell someone you are “all done”;12. say “no” or refuse;13. greet others;14. say “yes” or agree;15. name things;16. name people;17. describe what others are doing.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200817
Principle 9<strong>The</strong> development of social relationships is based on achild’s ability to play and interact with others.In addition to difficulties with communication, young children with ASD typically lackappropriate interaction and play skills. Intervention for a child with ASD needs tospecifically address these skills.Before focusing on social interaction in play, the child needs to have some skills for usingtoys in a playful way. Usually children begin interacting with toys by playing bythemselves. To increase a child’s success while playing, the environment needs to beorganized. <strong>The</strong> physical space should be defined in a way that is clear for the child, forexample, sitting at a table or on a rug. <strong>The</strong> choices of toys and activities need to beplanned. <strong>The</strong> length of the play period and how to end the play session should bedetermined. Initial sessions for learning how to use toys may include simple actions ontoys such as dumping, pulling, and building. Once the child becomes more sophisticatedin his or her use of toys, he or she will move on to symbolic use of toys. This will includesimple imitation such as giving a baby doll a drink or talking on a play telephone.Social play begins when a child plays with a parent or alongside another child or siblingusing the same materials. This is referred to as parallel play. As the children interactwith materials, they learn to share materials and themes in a play routine. Moving intoplay that is more cooperative or social requires skills such as turn-taking and sharing.For children with ASD, these skills may have to be taught. Children develop from simplecooperative play to participation in small group activities. Again, for a child with ASD thisoften requires planning and support to be successful. Just placing a child with ASD in agroup setting with children is not sufficient. Often it is helpful to begin with a short,planned “play date.” <strong>The</strong> number of children should be limited to one or two familiarchildren and the environment should also be familiar. <strong>The</strong> toys that will be mostmotivating for the child with ASD should be identified and there should be sufficientnumber of toys for both children to have their own set.A child’s social behavior with adults and peers needs to be a focus of intervention. Thisfocus usually begins with child--adult interactions which, over time, become child--childinteractions.<strong>The</strong> basic structure for planning for social interactions should include the following:1. define the space;2. organize the choices, toys or materials;3. organize which materials are to be shared;4. organize the expectations of the activity;5. define the social expectations for the children;6. determine how long the activity will continue;7. determine how the activity will end.<strong>The</strong>se same guidelines can be used when introducing a child with ASD to a larger groupsetting such as a play group or nursery school class.It may also be helpful to use the same structure in planning community experiences forthe young child with ASD. Community settings may be difficult for the child with ASD18CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
ecause they are unpredictable. Although all aspects of a community outing cannot beorganized, establishing some of the above parameters will help the child stay calm andfocused throughout the experience. Community outings should begin in the presence ofa trusted adult. <strong>The</strong> goal is for the child to become familiar enough with the peers to becomfortable in the community or group setting with less adult support over time.Principle 10<strong>The</strong> transition from the Birth to Three System topreschool special education and related servicesshould be well planned.Children with ASD often have difficulty with change, including change experienced whenstarting something new and different. During the transition to a school based programthere will be changes in adults, children, settings, and routines. <strong>The</strong> child with ASD maybe so sensitive to change as to notice differences that others do not. <strong>The</strong>re aresignificant differences between the service delivery model used in the Birth to ThreeSystem and an educationally based program developed by a local school district.Planning and flexibility on the part of Birth to Three providers and preschool programsare necessary to assist families and children with adjusting to this change.When planning the transition from a Birth to Three program to a school program, thefollowing is helpful:1. the earliest possible notification to the local school district that the child isreceiving Birth to Three services. This should occur even before discussionsregarding transition take place. Early notification allows the school district toplan for the child with ASD. This may include identification of the appropriatestaff and resources needed as well as completion of any training staff mayneed;2. the earliest possible communication with the school district about the child andfamily’s strengths;3. details of the program that is in place and strategies that have beensuccessful;4. a focus on the family as well as on the child throughout the transition process.Cooperation between a Birth to Three program and the school district is essential foreffective transitions. Prior to the transition meeting that is held between 9 months and atleast 90 days before the child’s third birthday, it may be helpful to identify skills that canbe introduced at home but that will be helpful in a school based program. In addition,community resources for necessary family supports should be identified that may not beavailable from the school.Flexibility and creativity on the part of the school district and the Birth to Three programis needed for transitions to meet the needs of the child and family. For example, forchildren who turn three in the late spring or summer, the school may want to investigatewhether it is possible to have the services in the IFSP continue until September using theschool as a payment source. If the child is turning three early in the school year, it maymake sense for the school district to consider asking the Birth to Three program todeliver services in the school setting.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200819
Unfortunately, many children with ASD do not present their complex needs until veryshortly before their third birthday. If that is the case, Birth to Three providers must workdiligently to help parents understand the need to share information with the schooldistrict as soon as possible. Transition and transition activities should be a major focusof IFSPs for all children with ASD but especially for those nearing the age of three.School districts may wish to participate in joint evaluations or observations of the child. Itis important for Birth to Three programs to participate in early information-sharing withschool districts for all children with complex or challenging behaviors whether or not theyhave an ASD diagnosis.Parents and Birth to Three programs should be aware that the determination of eligibilityfor special education services under the classification of autism for children over the ageof three is made by the school district. <strong>The</strong>re may be instances where a child hasparticipated in an autism-specific Birth to Three program but is not considered to have“autism” by a school district. In cases such as this it is especially important for the Birthto Three Program to work with the school district and the family to assure a smoothtransition.APPROACHES TO PROVIDING SERVICES TO YOUNG CHILDRENWITH AUTISTIC SPECTRUM DISORDERS<strong>The</strong>re has been a great deal of publicity and controversy about what is the “best” way toaddress the needs of children with ASD. Several approaches have been widelypublicized. When parents learn that their child may have an ASD, they may come tobelieve that a certain “brand name” program is guaranteed to resolve all of the issuesassociated with the condition. Extensive research has been conducted about manyapproaches. “Children’s outcomes are variable, with some children making substantialprogress and others showing very slow gains. Although there is evidence thatinterventions lead to improvements, there does not appear to be a clear, directrelationship between any particular intervention and children’s progress. Thus, whilesubstantial evidence exists that treatments can reach short-term goals in many areas,gaps remain in addressing larger questions of the relationships between particulartechniques and specific changes.” (23)Further, while research has shown that early treatment is very beneficial, “early” isusually defined as three years of age or older. “It remains to be seen whether veryyoung children (i.e. 2 years or younger) will tolerate and benefit from teaching sessionsthat are as lengthy and structured as those commonly used with children 3 years andolder.” (24)In reality, the intervention strategies that work best for the young child with ASD arethose that fit a given child’s and family’s needs. A good plan will consider thedevelopmental strengths and needs and unique learning style of each child. One childmay require a high level of direct instruction, whereas another may be over-stimulated byit. Children with ASD learn in complex ways. <strong>The</strong>ir learning needs, like their autism,transform as they develop. In many cases, focusing exclusively on one approach ormethod of instruction, which might temporarily produce a desired result, could ultimatelyrestrict a child’s growth. Sometimes, however, there may be a rationale for temporarilyputting a significant effort into the development of a specific skill.20CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
