do irritable bowel syndrome symptoms vary between men and ...
do irritable bowel syndrome symptoms vary between men and ...
do irritable bowel syndrome symptoms vary between men and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Ali<strong>men</strong>tary Pharmacology <strong>and</strong> TherapeuticsMeta-analysis: <strong>do</strong> <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> <strong>symptoms</strong> <strong>vary</strong><strong>between</strong> <strong>men</strong> <strong>and</strong> wo<strong>men</strong>?M. A. Adeyemo*, B. M. R. Spiegel & L. Chang**Center for Neurobiology of Stress,Los Angeles, CA 90095, USA.VA Greater Los Angeles HealthcareSystem; Division of Digestive Diseases,David Geffen School of Medicineat UCLA; <strong>and</strong> UCLA ⁄VA Centerfor Outcomes Research <strong>and</strong> Education(CORE), Los Angeles, CA 90073,USA.Correspondence to:Dr L. Chang, Center for the Neurobiologyof Stress, CHS 47-122, 10833 LeConte Avenue, Los Angeles, CA90095, USA.E-mail: linchang@ucla.eduPublication dataSubmitted 16 February 2010First decision 5 March 2010Resubmitted 23 June 2010Accepted 23 June 2010SUMMARYBackgroundStudies suggest that sex <strong>and</strong> gender-related differences exist in <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> (IBS), but data is often conflicting.AimTo evaluate gender differences <strong>and</strong> the effect of <strong>men</strong>strual cycle <strong>and</strong> <strong>men</strong>opausalstatus on IBS <strong>symptoms</strong>.MethodsWe performed a systematic review of MEDLINE to search for studiescomparing IBS <strong>symptoms</strong> <strong>between</strong> gender, <strong>men</strong>strual cycle phases <strong>and</strong><strong>men</strong>opausal states in IBS <strong>and</strong> ⁄ or healthy individuals. We performed metaanalysesto compare the relative risk (RR) of individual IBS <strong>symptoms</strong><strong>between</strong> <strong>men</strong> <strong>and</strong> wo<strong>men</strong>.ResultsTwenty-two studies measured gender differences in IBS <strong>symptoms</strong>. Wo<strong>men</strong>were more likely to report ab<strong>do</strong>minal pain (RR = 1.12, 95% CI: 1.02, 1.22)<strong>and</strong> constipation-related <strong>symptoms</strong> (RR = 1.12, 95% CI: 1.02, 1.23) than<strong>men</strong> (all P < 0.05). However, <strong>men</strong> with IBS were more likely to reportdiarrhoea-related <strong>symptoms</strong> than wo<strong>men</strong> with IBS (RR = 0.84, 95% CI:0.75, 0.94, P < 0.05). A systematic review of 13 studies demonstrated thatboth IBS <strong>and</strong> healthy wo<strong>men</strong> reported increased IBS <strong>symptoms</strong> during<strong>men</strong>ses vs. other phases. There were insufficient data to determine the effectof <strong>men</strong>opause <strong>and</strong> hormone supple<strong>men</strong>tation on IBS <strong>symptoms</strong>.ConclusionsIn the general <strong>and</strong> IBS populations, gender differences in IBS <strong>symptoms</strong>exist, although these differences are modest. Studies suggest that female sexhormones influence the severity of IBS <strong>symptoms</strong>, but more studies areneeded.Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd 1<strong>do</strong>i:10.1111/j.1365-2036.2010.04409.x
M. A. Adeyemo et al.INTRODUCTIONIrritable <strong>bowel</strong> <strong>syndrome</strong> (IBS) is characterized by recurrentab<strong>do</strong>minal pain or discomfort associated with achange in <strong>bowel</strong> habits. 1 The prevalence of IBS rangesfrom 6% to 22% in Western countries, although theprevalence in Eastern countries tends to be lower <strong>and</strong>ranges from 2% to 17%. 