It is useful to characterize the active ingredients of treatment approaches along acontinuum – from traditional behavioral approaches, such as discrete trial, to morecontemporary behavioral approaches that use naturalistic language teaching techniques,to developmentally oriented approaches.Behavioral ApproachesTo understand behavioral approaches to ASD, a clarification of terms is necessary. (24)In brief, behavior analysis is the study of behavior, behavior change, and the agents ofchange. Applied Behavioral Analysis (ABA) is the science of applying what is learnedfrom the analysis of behavior to understand the relationship between behavior andconditions. <strong>The</strong> behavior analyst uses data review to develop theories as to why aparticular behavior occurs in a particular context and then creates interventions to alterthe behavior(s). Information obtained from behavior analysis, therefore, is used topurposefully and systematically modify behavior.Applied Behavioral Analysis generally emphasizes four elements:1. antecedents (what comes before the targeted behavior such as instructions,demands, or corrections);2. behavior (which is observable and measurable);3. consequences (such as reinforcement); and,4. context (the setting conditions such as people, places, materials, activities, ortime of day.)Since the 1970s, the science of ABA has been used to create programs for individualswith autism that teach specific skills in a specialized sequence with the goal of increasingor improving socialization, communication, and general adaptive functioning. Suchtreatment, applied intensively in the toddler and preschool years, has been referred to asEarly Intensive Behavioral Intervention (EIBI). Although they are not synonymous, ABAis often used interchangeably with EIBI, particularly in the popular press. ABA also iserroneously perceived as a specific intervention technique rather than as an overallscience and service delivery mechanism used to establish, guide, and evaluate ongoingintervention.Among the ABA-based approaches for young children with autism developed to date,most are based on the research of Lovaas and others at the University of California, LosAngeles. This has led many to conclude inaccurately that the term “Lovaas therapy” canbe used interchangeably with ABA or other intensive behavioral treatments for autism.Within both broadly defined ABA-based interventions and more specific EIBI programs,numbers of techniques are used to accomplish treatment goals. <strong>The</strong>se often includetraditional behavioral techniques such as functional assessment, prompting, shaping,and reinforcement, as well as techniques specifically designed for the treatment ofautism (e.g. Discrete Trial Instruction).Discrete Trial Instruction (DTI) is a method of teaching children that was first adapted forchildren with autism by Dr. Ivar Lovaas and his colleagues at UCLA. This method ofinstruction includes multiple opportunities of intensive practice or “trials” where the childis taught to respond to a command or “stimulus.” Each practice session includes aCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200821
series of short, concise instructional prompts. <strong>The</strong> model emphasizes precision andorganization during instruction. This includes adult control over the learningenvironment, the use of prompting and shaping techniques, and reinforcement when thechild produces the correct response. <strong>The</strong> rationale for using DTI is the belief thatchildren with autism are unable to learn in natural contexts due to their specific learningand behavioral characteristics. (25)However, there are even variations in the uses of DTI. <strong>The</strong> more recent work of VincentCarbone and his colleagues advocate uses of discrete trials in which the curricularcontent is very specific to functional verbal behavior, the trials are usually mixed ratherthan massed, and the response time is very short. Verbal Behavior is an intervention thatis focused on language as a skill that can be analyzed and targeted according tobehavioral principles. That is, language is a behavior and can, therefore, be influencedby reinforcement and maintained through motivation. <strong>The</strong> use of language is directlyrelated to the value of the reinforcement that follows the communication attempt.Carbone, Sundberg, and Partington have used these teaching procedures to achievespontaneous language in children with autism. (26)Another behavioral approach is pivotal response training, which targets behaviors thatwill have widespread effects on development. (27)<strong>The</strong> difficulties cited with using a traditional behavioral model to enhance social andcommunication skills include the artificial nature of the instructional setting and the lackof a clear link between instruction and the social use of a skill. (28)<strong>The</strong>re is now a large body of empirical support for behavioral approaches usingnaturalistic teaching methods. <strong>The</strong>se behavioral programs are often carried out incommunity and home settings and are structured to take advantage of natural learningopportunities. Incidental teaching (29) such as the Little Walden Program at EmoryUniversity, which often takes place in a preschool classroom setting, is an example of abehavioral model of this type.Developmental Approaches<strong>The</strong>re are numerous intervention approaches based on a developmental framework.Although the empirical support for developmental approaches is more limited than forbehavioral approaches, there are several treatment studies that provide empiricalsupport for language outcomes using specific strategies built on a developmentalapproach (30, 31, 32, 33) and many case studies, with Greenspan and Wieder (34) providing thelargest case review. Developmental approaches share many common active ingredientswith contemporary naturalistic behavioral approaches and are compatible along mostdimensions. (35) A common feature of developmental approaches is that they are childdirected.Intervention emphasizes the development of skills through active explorationand positive social interactions, based on the belief that children acquire skills throughsocial interactions. <strong>The</strong>se approaches emphasize naturally occurring situations as thecontext for instruction. Intentionality and meaning are assigned to all of the child’sbehaviors. <strong>The</strong> rationale for using a developmental approach to enhance developmentin children with autism is based on the belief that the fundamental process of learning isthe same for all children, so children with autism are able to learn in natural contexts. (36)22CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
One of the developmental approaches commonly used is the relationship-based model,also called “Floor Time” and DIR, which was developed by Dr. Stanley Greenspan.Structured teaching (e.g. TEACCH) is a cognitively-based approach to teaching self careskills and managing disruptive behavior. (37)Another developmental model SCERTS (Social Communication, EmotionalRegulation, Transactional Support) This model, developed by Prizant, Wetherby, Rubin,and Laurent, is intended to provide a flexible, yet comprehensive multidisciplinary planfor children with ASD. Goals, specific objectives, progress ratings and evaluationprocedures are recommended with an emphasis on developing goals that address thecore deficit areas of children with ASD. <strong>The</strong> model addresses Social Communicationgoals and, Emotional Regulation. It uses Transactional Supports include the visual andorganizational supports children with ASD commonly need, support to families and staff,and the supports necessary to facilitate social interactions with partners. (38)Limitations to the socio-communicative approach include inconsistency in the number oflearning opportunities that occur depending on the skills of the interventionist and thedifficulty some children have in a distractible learning environment. Documentation ofprogress may also be less specific than in a behavioral approach.“<strong>The</strong> conceptual differences between developmental and behavioral approaches tointervention are real, yet the gaps in practice appear to be narrowing. Developmentalresearchers may criticize behavioral approaches for failure to target the specific deficitsassociated with autistic spectrum disorders, “ (39) and it has been argued that this failure toselect target skills within a meaningful developmental framework results in isolated skillsthat are difficult to transfer to other situations and skills. (40) Behaviorists counter that theirregularity of skill development in children with ASD decreases the relevance of carefuladherence to normal developmental sequencing. (41) However, “developmentalapproaches to ASD treatment have incorporated methods that recognize the needs ofchildren with ASD for high levels of structure, adult attention and consistency. At thesame time, behavioral interventions are increasingly being used to address complexsocial and communication goals in normal environmental settings.” (42)Relationship Based ApproachesIn recent years, experts have found promising results in using relationship basedapproaches for young children with ASD. One relationship based approach isResponsive Teaching. This parent mediated intervention model developed by Dr.Gerald Mahoney is especially well suited to the Birth to Three service delivery modelwhich emphasizes a strong partnership between families and service providers (43) . <strong>The</strong>rehas been a great deal of interest recently in Relationship Development Interventiondeveloped and promoted by Dr. Steven Gutstein. This approach focuses on teachingpeople with ASD how to develop strong emotional relationships with others (44) . To date,research validating this approach is incomplete.One of the drawbacks of the relationship-based approach for children with autism is theopen ended quality of the instructional environment. Children who lack core skills suchas joint attention and imitation or who have severe challenging behaviors may be harderto engage in this model.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200823
Approaches used in the Birth to Three SystemOne or more of the previous approaches may be helpful in developing an individualizedprogram for a child with ASD in the Connecticut Birth to Three System. <strong>The</strong>seapproaches, in conjunction with the principles of intervention, should be consideredwhen developing an IFSP, depending on the individual needs of the child and family.All of the intervention techniques used in the Connecticut Birth to Three System arecarried out by licensed and certified staff as well as early intervention associates andassistants who meet the requirements of the Birth to Three Personnel Standards forConnecticut. Intervention for children with ASD requires that staff with expertise in theimplementation of the approach be a member of the intervention team. <strong>The</strong>seindividuals may come from a variety of professional backgrounds such as speechpathology, occupational therapy, early childhood education, special education orpsychology. <strong>The</strong>se staff members have the responsibility of working with the team in thedesign, training, and implementation of the program.ALTERNATIVE OR COMPLEMENTARY TREATMENTS<strong>The</strong>re is a great deal of information available today on treatment options for youngchildren with ASD. In addition to the standard forms of treatment previously noted in this<strong>Guideline</strong>, there are others that fall into a category of physiological and/or physicalinterventions. <strong>The</strong>se are often referred to as alternative treatments or complementarytreatments. <strong>The</strong>se interventions are viewed as an addition to the existing servicesprovided and supported by the Birth to Three System. Although the Birth to ThreeSystem neither provides these services, nor covers their cost, a service coordinator canassist a family in gathering necessary information on these treatment options.Some of the concerns service providers, as well as families, have expressed regardingthese treatments include:1. <strong>The</strong>re is a lack of scientific research and documentation on the effectiveness orpotential side effects (physical or emotional) that may result from the treatment;2. there are tendencies for some interventions to be either too narrow in focus or toclaim that the intervention will affect all areas of development;3. the financial impact on families who pursue treatments, is significant. Mosttreatments are not reimbursable by health insurance or, if they are, very little iscovered;4. there is a difficulty in finding qualified specialists to help implement and overseetreatment;5. the family may have unrealistic and false expectations about the outcome of theintervention.Families need to acquire as much information as possible before deciding to use thesetreatments. It is essential that these treatments be done under the guidance of qualifiedmedical specialists or therapists with experience in ASD. <strong>The</strong>se specialists may also behelpful in providing information on the effectiveness of the treatment based on otherpeople whom they treat. With any new treatment of intervention, a family should setspecific goals and objectives and should agree with the practitioner on a clear way of24CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
measuring success. If a treatment isn’t working it should be modified or discontinued, nomatter how convinced the practitioner is that it should work or he experience of others.Families need to keep in mind that participating in alternative treatments is verychallenging and they will often require ongoing support to implement the treatment aswell as data collection to measure effectiveness. In many cases, alternative treatmentsinvolve a change in a family’s lifestyle. <strong>The</strong>re are no “quick fixes” and thereforetreatments require ongoing supervision and adjustments as well as family commitment.Most importantly, in order to determine if a treatment is effective, it is essential toparticipate in one at a time. Intervention with multiple treatments will not allowassessment of which treatment was actually successful.To assist parents or caregivers as they evaluate different treatments, below is a list ofguidelines created by Dr. B.J. Freeman in her paper “Diagnosis of the Syndrome of<strong>Autism</strong>: Questions Parents Ask.”Principles of Evaluating the Treatment of <strong>Autism</strong>1. Approach any new treatment with hopeful skepticism. Remember that thegoal of any treatment should be to help the person become a fully functioningmember of society.2. Beware of any program or technique that is touted as effective or desirable forevery person with autism.3. Beware of any program that thwarts individualization and potentially results inharmful program decisions.4. Be aware that any treatment represents one of several options for a personwith autism.5. Be aware that treatment should always depend on individual assessmentinformation that points to it as an appropriate choice for a particular child.6. Be aware that no new treatment should be implemented until its proponentscan specify assessment procedures necessary to determine whether it will beappropriate for an individual with autism.7. Be aware that debate over use of various techniques are often reduced tosuperficial arguments over who is right, moral and ethical and who is a trueadvocate for the child. This can lead to results that are directly opposite tothose intended.8. Be aware that new treatments have often not been validated scientifically.Questions to Ask Regarding Specific Treatments:1. Will the treatment result in harm to the child?2. How will failure of the treatment affect the child and family?3. Has the treatment been validated scientifically?4. Are there assessment procedures specified?5. How will we know the treatment is working?6. How will the treatment be integrated into the child’s current program? Do notbecome so infatuated with a given treatment that functional curriculum, playand social skills are ignored. (45)An overview of some of the alternative or complementary treatment options and resources are included in AppendixSeven.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200825
FAMILY SUPPORTChildren with ASD present unique challenges to their families. No two families ofchildren with ASD will require the same support and often the need for support changesover time. Family support goals on the IFSP are often as important as childdevelopmental goals. Similarly, these goals should be evaluated over time and changedto reflect the needs of the child and family. Parents have shared that their need forsupport is quite significant during the time their child was first identified with an ASD.<strong>The</strong> IFSP should reflect a wide range of family support outcomes. <strong>The</strong>se might include:1. <strong>The</strong> need for information on ASD and intervention philosophies;2. Opportunities to speak with other parents of children with ASD;3. Support groups for parents of children with ASD;4. Training on how to teach the child new skills or strategies to integrate the child’sintervention into daily routines;5. Identifying appropriate childcare or respite support options;6. Professional counseling support;7. Support and information for siblings of children with ASD;8. Support and information for extended family members;9. Support for families to develop advocacy skills for their child with ASD.10. Support at the time of transition out of the Birth to Three System or othertransitions the family may experience.Appendix Eight contains a list of resource organizations for families.26CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
A FINAL NOTE FOR PARENTS BY PARENTSNothing during pregnancy prepares you for the news that your child has a disability. Fornine months all that expecting parents think about are names, preparing a nursery andplanning for the future. As parents receive the news of their child’s disability theyexperience all different emotions; from denial, depression, anger, and guilt , to finallyacceptance. All of these emotions are natural and healthy. <strong>The</strong>n the real work begins.Remember you are not alone- there are parents out there that want to help you. <strong>The</strong>ywant to offer advice, help you through the process of learning about the system, give youa shoulder to cry on and a push you in the right direction. Ask for help, and don’t beashamed. We all need help, and you should be ashamed if you are not asking. Beingan advocate for your child will help your child become successful through the years..This guideline and your Birth to Three Provider are there to help you. <strong>The</strong>y are there tosupport you, your family and your child. <strong>The</strong>y are the experts. If they do not have theanswer to your questions they will help you find them. Your journey has just begun, andyou do not have to travel alone.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200827
QUESTIONS COMMONLY ASKED THE BIRTH TO THREE SYSTEMBY PARENTS OF CHILDREN WITH ASD1. Q. My child has not had an evaluation for ASD. Will the Birth to Three System payfor an evaluation?A. <strong>The</strong> primary concern of the Birth to Three System is to determine whether yourchild meets the classification of autism under the IDEA. If your child has not hadan evaluation for ASD, this determination will typically be made by an <strong>Autism</strong>Specific program or your general Birth to Three program. Birth to Three will notpay for an outside medical diagnosis to determine if your child needs autismspecific services.2. Q. Our 17 month old had an autism screening as part of his initial Birth to Threeassessment and the Birth to Three program would like him to have further testingdone by an autism-specific program. We recognize that he has delays and isdifferent than other two-year-old children. But we think he is too young to bebrought to a specialist for a diagnosis. We would prefer to wait another year tosee how he develops. Is there any harm in waiting?A. It is important that a family makes the decision with which they are mostcomfortable for their child. What is most important is that you and your team arediscussing your child’s individual needs and developing a plan to address hischallenges. Further testing by an autism-specific program would occur in yourhome and would give a clearer picture of your child’s developmental needs butdoes not mean that you need to receive your Birth to Three services from anautism-specific program or receive more intensive services than you arecomfortable with. Should the evaluation by the autism-specific program indicatethat your child is on the autism spectrum, the research is very clear thatintervention should begin as early as possible to be most successful.3. Q. My child was diagnosed by an expert in the field who does not live inConnecticut. During the evaluation, he recommended we hire a consultant outsideof the Birth to Three System to consult with us on his program. Will the Birth toThree System pay for this?A. No, the Birth to Three programs in Connecticut are not obligated to hire anoutside consultant if the program has the available expertise to implement theIFSP. Parents are welcome to invite anyone they choose to participate in theIFSP meeting. As part of the development of the IFSP, appropriate staff andsupports are discussed and identified. It is the program’s decision as to whetherthey need a consultant and, if so, who that consultant will be.4. Q. Can early intervention cure ASD?A. No, there is no nationally accepted treatment that claims to cure ASD. Researchdoes indicate that with early and intensive intervention, many children makesubstantial gains and enter kindergarten in a regular education classroom withvarying levels of support.28CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