2 IBS has a female pre<strong>do</strong>minancewith a female-to-male ratio of 2–2.5:1 in those who seekhealth care. The female pre<strong>do</strong>minance is less apparent inthe general population, which suggests that wo<strong>men</strong> withIBS are more likely to seek healthcare for their <strong>symptoms</strong>.3–7 However, some Asian studies fail to report significantgender differences in the prevalence of IBS,suggesting that cultural differences may also play a rolein IBS symptom reporting. 8, 9Gender differences in IBS are evident by subclassification,nongastrointestinal (GI) <strong>symptoms</strong>, pathophysiologicalresponses <strong>and</strong> treat<strong>men</strong>t response. 10 Specifically,female pre<strong>do</strong>minance is particularly apparent in the IBSwith constipation (IBS-C) subtype compared with IBSwith diarrhoea (IBS-D) <strong>and</strong> alternating or mixed pattern(IBS-M). 11 Although gender differences in pathophysiologicalstudies (e.g. GI transit, rectal perception, brainactivation patterns) have been reported in IBS <strong>and</strong>healthy controls, 12, 13 there are also conflicting reportsthat failed to identify differences <strong>between</strong> <strong>men</strong> <strong>and</strong>wo<strong>men</strong>. 14 Response to some IBS treat<strong>men</strong>ts, such asserotonergic agents, appears to be more robust in wo<strong>men</strong>than in <strong>men</strong>. 12, 15–17 However, these findings may be dueto an inadequate number of <strong>men</strong> in IBS studies ratherthan a true gender difference in nonstudy populations.In fact, there have been inadequate efforts to enrollsufficient numbers of <strong>men</strong> in many IBS studies <strong>and</strong> inadequateattempts to control for <strong>men</strong>strual cycle phaseamong wo<strong>men</strong> in these trials. 10 In addition, genderdifferences <strong>and</strong> the effect of female sex hormones havelargely been understudied in IBS. A recent review suggestedthat a strong relationship <strong>between</strong> <strong>men</strong>strual cycle<strong>and</strong> <strong>bowel</strong> <strong>symptoms</strong> exists <strong>and</strong> that this may be due toeffects of ovarian hormones on visceral pain sensitivity<strong>and</strong> <strong>bowel</strong> function. 18It is important to determine whether there are truesymptom differences <strong>between</strong> genders in IBS because thisinformation can potentially impact our underst<strong>and</strong>ing ofthe pathophysiology of IBS <strong>and</strong> influence research studydesign, drug develop<strong>men</strong>t <strong>and</strong> treat<strong>men</strong>t. Two previousreviews assessed gender differences in the diagnosis ofIBS. One review was conducted in developing countries,19 whereas the other was a systematic review ofstudies conducted in community populations. 2 Bothreviews concluded that most Western studies supporteda female pre<strong>do</strong>minance of IBS. However, approximatelyhalf of the studies conducted in Eastern countriesreported a female pre<strong>do</strong>minance while the other half didnot. Irrespective of whether the studies were conductedin Western or Eastern populations, the female-to-maleratio was dependent on the diagnostic criteria, i.e. agreater female pre<strong>do</strong>minance was seen when Manningcriteria were used vs. Rome criteria. 2To underst<strong>and</strong> better the gender differences in IBS,we performed a systematic review <strong>and</strong> meta-analysis ofthe literature to evaluate gender differences in individualIBS <strong>symptoms</strong> <strong>and</strong> the role of <strong>men</strong>strual cycle, <strong>men</strong>opausalstatus <strong>and</strong> hormone supple<strong>men</strong>tation on these<strong>symptoms</strong>. We hypothesized that the pooled data wouldreveal that wo<strong>men</strong> more frequently report ab<strong>do</strong>minalpain <strong>and</strong> nonpain related <strong>symptoms</strong> associated with constipationsuch as hard stools, bloating, ab<strong>do</strong>minal distension<strong>and</strong> straining than <strong>men</strong>, <strong>and</strong> that <strong>men</strong> more oftenreport <strong>symptoms</strong> associated with diarrhoea such as loosestools <strong>and</strong> increased stool frequency. In addition, wehypothesized that the pooled data would reveal a higherprevalence of IBS <strong>symptoms</strong> at times when ovarian hormonesare low, i.e. at the onset of <strong>men</strong>ses in pre<strong>men</strong>opausalwo<strong>men</strong> <strong>and</strong> during <strong>men</strong>opause, <strong>and</strong> that these<strong>symptoms</strong> decrease with hormone supple<strong>men</strong>tation.METHODSSearch strategyThe analysis for this study was based on a broadersearch for articles pertaining to dyspepsia <strong>and</strong> ⁄ or IBS.We conducted a comprehensive search for English languagestudies in MEDLINE published up to June 2010,which examined gender differences in IBS <strong>and</strong> ⁄ or theeffect of <strong>men</strong>strual cycle, <strong>men</strong>opausal status or hormonesupple<strong>men</strong>t on GI <strong>symptoms</strong>. The keywords <strong>and</strong> searchstrings used to perform the search with Reference ManagerSoftware are indicated in Table 1. In addition, weperformed manual searches of reference lists from relevantpapers to identify other manuscripts, which mayhave been missed by the search strategy.Screening strategyWe excluded titles if they did not meet the followinginclusion criteria: (i) written in English; (ii) investigationof humans; (iii) examination of IBS or functional dyspepsia<strong>symptoms</strong>; (iv) assess<strong>men</strong>t of IBS or functional2 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.Table 3 | Relative risk of IBS <strong>symptoms</strong> in wo<strong>men</strong> vs. <strong>men</strong> in both the general <strong>and</strong> IBS patient populationsGeneral population IBS onlyRR favouring wo<strong>men</strong>(95% CI)No.studiesHeterogeneity(P)RR favouring wo<strong>men</strong>(95% CI)No.studiesHeterogeneity(P)IBS diagnostic <strong>symptoms</strong>Pain 1.12 (1.02, 1.22)* 5
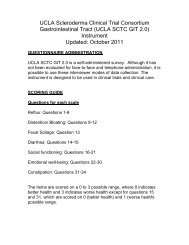
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>Ab<strong>do</strong>minal painStudyRisk ratio % WeightStudy(95% CI)Zuckerman 31 1.01 (0.94, 1.09) 20.41.09 (1.00, 1.20) 19.3Talley 28Talley 281.08 (1.02, 1.14) 21.9Talley 27Talley 271.08 (1.02, 1.15) 21.6 Taub 29Taub 291.40 (1.24, 1.58) 16.8 Zuckerman 31Ab<strong>do</strong>minal pain associatedwith a change in stool formRisk ratio(95% CI)% Weight1.23 (1.14, 1.33) 24.41.10 (1.03, 1.17) 25.91.19 (1.11, 1.27) 25.60.98 (0.91, 1.06) 24.1S<strong>and</strong>ler 52 S<strong>and</strong>ler 52Overall (95% CI)1.12 (1.02, 1.22)0.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong>Overall (95% CI)1.12 (1.02, 1.23)0.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong>BloatingStudyRisk ratio(95% CI)% WeightStudyShen 58Talley 27Talley 281.21 (1.06, 1.39) 14.41.00 (0.95, 1.05) 18.01.00 (0.89, 1.13) 15.1Schmulson 59Shen 58Talley 27TalleyTan 531.44 (1.33, 1.57) 17.028Tan 53Taub 291.11 (1.06, 1.16) 18.1 Taub 29Zuckerman 31 1.02 (0.95, 1.09) 17.4 Tujeta 30Zuckerman 31Overall (95% CI)1.12 (1.01, 1.25)Overall (95% CI)StrainingRisk ratio % Weight(95% CI)1.10 (1.04, 1.16) 12.31.47 (1.08, 2.01) 4.91.04 (1.00, 1.09) 12.61.07 (0.95, 1.20) 10.61.09 (1.02, 1.17) 12.11.11 (1.02, 1.21) 11.51.43 (1.35, 1.52) 12.31.09 (1.01, 1.17) 11.90.97 (0.89, 1.05) 11.71.12 (1.03, 1.23)0.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong>0.