5. Q. Who is qualified to work with a young child with ASD?A. <strong>The</strong>re is no specific credential or discipline that qualifies an individual to workwith a child with ASD. We find that the complexity of behaviors and needs forchildren with ASD often require a team of individuals who work with the family.Team members could include any or all of the following: a special educator orearly childhood educator, an early intervention assistant or associate, aspeech/language pathologist, an occupational therapist, a psychologist or a socialworker. It is important that the members of the team have adequate training andexperience in working with children with ASD. While the system does not requireit, providers have Board Certified Behavior Analysts of other experienced staff aspart of their program to deal with all the components of the IFSP. If they do nothave staff experienced in a specific strategy or technique, then they may hire aconsultant of their choice to provide technical assistance and training to the staffand family.6. Q. Will the Birth to Three System provide a discrete trial instruction program for mychild?A. Yes. Discrete trial instruction is a technique used within a framework of appliedbehavioral analysis. Your Birth to Three provider will assist you with implementingdiscrete trial instruction if it is determined to be an effective technique based onyour child’s needs and is identified on the IFSP. This will typically be onecomponent of the IFSP that also includes opportunities for generalization of skillsto other settings and social interaction with others.7. Q. My child is not getting enough hours of service because we have a team meetingevery month. Is there any way to stop having team meetings so he can get moreservices?A. <strong>The</strong> exact pattern of service delivery is agreed upon by your family and yourservice coordinator is part of the IFSP process. <strong>The</strong> IFSP focuses on what isimportant to you as your child develops. Framing this conversation in terms of thehours Birth to Three staff are working with your child may stand in the way offiguring out the best ways Birth to Three and your family can work together to meetthe outcomes that are important to you. <strong>The</strong> point is not to receive hours ofservices but to make progress toward the outcomes you have identified. Yourfamily and Birth to Three need to strike a balance, using meeting time to makesure everybody is working together and still maintaining an intensity of servicesthat works well for your child and family.8. Q. Will the Birth to Three System pay for an alternative therapy such as auditorytraining, vision therapy or cranial sacral therapy for my child?A. No. <strong>The</strong> Birth to Three System will assist families with finding information andresources on alternative or complementary treatments. Often these treatmentsare considered medical intervention, which are not covered by our System. <strong>The</strong>System will not provide any treatment that has not been proven effective based onresearch studies.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200829
9. Q. What should I do if I am not satisfied with my child’s progress or program?A. If at all possible, you should be funneling your concerns about your child’sprograms through your service coordinator. This is the person who is mostfamiliar with you, your child, your IFSP, and the services that are being delivered.If you have done this, or feel that it is not a viable option, you should contact thedirector of the program who provides your services. In addition, you may contactthe Birth to Three Support Line (866-888-4188) or Child Development Infoline(800-505-7000) to express your concerns. <strong>The</strong>y can help you problem-solve withyour provider and will inform you of ways to file a formal complaint if you choose.<strong>The</strong> Birth to Three System also provides formal mediation of differences betweenfamilies and providers or the option of a hearing by an impartial hearing officer.Your rights to this process are explained in the Family Handbook: Guide IIOrientation to <strong>Service</strong>s as well as a brochure entitled “Parent Rights Under IDEAPart C.” You may ask your service coordinator for a copy of either of these at anytime.10. Q. What if I want services delivered by a program or particular provider that is notaffiliated with the Connecticut Birth to Three System?A. Your Birth to Three program is obligated to provide your child and family withappropriate, individually-designed services that address your child’s needs and willoffer developmental benefit. <strong>The</strong> program may choose to use its own staff or maychoose to use subcontractors to deliver those services. Who they use and howmuch they pay their subcontractors is their decision. If you have located asubcontractor that you would like them to use, you may suggest it. However, it isultimately the program’s decision.11. Q. What will happen to my child when he turns three years old and no longerreceives services from the Birth to Three System?A. All school districts in Connecticut are required to provide children with disabilitieswith an educational program to meet each child’s needs at the age of three. Inorder to ensure that children have services and supports in place on their thirdbirthday, planning and communication begins at least six months before the childturns three. <strong>The</strong> child will be referred to the local school district and a meeting willbe scheduled to review the child’s progress and any additional evaluationsnecessary to determine if the child is eligible for services from the school district.<strong>The</strong> Birth to Three System has a handbook and a video to assist families withplanning for the transition process. You can obtain these from your servicecoordinator. <strong>The</strong> fact that a Birth to Three evaluation determined that your childmet the classification of autism under the IDEA does not mean that the schooldistrict will automatically agree that your child has autism.30CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
APPENDICES – INDEXAppendix OneAppendix TwoAppendix ThreeAppendix FourAppendix FiveAppendix SixAppendix SevenAppendix EightAppendix NineAppendix TenMission of Connecticut Birth to Three SystemEarly Indicators for Screening for Autistic <strong>Spectrum</strong> <strong>Disorder</strong>sM-CHAT and BITSEA ChecklistsScreening and Assessment Tools for Autistic <strong>Spectrum</strong> <strong>Disorder</strong>sMedical Follow-up for Children Identified with ASDHow Parents Can Get the Most out of their Early Intervention VisitTypes of Alternative or Complementary Treatments for ASDOrganizationsReferencesResourcesCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200831
Appendix One32CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
<strong>The</strong> M-CHAT, <strong>The</strong> BITSEA & <strong>The</strong> CSBS-DPAppendix TwoM-CHAT Modified Checklist for <strong>Autism</strong> in ToddlersPlease fill out the following about how your child usually is. Please try to answer every question.If the behavior is rare (e.g., you’ve seen it once or twice), please answer as if the child does notdo it.1. Does your child enjoy being swung, bounced on your knee, etc.? Yes No2. Does your child take an interest in other children? Yes No3. Does your child like climbing on things, such as up stairs? Yes No4. Does your child enjoy playing peek-a-boo/hide-and-seek? Yes No5. Does your child ever pretend, for example to talk on the phone or take care Yes Noof dolls, or pretend other things?6. Does your child ever use his/her index finger to point, to ask for something? Yes No7. Does your child ever use his/her index finger to point, to indicate interest in Yes Nosomething?8. Can your child play properly with small toys (e.g., cars or bricks) without just Yes Nomouthing, fiddling, or dropping them?9. Does your child ever bring objects over to you (parent) to show youYes Nosomething?10. Does your child look you in the eye for more than a second or two? Yes No11. Does your child ever seem oversensitive to noise? (e.g., plugging ears) Yes No12. Does your child smile in response to your face or your smile? Yes No13. Does your child imitate you? (e.g., you make a face-will your child imitate Yes Noit?)14. Does your child respond to his/her name when you call? Yes No15. If you point at a toy across the room, does your child look at it? Yes No16. Does your child walk? Yes No17. Does your child look at things you are looking at? Yes No18. Does your child make unusual finger movements near his/her face? Yes No19. Does your child try to attract your attention to his/her own activity? Yes No20. Have you ever wondered if your child is deaf? Yes No21. Does your child understand what people say? Yes No22. Does your child sometimes stare at nothing or wander with no purpose? Yes No23. Does your child look at your face to check your reaction when faced withsomething unfamiliar?© 1999 Diane Robbins, Deborah Fein, & Marianne Barton<strong>The</strong> authors of the M-CHAT recommend conservative scoring rules in order to miss as few children on the autismspectrum as possible. Any child who fails three or more items on the entire M-CHAT, or two or more of the criticalitems should receive a comprehensive evaluation. <strong>The</strong> critical items are 2, 7, 9, 13, 14, and 15.YesNoCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 200833
34<strong>The</strong> Brief Infant-Toddler Social & Emotional Assessment (BITSEA)(Briggs-Gowan & Carter, 2002) ©Child’s birth date: ______/______/________ Today’s date: ______/______/________month day year month day yearSex of child: 1: Boy 2: Girl Your relationship to child: 1: Mother 2: Father 3: OtherChild’s ethnicity: 1: White/Caucasian 3: Hispanic/Latino 5: Native American/Eskimo2: Black/African American 4: Asian/Pacific Islander 6:Other:______________________Instructions: This questionnaire contains statements about 1- to 3-year-old children. Many statements describe normal feelings andbehaviors, but some describe things that can be problems. Some may seem too young or too old for your child. Please do your bestto answerevery question.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008© Protected underCopyright law. Usedhere with the permissionof the authors.For each statement, please circle the answer that best describes your child in the LAST MONTH. Circle 0 to indicate “Not True orRarely.” Circle 1 to indicate “Somewhat True or Sometimes.” Circle 2 to indicate “Very True or Often.”Please choose the answer that best describes your child in the LAST MONTH:0 = not true/rarely 1 = somewhat true/sometimes 2 = very true/often1. Shows pleasure when s/he succeeds25. Imitates playful sounds when you ask him/her to. 0 1 2(For example, claps for self). 0 1 226. Refuses to eat. 0 1 22. Gets hurt so often that you can’t take27. your eyes off him/her. 0 1 2Hits, shoves, kicks, or bites children (not includingbrother/sister). (N = No contact with other children) 0 1 2 N3. Seems nervous, tense or fearful. 0 1 228. Is destructive. Breaks or ruins things on purpose. 0 1 24. Is restless and can’t sit still. 0 1 229. Points to show you something far away. 0 1 25. Follows rules. 0 1 230. Hits, bites or kicks you (or other parent). 0 1 26. Wakes up at night and needs help to31.fall asleep again. 0 1 2Hugs or feeds dolls or stuffed animals. 0 1 27. Cries or tantrums until s/he is exhausted. 032.1 2Seems very unhappy, sad, depressed or withdrawn. 0 1 28. Is afraid of certain places, animals or things.33. Purposely tries to hurt you (or other parent). 0 1 2What is s/he afraid of?_______________ 0 134. 2 When upset, gets very still, freezes or doesn’t move. 0 1 2_________________________________<strong>The</strong> following questions are about feelings and behaviors that9. Has less fun than other children. 0 1 2 can be problems for young children. Some of the10. Looks for you (or other parent) when upset. 0 1 2questions may be a bit hard to understand, especially ifyou have not seen them in a child. Please do your best to11. Cries or hangs onto you when you try to leave. 0 1 2 answer them anyway.12. Worries a lot or is very serious. 0 135. 2 Puts things in a special order, over and over. 0 1 213. Looks right at you when you say his/her name. 0 136. 2 Repeats the same action or phrase, over and over. 0 1 2Describe: ___________________________14. Does not react when hurt. 0 1 237. Repeats a particular movement, over and over15. Is affectionate with loved ones. 0 1 2(like rocking, spinning, etc.). 0 1 216. Won’t touch some objects because of how they feel. 0 1 2 Describe: ___________________________17. Has trouble falling asleep or staying asleep. 0 138. 2 “Spaces out.” Is totally unaware of what’shappening around him/her. 0 1 218. Runs away in public places. 0 1 239. Does not make eye contact. 0 1 219. Plays well with other children (not includingbrother/sister). (N = No contact with other children) 0 140. 2 Avoids N physical contact. 0 1 220. Can pay attention for a long time. (Not including TV) 0 141. 2 Eats or drinks things that are not edible,like paper or paint. 0 1 221. Has trouble adjusting to changes. 0 1 2 Describe: ___________________________22. Tries to help when someone is hurt.42. Hurts him/herself on purpose.For example, gives a toy. 0 1 2 For example, bangs his or her head. 0 1 223. Often gets very upset. 0 1 2 Describe: ___________________________24. Gags or chokes on food. 0 1 2
<strong>The</strong> Brief Infant-Toddler Social & Emotional Assessment (BITSEA)(Briggs-Gowan & Carter, 2002) ©Scoring Instructions:1) Convert all “N” (no opportunity) responses to 0N responses are possible for the following two items:“Plays well with other children”“Hits, shoves, kicks or bites other children.”2) Problem domain:Sum the responses to the following questions: 2, 3, 4, 6, 7, 8, 9, 11, 12, 14, 16, 17, 18, 21, 23, 24,26, 27, 28, 30, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42If 6 or more problem questions are unanswered, we recommend that you do not use the problemsum.3) Competence domain:Sum the responses to the following questions: 1, 5, 10, 13, 15, 19, 20, 22, 25, 29, 31If 2 or more competence questions are unanswered, we recommend that you do not use thecompetence sum.Cutpoints:Problem scores that fall at or above the values listed below are considered high problems.Competence scores that fall at or below the values listed below are considered to indicate lowcompetence.Girls BoysBITSEA Scale:Cutpoint CutpointProblems12-17 months 13 1518-23 months 15 1524-29 months 13 1430-35 months 14 14Competence12-17 months 11 1118-23 months 15 1324-29 months 15 1430-35 months 15 14Combining a child’s status on the Problem and Competence cutpoints provides most sensitive detectionof problems and delays in competence. By combining cutpoints we mean that if a child has a highproblem score and/or a low competence score s/he would be considered to screen positive on theBITSEA.© Protected under Copyright law. Used here with the permission of the authors.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 35
Information on scoring this instrument may be found at www.firstwords.fsu.edu36CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Appendix ThreeScreening Tools for Autistic <strong>Spectrum</strong> <strong>Disorder</strong>s<strong>The</strong> Brief Infant-Toddler Social & Emotional Assessment (BITSEA) ©Birggs-Gowan, M. & Carter, A., 2002Communication and Symbolic Behavior Scales DP (CSBS) – (2002)Wetherby, A.M., & Prizant, B.Paul H Brookes Publishing, CO.First Signs – Public Awareness program for early identification for children withASD. Phone 978-346-4380 1-800-80-SIGNSEmail: nwiseman@firstsigns.orgPsycho-educational Profile – Revised (PEP-R) (1990)Schopler, E., Reichler, R., Bashford, A., Lansing, M. & Marcus, L.Austin, TX: Pro-Ed.<strong>The</strong> Checklist for <strong>Autism</strong> in Toddlers (CHAT) (1992)Baron-Cohen, S., Allen, J., & Gillberg, C.Can autism be detected at 18 months? <strong>The</strong> needle, the haystack and theCHAT. British Journal of Psychology, 161, 839-842.<strong>The</strong> Modified Checklist for <strong>Autism</strong> in Toddlers (M-CHAT) (1999)Robins, D., Fein, D., & Barton, M.University of Connecticut, Psychology Department, 860-486-3515Vineland Adaptive Behavior Scles (1984)Sparrow, S., Balla, D., & Cicchetti, D.Circle Pines, MN: American Guidance <strong>Service</strong>Appendix FourAssessment Instruments for <strong>Autism</strong> <strong>Spectrum</strong> <strong>Disorder</strong>s<strong>Autism</strong> Diagnostic Interview – Revised ADI-R (1994)Lord, C., Ritter, M,. & LeCourteur, A.Journal of <strong>Autism</strong> and Developmental <strong>Disorder</strong>s, 24, 659-685.<strong>Autism</strong> Diagnostic Observation Schedule ADOS (1999)Lord, C., Ritter, M., Di Lavorre, P., & Risi, S.Los Angeles, CA: Western Psychological <strong>Service</strong>s.Childhood <strong>Autism</strong> Rating Scale (CARS) (1988)Schopler, E., Reichler, R., & Renner, B. Los Angeles, CA: WesternPsychological <strong>Service</strong>sCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 37
• Referral to allergist if significant history of food allergies or eczema in child or very stronghistory of family history of allergic disorders• Referral to nutritionist to oversee “elimination” diet if food allergy is diagnosed.Although no medications have been demonstrated to “treat” autism, there is evidence that forsome older children and adults medications improve symptoms associated with autism includinganxiety, depression, and over stimulation. <strong>The</strong> most common medications used arepsychoactive medications. Psychoactive medications are those that primarily affect theperson’s behavior, mood, or thought processes. Many of the psychoactive medications thathave been used to treat other neurological or psychiatric conditions have also been tried forindividuals with autism.Diet therapies most commonly involve the elimination of milk or wheat products from the diet. Itis suggested that some young children with autism are allergic to milk and/or wheat and thateliminating these foods from the diet can result in an improvement in manifestations of autism.Most of the literature focuses on eliminating cow’s milk or casein and/or wheat products orgluten. If food allergies are documented, the child should be treated with standard allergytesting methods, including elimination diets. Since children with ASD often only eat a very smallnumber of foods, it is important to consult with a nutritionist before beginning any diet therapy,since one could be eliminating a child’s only source of important nutrients. A source of moreinformation can be found in Lisa Lewis’s 1998 book: Special Diets for Special Kids (1998),Arlington, TX: Future Horizons. 800-489-0727.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 39