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong>Figure 2 | Forest plots of the risk ratios <strong>and</strong> 95% confidence intervals for gender differences in general populationstudies evaluating ab<strong>do</strong>minal pain, bloating <strong>and</strong> straining are shown.Assess<strong>men</strong>t for publication bias. Only two symptomcomparisons surveyed in the general population showeda potential publication bias. Funnel plots suggest a lackof small, positive studies for ab<strong>do</strong>minal pain associatedwith change in stool frequency <strong>and</strong> a lack of small, negativestudies for frequent stools.Menstrual cycle effect on IBS <strong>symptoms</strong>Table 4 provides general information on the 13 studiesthat assessed the effect of <strong>men</strong>strual cycle on IBS <strong>symptoms</strong>.32, 37–45, 62, 63 Study metho<strong>do</strong>logy varied withregard to study design <strong>and</strong> determination of <strong>men</strong>strualcycle phase with seven studies of good quality <strong>and</strong> six ofintermediate quality. Six studies assessed <strong>symptoms</strong> prospectivelyusing daily diaries, two surveyed currentsymptom severity score <strong>and</strong> the remaining studies usedsymptom recall. Only two studies used ovulation kits to<strong>do</strong>cu<strong>men</strong>t <strong>men</strong>strual cycle phase.All but three studies stated that wo<strong>men</strong> (average 40–60%) reported increased GI <strong>symptoms</strong> at time of <strong>men</strong>sescompared with other phases. 32, 37–42, 44, 45, 62 The <strong>symptoms</strong>for which most studies showed a significant <strong>men</strong>strualcycle effect were (in descending order) loose stools, bloating,ab<strong>do</strong>minal pain, stool frequency <strong>and</strong> other changes in<strong>bowel</strong> habit (Figure 4, Table 4). In general, increased diarrhoeawas reported at the time of <strong>men</strong>ses by more wo<strong>men</strong>than increased constipation. Although <strong>men</strong>strual cycleeffects on <strong>symptoms</strong> were similar in healthy wo<strong>men</strong> <strong>and</strong> IBSwo<strong>men</strong>, symptom severity was greater in wo<strong>men</strong> with IBS.If only the seven higher quality studies were assessed,five reported a <strong>men</strong>strual cycle effect on IBS <strong>symptoms</strong>at time of <strong>men</strong>ses, while two did not. Bloating, gas <strong>and</strong><strong>bowel</strong> habit changes (diarrhoea more than constipation)were reported to increase at time of <strong>men</strong>ses. Only threeof these studies assessed <strong>symptoms</strong> prospectively <strong>and</strong>were from a single centre.Ali<strong>men</strong>t Pharmacol Ther 7ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.Schmulson 59Ab<strong>do</strong>minal distensionAb<strong>do</strong>minal bloatingStudyRisk ratio % Weight StudyRisk ratio % Weight(95% CI)(95% CI)Lee, OY 32 Lee, OY 321.19 (0.96, 1.48) 19.81.52 (1.27, 1.81) 22.3Celebi 540.94 (0.71, 1.26) 6.0Celebi 540.96 (0.67, 1.37) 8.5Han 91.16 (0.86, 1.58) 4.0Han 91.18 (0.85, 1.64) 9.9Lee, OY 321.17 (1.07, 1.29) 30.5Lee, OY 321.41 (1.16, 1.70) 20.4Lu 33 1.11 (1.04, 1.19) 32.5Lu 33Perveen 56 1.12 (1.04, 1.22) 36.61.06 (0.98, 1.15) 9.3LuMasud 251.00 (0.86, 1.16) 23.4331.15 (1.02, 1.31) 25.5Perveen 56Si 341.32 (0.95, 1.84) 13.61.14 (0.93, 1.41) 20.8Ringel 602.36 (1.50, 3.71) 9.1Smith 35 1.50 (1.17, 1.93) 18.61.47 (1.08, 2.01) 14.5Schmulson 59 1.17 (1.06, 1.29) 17.7Thompson 681.30 (1.12, 1.53) 24.6Thompson 36 1.47 (1.04, 2.06) 14.9Smith 351.50 (1.17, 1.93) 17.5Overall (95% CI)1.29 (1.06, 1.56)Overall (95% CI)1.37 (1.16, 1.61)0.8 1 20.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong> Favors <strong>men</strong> Favors wo<strong>men</strong>Infrequent stoolsHard/Lumpy stoolsStudyRisk ratio % WeightStudyRisk ratio(95% CI)(95% CI)% WeightOverall (95% CI)1.13 (1.08, 1.18)Overall (95% CI)1.21 (1.08, 1.36)0.8 1 20.8 1 2Favors <strong>men</strong> Favors wo<strong>men</strong> Favors <strong>men</strong> Favors wo<strong>men</strong>Figure 3 | Forest plots of the risk ratios <strong>and</strong> 95% confidence intervals for gender differences in IBS only studies evaluatingbloating, distension, hard ⁄ lumpy stools <strong>and</strong> infrequent stools are shown.Effect of <strong>men</strong>opausal status on IBS <strong>symptoms</strong>Three retrospective <strong>and</strong> one prospective survey comparedIBS <strong>symptoms</strong> in pre<strong>men</strong>opausal vs. post<strong>men</strong>opausalwo<strong>men</strong> 32, 37, 46, 55 <strong>and</strong> were considered to be of high quality.Sample sizes for pre<strong>men</strong>opausal wo<strong>men</strong> ranged from 58to 89 subjects <strong>and</strong> post<strong>men</strong>opausal wo<strong>men</strong> ranged from 55to 170 subjects. Amongst the three studies restricted toIBS, 32, 37, 55 nausea was the only symptom reported morefrequently by pre<strong>men</strong>opausal wo<strong>men</strong> than post<strong>men</strong>opausalwo<strong>men</strong>. 32 In the study by Cain et al., 55 various GI <strong>symptoms</strong>were reported less frequently by pre<strong>men</strong>opausalwo<strong>men</strong> than post<strong>men</strong>opausal wo<strong>men</strong>; however, these differenceswere not significant after adjusting for age.Amongst healthy wo<strong>men</strong>, gaseousness <strong>and</strong> excessive flatulencewere the only GI <strong>symptoms</strong> that were significantlymore prevalent in post<strong>men</strong>opausal wo<strong>men</strong>.Effect of hormone supple<strong>men</strong>tation on IBS <strong>symptoms</strong>Table 5 shows the results from four studies which evaluatedthe effect of hormone supple<strong>men</strong>tation on IBS<strong>symptoms</strong> in pre- or post<strong>men</strong>opausal wo<strong>men</strong>. Two ofthe studies were ran<strong>do</strong>mized controlled trials; one evaluatingthe effect of estradiol or progesterone in post<strong>men</strong>opausalwo<strong>men</strong> 50 was of high quality <strong>and</strong> the otherevaluating a gon<strong>do</strong>tropin-releasing hormone (GnRH)agonist in pre<strong>men</strong>opausal wo<strong>men</strong> 49 was of intermediatequality. The other two studies were not ran<strong>do</strong>mized controlledtrials. One consisted of a retrospective chartreview 48 <strong>and</strong> the other was a prospective study, 39 butboth achieved criteria for good quality.Two studies investigated the effect of hormonereplace<strong>men</strong>t therapy (HRT) on IBS <strong>symptoms</strong> inwo<strong>men</strong> over the age of 50 who were presumably post<strong>men</strong>opausal.48, 50 Ruigomez et al. 48 found that wo<strong>men</strong>who use HRT are more likely to develop IBS thanwo<strong>men</strong> who <strong>do</strong> not; however, the prevalence <strong>and</strong> severityof IBS <strong>symptoms</strong> were similar among non-HRTusers <strong>and</strong> HRT users. Gonenne et al. 50 found that post<strong>men</strong>opausalhealthy wo<strong>men</strong> who were given estradiol orprogesterone therapy alone for 7 days were more likely8 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>Table 4 | Evidence table of studies comparing <strong>men</strong>strual cycle effect on IBS <strong>symptoms</strong>Study Population (N) Study design SettingMenstrualcycle assess<strong>men</strong>tIBSdiagnosticcriteria Findings QAJackson et al. 41 Healthycontrols (20)Prospective(daily diary)Not specified Menses: day 1–4;follicular: day 8–10;luteal: day 18–20;pre<strong>men</strong>strual: day24–28N ⁄ A Stool form was significantlylooser at <strong>men</strong>ses comparedto luteal phase; There wasnot a significant phase effecton number of stools per day9Hinds et al. 62 Healthycontrols (25)Retrospective Not specified Recall N ⁄ A 96% reported change in <strong>bowel</strong>habit before <strong>and</strong> during<strong>men</strong>ses; 72% reported loosestools during <strong>men</strong>ses; 32%reported constipation theweek prior to <strong>men</strong>ses9Simmons et al. 44 Healthycontrols (7)Prospective(daily diary)Not specified Basal bodytemperatureN ⁄ A No significant phase effect onstool form; 1 of 7 subjectsreported constipation beforeor