Appendix SixHow Parents can get the most out of their early intervention visit(This information is also found in “A Family Handbook: Guide II Orientation to <strong>Service</strong>s”, p. 25,Connecticut Birth to Three System)Parents: You know your child best. You have valuable information about your child; Birth toThree staff need your input just as much as you need theirs. Remember, you are and will beyour child’s best, most important, and most constant teacher and advocate.Before Your Visit:• Be prepared. Make sure you schedule your visit when you can be there and nothave a lot of distractions. Decide how brothers and sisters will be involved or plan anactivity for them.• Plan the agenda. Let the Birth to Three staff know what you want to discuss at yourvisit. Remember or write down any questions that you may have since your last visit.• Be ready to share what has happened since your last visit. Think about or makea list of anything you think is important to share such as a trip to the doctor orchanges in routine. Think about what suggestions have worked well and those thathave not worked so well.During Your Visit:• Ask questions. Make sure you understand what is being said. If you are not surewhy something is being done, just ask. If it helps, ask for things in writing.• Ask for a demonstration. Ask to be shown anything you don’t understand. Practicestrategies together during the visit. Hands-on instruction is the best way to learn.• Discuss ideas for carry over between visits. Time between visits is just asimportant as the visit itself. Be sure to talk about ways to use the strategies andactivities during everyday family activities.After Your Visit:• Try things out. Try out the suggested activities. What is working? What isn’t?• Make a note of it. Remember to make a mental note or keep a notebook forquestions that may come up between visits.• Have fun. <strong>The</strong> best teaching and learning occurs when you and your child are havingfun.• Celebrate successes – even the tiny ones!!40CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Appendix SevenTypes of Alternative or Complementary Treatments for ASDThis is not an exhaustive list but it is intended to provide a brief overview of treatment optionsavailable. <strong>The</strong>se are not approaches that are recommended by the Birth to Three System.Some of these treatments are controversial and may not be generally accepted by the scientificand medical community. <strong>The</strong>y are provided as a resource for families who would like to acquiremore information on treatment. Involvement in any of these treatments should be discussedwith the family’s primary health care provider.1. Hormone <strong>The</strong>rapies: Several health problems in children and adults are associated withdeficiencies of particular hormones. Some hormone replacement therapies have beenproposed as possible treatments for autism. In particular, adrenocorticotropin hormone(ACTH) and secretin (a hormone that helps regulate digestion) have been suggested. <strong>The</strong>sehave not been found to be effective in scientific studies for young children and the potentialside effects from treatment with secretin are unknown.2. Immune <strong>The</strong>rapies: Immune therapies include treatment with intravenous immune globulinhas been suggested as a possible treatment for children with autism. Proponents of thesetherapies suggest that a subset of children with ASD have abnormalities in their immunesystems. <strong>The</strong> only treatment described in the scientific literature is intravenous immuneglobulin (IVIG) therapy.3. Anti Yeast <strong>The</strong>rapies: Anti yeast therapies have been proposed for children with autism.<strong>The</strong>se treatments involve administrations of oral anti-fungal medications or special diets thatinclude foods purported to have anti-fungal properties (such as garlic and grapefruit seedextract). <strong>The</strong> use of anti-fungal therapies is based on the theory that for some children thesymptoms of ASD are caused or aggravated by an overgrowth of yeast in the intestinal tract.This theory also suggests that yeast overgrowth occurs after children are treated withantibiotics.4. Vitamin <strong>The</strong>rapies: Administration of high doses of vitamins has been suggested as atreatment for young children with autism. High doses of Vitamin B6 (pyridoxine), magnesiumor trace minerals are most common. If a child has a documented vitamin or trace mineraldeficiency it should be treated. However, there is insufficient evidence to recommend it as atreatment for autism. Short-term side effects are reported to be mild, but side effects are notknown for young children treated with high doses or over long periods.5. Auditory Integration <strong>The</strong>rapy (AIT): This technique presumes that the child has a sensorydysfunction, most likely hypersensitivity to certain sounds, making a number of commonsounds painful to hear. <strong>The</strong> treatment involves a prescribed treatment program of listeningto sounds and music over a period of time with certain frequencies filtered out. <strong>The</strong> intent isto reduce the sound sensitivity and thereby improve behavior, social skills and cognitivefunctioning.6. Craniosacral <strong>The</strong>rapy: This technique involves physical manipulation of the body to freerestrictions of motion in the craniosacral system. <strong>The</strong> theory assumes that the restrictedmovement of cerebrospinal fluid is adversely affecting the development and function of theCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 41
ain. Dr. John Upledger believes that children who have ASD show symptoms of restrictedfluid movement through head banging, wrist biting, teeth grinding and hyperactivity.7. Vision <strong>The</strong>rapy: This technique is based on the assumption that some of the unusualbehaviors associated with ASD may be related to visual perception problems. Some of thedifficulty experienced by young children with ASD include poor eye contact, difficultyattending visually, staring or hyper or hypo sensitivity to light and/or color. Treatment mayinclude use of specialized color or prism glasses or vision exercises. It is considered anexperimental method for young children with ASD.8. Music <strong>The</strong>rapy: Music therapy involves using some aspect of music that may lead toimprovement in social interaction and language development in young children with ASD.<strong>The</strong> procedures for music therapy are highly variable.Resources on Alternative or Complementary TreatmentsLabels in parentheses ( ) indicate whether this is a resource for multiple treatments or a specifictreatment.Allergy-Induced <strong>Autism</strong>8 Hollie Lucas RoadKing’s Heath, BirminghamB130QL United Kingdomwww.autismmedical.com (Allergies)American Music <strong>The</strong>rapy Association8455 Colesville Road, Suite 1000Silver Spring, MD 20910301-589-3300www.musictherapy.org (Music <strong>The</strong>rapy)<strong>Autism</strong> Network for Dietary Intervention (ANDI)PO Box 17711Rochester, NY 14617-0711www.autismNDI.com (Diet)<strong>Autism</strong> Research Institute (ARI)4182 Adams AveSan Diego, Ca 92116866-366-3361http://www.autism.com/ari (Multiple)<strong>Autism</strong> Treatment Checklist (ATEC)Developed by the <strong>Autism</strong> Research Institute as an on line evaluation tool to help in evaluatingthe different approaches to treatment.www.healing-arts.org/children/ATEC.htm (Multiple)<strong>Autism</strong> Society of America7910 Woodmont Avenue, Suite 300Bethesda, MD 2081442CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
800-3<strong>Autism</strong>www.autism-society.org (Multiple)Center for Visual Management150 White Plains RoadTarrytown, NY 10591914-631-1070www.autisticvision.com (Vision)Gerlach, E. <strong>Autism</strong> Treatment Guide, Second Edition, (2000) Arlington, TX, Future Horizons,Inc. (Multiple)Heflin, L., Juane and Simpson, R.L. “Interventions for Children and Youths with <strong>Autism</strong>: PrudentChoices in a World of Exaggerated Claims and Empty Promises.” Part I: Intervention andTreatment Option Review, Focus on <strong>Autism</strong> and Other Developmental Disabilities, Volume 13,Number 4, Winter, 1998, 194-211. (Multiple)Hymen. S.L, & Levy, S.E. (2000). Autistic spectrum disorders: When traditional medicine is notenough – Contemporary Pediatrics, 17 (10): 101-116. (Medication)Lewis, Lisa. Special Diets for Special Kids (1998). Arlington, TX: Future Horizons. 800-489-0727. (Diet)New York State Department of Health (1999). Clinical Practice <strong>Guideline</strong>: <strong>The</strong> <strong>Guideline</strong>Technical Report. <strong>Autism</strong>/Pervasive Developmental <strong>Disorder</strong>s, Assessment and Intervention forYoung Children (Age 0-3). 518 439-7286.www.healthstatenyus/nysdoh/eip/indexhtm (Multiple)Nickel R, E. (1996). Controversial therapies for young children with developmental disabilities.Infants and Young Children, 8 (4): 29 – 40. (Multiple)<strong>The</strong> Padula Institute of Vision37 Soundview Road, Guildford, CT 06437Ph. 203-453-2222 website: www.padulainstitute.comRimland, G & Edelson, S. (1994) <strong>The</strong> effects of auditory integration training in autism. AmericanJournal of Speech-Language Pathology. 3, 16-24. (Auditory Integration)Society for Auditory Intervention Techniques (SAIT)PO Box 4538Salem, OR 97302www.berardaitwebsite.com/sait (Auditory Integration)<strong>The</strong> Upledger Institute11211 Prosperity Farm Road, Suite 325Palm Gardens, FL 33410800-233-5880http://upledger.com/ (Cranial Sacral Intervention)Zimmerman, A.W., Bonfardin, B., & Myers, S. (2000).Neuropharmocoloical therapy in autism. In P. Accardo, C. Magnusen & A. Capute (Eds.),<strong>Autism</strong> Clinical and Research Issues. Baltimore, York Press. (Medication)CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 43
Decision Makers Tool KitSouth Eastern Regional Education <strong>Service</strong> Center, Inc. (SERESC)29 Commerce DriveBedford, NH 03110-6835603-206-6800 (Multiple)44CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Appendix EightOrganizationsAtypical PDD/Asperger Syndrome Support Group34 Bullfrog LaneTrumbull, CT 06610203-261-7872<strong>The</strong> <strong>Autism</strong> Research Institute (ARI)4182 Adams AvenueSan Diego, CA 92116Voice 619-281-7165Fax 679-563-6840www.autism.com/ari<strong>Autism</strong> Society of America7910 Woodmont Avenue, Suite 650Bethesda, MD 20184-303151-800-3-autismwww.autism-society.org<strong>Autism</strong> Society of Connecticut (ASCONN)P. O. Box 1404Guilford, CT 06437(888) 453-4975<strong>Autism</strong> Society of North CarolinaBookstore Catalogue3300 Women’s Club DriveRaleigh, NC 07612-4811919-743-0204www.autismsociety-nc.orgConnecticut <strong>Autism</strong> <strong>Spectrum</strong> Resource Center (ASRC)101 North Plains Industrial Road Harvest Park, Bldg. AWallingford, CT 06492203-265-7717www.ct-asrc.orgCT FEAT – CT Families for Effective <strong>Autism</strong> TreatmentP.O. Box 370352, West Hartford, CT 06137-0352(860) 571-3888www.ctfeat.orgCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 45
ReferencesAppendix Nine1 Individuals with Disabilities Education Act, Amendments of 2004, 34 U.S.C.2 Committee on Educational Interventions for Children with <strong>Autism</strong> (2001).Educating Children with <strong>Autism</strong>. Washington, DC: National ResearchCouncil.3 Connecticut State Department of Education, Division of Teaching and LearningPrograms and <strong>Service</strong>s, Bureau of Special Education (2005):<strong>Guideline</strong>s for Identification and Education of Children and Youth With<strong>Autism</strong>4 Minnesota Early Intervention Project for Learners with <strong>Autism</strong> (1996) <strong>Autism</strong>and Related Pervasive Developmental <strong>Disorder</strong>s: Early Identificationand Intervention. Minnesota Department of Children, Families andLearning5 American Psychiatric Association. (2004). Diagnostic and Statistical Manual ofMental <strong>Disorder</strong>s, Fourth Edition, Text Revision). Washington, DC.6 <strong>Autism</strong> Society of America (January 1999). What is <strong>Autism</strong>? Bethesda, MD7 Briggs-Gowan, M.J. and Carter, A.S. (2001) BRIEF – Infant Toddler Social andEmotional Assessment Manual, Version 1.08 Robins, D., Fein, D., Barton, M. & Green, J. (1991) Modified Checklist for<strong>Autism</strong> in Toddlers (M-CHAT) J <strong>Autism</strong> Dev Disord 20019 Wetherby, A, & Prizant, B. (2002)Communication and Symbolic BehaviorScales Developmental Profile (CSBS DP)10 Plauch, Johnson Identification of Children with ASD Pediatrics Vol 120,Number 5 (November 2007) Baltimore, Paul Brookes11 Lord, C., Rutter, M., DiLavore, P., and Risi, S. (2000) <strong>Autism</strong> DiagnosticObservation Schedule (ADOS). Los Angeles, Western Psychological<strong>Service</strong>s12 Rutter, M., LeCouteur, A., & Lord, K. (2003) <strong>Autism</strong> Diagnostic Interview,Revised (ADI-R), Los Angeles, Western Psychological <strong>Service</strong>s13 Schopler, E. Reichler, R., and Rochen Renner B.(1988) Childhood <strong>Autism</strong>Rating Scale (CARS) J <strong>Autism</strong> Dev Disord 10 (1): 91–103.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 47
14 Myers, S., MD Management of Children with <strong>Autism</strong> <strong>Disorder</strong>s, Pediatrics Vol120, Number 5 (November 2007)15 Hurth, J., Shaw, E., Izeman, S., Whaley, K. & Rogers, S. (1999). Areas ofagreement about effective practices among programs serving youngchildren with autism spectrum disorders. Infants and Young Children. 12(2) 17-2616 Mahoney, G., Boyce, G., Fewell, R. R., Spiker, D., & Wheeden, C. A. (1998).<strong>The</strong> relationship of parent-child interaction to the effectiveness of earlyintervention services for at-risk children and children with disabilities.Topics in Early Childhood Special Education, 18, 5-17.17 Hume, K., Bellinei, S., Pratt, C. (2005). <strong>The</strong> Usage and Perceived Outcomesof Early Intervention and Early Childhood Programs for Young Childrenwith <strong>Autism</strong> <strong>Spectrum</strong> <strong>Disorder</strong>. Topics in Early Childhood SpecialEducation, 25, 195-207.18 Rapport, M. J., McWilliam, R. A., & Smith, B. J. (2004). Practices acrossdisciplines in early intervention: <strong>The</strong> research base. Infants & YoungChildren, 17(1), 32-44.19 Dunlap, G., and L. Fox (1999) “A Demonstration of Behavioral Support forYoung Children with <strong>Autism</strong>”. Journal of Positive Behavior InterventionsVol. 1, #2, Spring Pp 77-87.20 Ayers, J. (1989) Sensory Integration and the Child. Los Angeles, CA:Western Psychological <strong>Service</strong>s21 Frost, L.A. & Bondy, A.S. (1994). PECS: <strong>The</strong> Picture ExchangeCommunication System: Training Manual. Cherry Hill, NJ: PyramidEducational Consultants, Inc.22 Carbone, V., (2002) Teaching Verbal Behavior to Children with <strong>Autism</strong> andRelated Disabilities Unpublished Workshop Manual23 Quill, K.A. (2000). Do-Watch-Listen-Say. Baltimore, MD: Paul H. Brooks24 Jensen, V., and Sinclair, L. (2002). Treatment of autism in young children:Behavioral Intervention and Applied Behavior Analysis Infants andYoung Children, 14(4): Pp 42-52.25 Maurice, C., Green, G. & Luce, S. (Eds.) (1996). Behavioral Interventions forYoung Children with <strong>Autism</strong>, A Manual for Parents and Professionals.Austin, TX: Pro-Ed.26 Sundberg, M. & Partington, J. (1998) Teaching Language to children withautism and other developmental disabilities.27 Koegel, R., S. Camarata, L. Koegel, A Ben-Tall, and A. Smith (1998)Increasing speech intelligibility in children with autism. Journal of<strong>Autism</strong> and Developmental <strong>Disorder</strong>s 28:241-251.48CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
28 Fox, L.G., Dunlap, & D. Powell (2002). “Young children with challengingbehavior: Issues and considerations for behavior support.” Journal ofPositive Behavior Interventions 4: 208–17.29 McGee, G., M. Morrier, and T. Daly (1999). “An incidental teaching approachto early intervention for toddlers with autism”. Journal of the Associationfor Persons with Severe Handicaps 24:133-146.30 Wetherby, A.M., A. Schuler, and B. Prizant (1997). “Enhancing language andcommunication: <strong>The</strong>oretical foundations.” Pp. 513-538 in Handbook of<strong>Autism</strong> and Pervasive Developmental <strong>Disorder</strong>s, 2 nd Edition, D. Cohenand F Volkmar, eds. New York: John Wiley and Sons.31 Lewy, A.L., and G. Dawson (1992) “Social stimulation and joint attention inyoung autistic children.” Journal of Abnormal Child Psychology20(6):555-566.32 Hwang, B., and C. Hughes (2000). Increasing early social-communicativeskills of preverbal children with autism through social interactivetraining. Journal of the Association for Persons with Severe Handicaps25:18-28.33 Rogers, S.J., and D. DiLalla (1991) A comparative study of a developmentallybased preschool curriculum on young children with autism and youngchildren with other disorders of behavior and development. Topics inEarly Childhood Special Education 11:29-48.34 Rogers, S.J., and H. Lewis (1989). An effective day treatment model foryoung children with pervasive developmental disorders. Journal of theAmerican Academy of Child and Adolescent Psychiatry 28:207-214.35 Greenspan, S., & Weider, S. (1997). Developmental patterns and outcomes ininfants and children with disorders in relating and communicating: Achart review of 200 cases of children with autistic spectrum diagnoses.Journal of Developmental and Learning <strong>Disorder</strong>s 1:87-141.36 Greenspan, S., & Weider, S. (1998). <strong>The</strong> Child With Special Needs. Redding,MA. Addison-Wesley.37 Schopler, E., Mesibov,G. B., Hearsey, K.A. (1995) Structured teaching in theTEACCH system. Pp 243-268 in Learning and Cognition in <strong>Autism</strong>, E.Schopler and G.B. Mesibov eds, New York, Plenum Press38 Prizant, B., Wetherby, A., Rubin, E. Rydell, P., Laurent, A. Quinn, J. (2003) <strong>The</strong>SCERTS TM Model [Special Issue] Jension <strong>Autism</strong> Journal (14:4).CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 49
39 Prizant, B. & Wetherby, A. (1998). Understanding the Continuum of DiscretetrialTraditional to Social-Pragmatic Developmental Approaches toCommunication Enhancement for Young Children with <strong>Autism</strong>, PDD.Seminars in Speech and Language. 19: 329-353.40 Rogers, S.J., Herbison, H. Lewis, J. Pantone, and K. Reis (1986) Anapproach for enhancing the sumbolic, communicative, andinterpersonal functioning of young children with autism and severeemotional handicaps. Journal of the Division of Early Childhood,10:135-148.41 Rogers, S.J., and Lewis, H. An effective day treatment model for youngchildren with pervasive developmental disorders. Journal of theAmerican Academy of Child and adolescent Psychiatry 28:207-214.42 Anderson, S.R., and R.G. Romanczyk (1999). “Early intervention for youngchildren with autism: Continuum-based behavioral models”. Journal ofthe Association for People with Special Handicaps 24(3):162-173.43 Mahoney, G. & MacDonald, J. (2007) <strong>Autism</strong> and Developmental Delays inYoung Children: <strong>The</strong> Responsive Teaching Curriculum for Parents andProfessionals. Austin, PRO-ED44 Gutstein, S., Sheely, R. (2002) Relationship Development Intervention withYoung Children. London, Jessica Kingsley Publishers45 Freeman,B.J. (1993) Diagnosis of the syndrome of autism: Questions parentsask. <strong>Autism</strong> Society of America50CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Appendix TenResourcesAyers, J. (1989). Sensory Integration and the Child. Los Angeles, CA: Western Psych <strong>Service</strong>s.Bambara, L.M., Brown, F. editors (1999) “Special Series on Intervention for Young Children with<strong>Autism</strong>” <strong>The</strong> Journal of <strong>The</strong> Association for Persons with Severe Handicaps, Volume 24,Number 3.Baron-Cohen, S. Allen, J., & Gillberg, C. (1992). Can autism be detected at 18 months? theneedle, the haystack and the CHAT. British Journal of Psychiatry. 168:158-63.Berkson, G. & Tupa, M. (2000). “Early Development of stereotyped and self injurious behaviors”.Journal of Early Intervention. Vol. 23, No 1. 1-19.Blackman, J.A., Neisworth, J.T. Bagnato, S., (Eds) (1999). “Special Issue on <strong>Autism</strong>”.Infants & Young Children. 12, #2.Bricker, Diane et al. (1998) An Activity Based Approach to Early Intervention, SecondBaltimore, MD, Paul Brookes, Inc.Edition.Durand, M. (1998). Sleep Better! A Guide to Improving Sleep for Children with Special Needs.Baltimore, MD, Paul Brookes, Inc.Filipek, P., Prizant, B.M. et al., (2000). “Practice parameter: screening and diagnosis of autism”.Neurology. 55 548-479.Fox, L. Dunlop, G., Buschbacker, P., & Valente, L.A. (1998). Individualized Support Project –Replication Manual. University of South Florida; <strong>The</strong> Louise de la Park Florida MentalHealth Institute.Freeman, B.J. (1997). “<strong>Guideline</strong>s for evaluating intevention programs for children with autism”.Journal of <strong>Autism</strong> and Developmental <strong>Disorder</strong>s, 27(6), 641-651Frost, L.A. & Bondy, A.S. (1994). PECS: <strong>The</strong> Picture Exchange Communication System:Training Manual. Cherry Hill, NJ: Pyramid Educational Consultants, Inc.Gerlach, E. (2000). <strong>Autism</strong> Treatment Guide. Arlington, TX: Future Horizons Press.Gill, Barbara (1997) Changed by a Child: Companion Notes for Parents of a Child with aDisability. New York: Doubleday.CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 51