during <strong>men</strong>ses; 2 of 7subjects reported diarrhoea atthe beginning of <strong>men</strong>ses11Lee et al. 43 GI clinicpatients (193)Cross-sectional(survey)3° care Menstrual: day 0–6;proliferative: day 7–14; secretory: afterday 15Rome II 50.8% of wo<strong>men</strong> metdiagnostic criteria for IBS. Nosignificant phase effect forab<strong>do</strong>minal pain, constipation,diarrhoea, ab<strong>do</strong>minaldistension, tenesmus13Altman et al. 63 IBS (114) Prospective(daily diary)1° care <strong>and</strong>communityMenses: day 1; lutealphase: 7–10 daysprior to onset of<strong>men</strong>sesDiagnosismade by health provider;criteria not specifiedNo significant phase effect onab<strong>do</strong>minal or stomach pain13Chang et al. 37 IBS (380) Retrospective 3° care <strong>and</strong>communityRecall Rome I 40% of bloating patients <strong>and</strong>43% of bloating + distensionpatients reported thatbloating was related to<strong>men</strong>strual cycle15Ali<strong>men</strong>t Pharmacol Ther 9ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.Table 4 | (Continued)Study Population (N) Study design SettingMenstrualcycle assess<strong>men</strong>tIBSdiagnosticcriteria Findings QAHoughton et al. 40 IBS (29) Prospective(daily diary)Not specified Menses: day 1–4;follicular: day 8–10;luteal: day 18–20;pre<strong>men</strong>strual: day24–28Rome I There were significant phaseeffects on ab<strong>do</strong>minal pain,bloating, stool frequency <strong>and</strong>loose stools11Lee et al. 32 IBS (477) Retrospective 3° care <strong>and</strong>communityRecall Rome Overall 40% of wo<strong>men</strong> <strong>and</strong>50.8% of wo<strong>men</strong>
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>Table 4 | (Continued)Study Population (N) Study design SettingMenstrualcycle assess<strong>men</strong>tIBSdiagnosticcriteria Findings QAHoughton et al. 57 IBS-D (39)Healthycontrols (19)Cross-sectional University clinic,general practices,advertise<strong>men</strong>tLuteal phase (days18–20 of cycle) ortaking OCP wereclassified as highprogesterone ⁄oestrogen; <strong>men</strong>ses(days 2–3) wasclassified as lowprogesterone ⁄oestrogen: <strong>men</strong>ses(days 2–3 of cycle)Rome II No differences in severity ofpain, bloating, urgency oroverall <strong>symptoms</strong> <strong>between</strong>high <strong>and</strong> low progesterone ⁄oestrogen conditions in IBS-Dwo<strong>men</strong> or healthy wo<strong>men</strong>11Kane et al. 42 IBS (46)Healthycontrols (90)Retrospective 2° care <strong>and</strong>communityRecall Rome Increased diarrhoea wasreported significantly moreoften during pre<strong>men</strong>strualperiod <strong>and</strong> <strong>men</strong>ses in IBS vs.controls. Increasedconstipation was less oftenreported than diarrhoea, butwas significantly moreprevalent in IBS vs. controlsduring <strong>men</strong>ses. There was asignificant <strong>men</strong>strual cycleeffect on ab<strong>do</strong>minal pain inIBS16Whitehead et al. 45 IBS (72)Healthycontrols (234)Retrospective 1° <strong>and</strong> 2° care Recall Manning IBS were more likely thancontrols to report <strong>men</strong>sesrelatedincreases in gas (39–48% vs. 14%), diarrhoea(29–32% vs. 19%) <strong>and</strong>constipation (18–24% vs.11%)11QA, quality assess<strong>men</strong>t; GI, gastrointestinal; N ⁄ A, not applicable; 1°, primary; 2°, secondary; 3°, tertiary; OCP, oral-contraceptive pills.Ali<strong>men</strong>t Pharmacol Ther 11ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.Number of studies6420Menstrual cycle effectNo <strong>men</strong>strual cycle effectLoose stools Bloating Ab<strong>do</strong>minalpainStoolfrequencyChange in<strong>bowel</strong> habitFigure 4 | The number of studies that tested for a significanteffect of IBS <strong>symptoms</strong> on <strong>men</strong>strual cycle ispresented. The P-value of significance was specific toeach study. One study was not included in the figurebecause statistical analysis of <strong>men</strong>strual cycle effect onbloating was not performed. 