Greenspan, S.I. (1992). “Reconsidering the diagnosis and treatment of very young childrenwith autistic spectrum or pervasive developmental disorder”.Zero to Three. Volume 13 (Number 2).Greenspan, S. & Weider, S., (1998). <strong>The</strong> Child with Special Needs. Reading, MA: AddisonWesley.Harris, S.L. (1994). Siblings Of Children With <strong>Autism</strong>. New York, NY: Pocket BooksHarris, S.L. & Handleman, J.S. (1994). Preschool Education Programs For Children With<strong>Autism</strong>. Austin, TX: Pro-EdHarris, S., Weiss M. (1998). Right from the Start: Behavioral Intervention for yound childrenwith <strong>Autism</strong>. Bethesda, M.D.: Woodbine House. www.woodbinehouse.com or 800-843-7323Hart, C. (1993). A Parents Guide To <strong>Autism</strong>: Answers To <strong>The</strong> Most Common Questions. NewYork, N.Y. Pocket Books.Hodgdon, L. (1999). Visual Strategies for Improving Communications – Practical Supports forHome and School. Troy, MI: Quirk Roberts Publishing.Hurth, J., Shaw, E., Izeman, S., Whaley, K. & Rogers, S. (1999). “Areas of agreement abouteffective practices among program serving young children with autism spectrumdisorders”. Infants and Young Children. 12 (2): 17-26.Hyman, S. & Levy, S. (2000). “Autistic spectrum disorders. When traditional medicine is notenough”. Contemporary Pediatrics. October, Vol. 17 No 10 101-116.Interdisciplinary Council on Developmental and Learning <strong>Disorder</strong>s (2000).Clinical Practice <strong>Guideline</strong>s. Bethesda, MD. IDCS Press, www.kdl.comIzeman, S. (1995). “Embedding teaching for young children with autism into daily activities”.Early Intervention. Vol. 6, Number 2, Pages 1-3.Leaf, R., & McEachin, J. (Eds.) (2000). A Work In Progress- Behavioral Management Strategiesand a Curriculum for Intensive Behavioral Treatment of <strong>Autism</strong> Different Roads toLearning. New York, NY: DRL BooksLehman, J. & Klaw, R. (2001). From Goals to Data and Back Again: Adding Backbone toDevelopmental Intervention for Children with <strong>Autism</strong>. Pittsburg, PA: Kid Access, Inc.Lewis, L. (1998). Special Diets for Special Kids. Arlington, TX: Future Horizons, Press.Lovaas, I.O. (1981). Teaching Developmentally Disabled Children: <strong>The</strong> ME Book. <strong>Autism</strong>, TX.Pro-Ed.McClannahan, L., & Kratz, P., (1999). Activity Schedules for Children with <strong>Autism</strong> – TeachingIndependent Behavior. Bethesda, MD, Woodbine House.52CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
McGee, G., Morrier, M., & Daly, T. (1999). An incidental teaching approach to early intervention.Journal of the Association for Severe Handicaps, 24, 133-146.Maurice, C., Green & Luce, S. (Eds.) (1996). Behavioral Interventions for Young Children with<strong>Autism</strong>, A Manual for Parents and Professionals. Austin, TX,Pro-Ed.Mirenda, P., and Santogrossi, J. (1985). A prompt-free strategy to teach pitorial communicaitonsystem use. Augmentative and Alternative Communicaiton, 1, 143-150.Nickel, R. (1996). “Controversial therapies for young children with developmental disabilities”.Infants and Young Children. 8(4) 29-40.National Research Council (2001). Educating Children with <strong>Autism</strong>. Washington DC. NationalAcademy Press. www.nap.eduNew York State Department of Health (1999). Clinical Practice <strong>Guideline</strong>: <strong>The</strong> <strong>Guideline</strong>Technical Report. <strong>Autism</strong>/Pervasive Developmental <strong>Disorder</strong>s, Assessment andIntervention for Young Children (Age 0-3.)(518) 439-7286.Powers, M.D. (Ed.) (2000). Children with <strong>Autism</strong>: A Parents Guide. New York: Woodbine House.Prizant, B., & Wetherby, A. (1998). Understanding the continuum of discrete-trial traditionalbehavioral to social –pragmatic developmental approaches in communicationenhancement for young children with <strong>Autism</strong>/PDD.Seminars in Speech and Language. 19, 329-353.Prizant, B.M., Wetherby, A.M. & Rydell, P. (2000). Children with <strong>Autism</strong> <strong>Spectrum</strong> <strong>Disorder</strong>s: ADevelopmental Transactional Perspective. Baltimore, MD: Paul Brookes Publishing Co.Quill, K. (Ed.) (1995). Teaching children with autism: Strategies to enhance communication andsocialization. Albany, NY: Delmar Publishers. 800-347-7707Quill, K.A., (2000). Do-Watch-Listen-Say: Social Communication Intervention for Children with<strong>Autism</strong>. Baltimore, MD. Paul Brooks.Satkiewicz-Gayhardt, V., Peerenboom, B., Campbell, R., (1998). Crossing Bridges: A ParentsPerspective on Coping After a Child is Diagnosed with <strong>Autism</strong>/PDD. Stratham, NH:Potential Unlimited Publishing. 603-778-6006.Schuler, A., & Wolfberg, P. Promoting peer play and socialization: <strong>The</strong> art of scaffolding. In A.Wetherby & B. Prizant. (Eds.) Autistic <strong>Spectrum</strong> <strong>Disorder</strong>s (pp. 251 – 278) Baltimore:Paul H. Brookes.Southeastern Regional Education <strong>Service</strong> Center, Inc., (2001). Decision Maker’s Tool Kit – ForThose Who Live and Work With Young Children With Autsim/Pervasive Developmental<strong>Disorder</strong>s. Perry, NH: SERESC. Cwoodman@seresc.netCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 53
Sperry, L., Whaley, K., Stacy E., & Brame, K., (1999). <strong>Service</strong>s for young children with autismspectrum disorders: voices of parents and providers. Infants and Young Children. 11(4),17-33.Stock-Kranowitz, Carol (1998) <strong>The</strong> Out of Sync Child. New York, NY: Penguin PutnamPublishing.Sussman, F., (1999). More Than Words:Helping Parents Promote Communication Skills inChildren with <strong>Autism</strong> <strong>Spectrum</strong> <strong>Disorder</strong>. Toronto, Canada, Beacon Press.Trott, M., Laurel M. K. & Windeck, S.L., (1993). Sensibilities: Understanding SensoryIntegration. Tuscon, AZ: <strong>The</strong>rapy Skill Builders.Wetherby, A. & Prizant, B. (May 2000) <strong>Autism</strong> spectrum disorders: A transactionaldevelopmental perspective. Baltimore, MD: Brookes Publishing Co. 800-638-3775Whaley, K & Shaw, E., (Eds.) (1999). NECTAS Resource Collection on <strong>Autism</strong> <strong>Spectrum</strong><strong>Disorder</strong>s. Chapel Hill, NC NECTAS. www.nectas.unc.eduWheeler, M., (1998) Toilet Training for Individuals with <strong>Autism</strong> and Related <strong>Disorder</strong>s. Arlington,TX: Future Horizons Press.Books Written by Parents and Individuals with <strong>Autism</strong>Barron, J & Barron, S. (1992). <strong>The</strong>re’s a Boy in Here. New York: Simon and SchusterGrandin, T. (1986). Emergence: Labeled Autistic. Norvato, CA: Arena PressKephart, B. (1999). A Slant of Sun One Child’s Courage New York: W.W. NortonMaurice, C. (1993). Let Me Hear Your Voice. New York: Alfred A. Knopf, Inc.Park, C.C. (1993). <strong>The</strong> Seige: <strong>The</strong> First Eight Years with an Autistic Child. Boston, MA: LittleBrown.Schulze, C.B., (1993). When Snow Turns to Rain: One Family’s Struggle to Solve the Riddle of<strong>Autism</strong>. Rockville, MD: Woodbine.Stehl, A., (1991). <strong>The</strong> Sound Of A Miracle: A Child’s Triumph Over <strong>Autism</strong>. New York: AvonBooks.Stehl, A., (1995). Dancing in the Rain: Stories of Exceptional Progress by Parents of Childrenwith Special Needs. Westport, CT: Georgiana Org., Inc.Williams, D., (1992). Nobody Nowhere: <strong>The</strong> Extraordinary Autobiography Of An Autistic. NewYork: New York Times Books.Williams, D., (1994). Somebody’s Somewhere: Breaking Free From the Wold of <strong>Autism</strong>. NewYork: New York Times Books.54CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008
Books For KidsAmenta, C.A., (1992). Russell is Extra Special A Book About <strong>Autism</strong> For Children. New York,NY: Magination Press.Brown, T., (1984). Someone Special Just Like You. New York, NY: Holt & Co.Katz, I. & Rituo, E. (1993). Joey and Sam. Northridge, CA: Real Life Story Books.Lears, Laurie, (1998). Ian’s Walk, A Story about <strong>Autism</strong>. North Carolina Bookstore.Martin, Ann (1990). <strong>The</strong> Baby Sitter Club: Kristy and the Secret of Susan. New York Scholastic,Inc.Messner, A.B., (1996) Captain Tommy. Stratham, NH: Potential Unlimited Publishing. (603) 778-6006Single Sheet Designed for Kidswww.autism-society.orgBrochure: <strong>Autism</strong> Information Written for Kids OnlyAvailable from: <strong>Autism</strong> Society of America7910 Woodmart Avenue, Suite 650Bethesda, MD 208114-30151-800-3-AUTISMwww.autism-society.orgCT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008 55
VideosDoctor, My Child Doesn’t Talk<strong>The</strong> Importance of Early <strong>Autism</strong> Diagnoses (1997)FEATPO Box 255722Sacramento, CA 95865Discrete Trial Teaching (1999)Family Education Series NY Families for Autistic Children, Inc.718-641-6711An Introduction to PECS:<strong>The</strong> Picture Exchange System (1998)Pyramid Ed Consultants, Inc.226 W. Park Place, Suite 226Newark, DE, 1974<strong>Autism</strong>: Being Friends (a video for children)Indiana Resource Center for <strong>Autism</strong>3853 East 10 th StreetBloomington, IN 47408812-855-6508www.iidc.indiana.edu (publications catalog screen)56CT Birth to Three System • <strong>Service</strong> <strong>Guideline</strong> #1 • Revised July, 2002 and January, 2008