37 Another study was notincluded because it did not specifically evaluate a <strong>men</strong>strualcycle effect on these <strong>symptoms</strong>. 45to have looser stools <strong>and</strong> greater ease of passage thanthose on placebo.Two studies evaluated the effect of hormone supple<strong>men</strong>tationon IBS <strong>symptoms</strong> in pre<strong>men</strong>opausal wo<strong>men</strong>.One study assessed the effect of oral-contraceptive pills(OCP), whereas the other assessed the effect of a GnRHagonist. 38, 49 Heitkemper et al. 38 found that OCP use bywo<strong>men</strong> with IBS was associated with lower ab<strong>do</strong>minalpain severity compared with non-OCP users, but thisdifference did not maintain significance after correctingfor multiple comparisons. Palomba et al. 49 found thattreat<strong>men</strong>t with a GnRH agonist improved the severity ofIBS <strong>symptoms</strong> compared with placebo.DISCUSSIONDue to conflicting data in the literature regarding genderdifferences in IBS, we performed a systematic review toinvestigate if there are differences in IBS <strong>symptoms</strong><strong>between</strong> genders, <strong>and</strong> further evaluated the literatureregarding the relationship <strong>between</strong> IBS <strong>symptoms</strong>, <strong>men</strong>strualcycle phase <strong>and</strong> <strong>men</strong>opause. Our study has fourmain findings: (i) wo<strong>men</strong> experience a greater prevalenceof IBS <strong>symptoms</strong> than <strong>men</strong>, particularly constipationrelated<strong>symptoms</strong>; (ii) wo<strong>men</strong> appear to have morefrequent <strong>and</strong> severe IBS <strong>symptoms</strong> during <strong>men</strong>ses comparedwith other phases of the <strong>men</strong>strual cycle; (iii) theeffect of hormonal therapy on IBS <strong>symptoms</strong> cannot bedetermined based on limited available data; <strong>and</strong> (iv)there is a lack of studies comparing IBS <strong>symptoms</strong> inpre- <strong>and</strong> post<strong>men</strong>opausal wo<strong>men</strong>.For the most part, the occurrence <strong>and</strong> diagnosis of6, 29, 64IBS is more common in wo<strong>men</strong> than in <strong>men</strong>.Female gender is a significant independent risk factor forthe develop<strong>men</strong>t of IBS, 65 including postinfectious IBS. 66In cross-sectional surveys conducted in the US, 67 Canada68 <strong>and</strong> Israel, 69 wo<strong>men</strong> reported IBS <strong>symptoms</strong> 1.5 to2 times more commonly than <strong>men</strong>. Greater health careseeking <strong>and</strong> referral for IBS in wo<strong>men</strong> may in part bedue to increased IBS severity 32, 70, 71 <strong>and</strong> greater impactof <strong>symptoms</strong> on health related quality of life in wo<strong>men</strong>with IBS compared with <strong>men</strong>. 70, 72, 73 However, populationstudies conducted in Asia suggest that the prevalenceof IBS in <strong>men</strong> <strong>and</strong> wo<strong>men</strong> is similar. 19, 74–76 Thisdifference may be largely due to cultural reasons. InAsia, <strong>men</strong> see physicians as much <strong>and</strong> more often thanwo<strong>men</strong> possibly for cultural <strong>and</strong> economic reasons. 76–79Gender differences in IBS <strong>symptoms</strong>Our meta-analysis reveals that wo<strong>men</strong> more frequentlyreport individual IBS <strong>symptoms</strong> than <strong>men</strong>. In generalpopulation studies, which included individuals with IBS,wo<strong>men</strong> reported a greater prevalence of the IBS diagnostic(i.e. pain-related) <strong>symptoms</strong> than <strong>men</strong>. These findingsare consistent with studies which showed an enhancedperception of pain or discomfort to distension in the80, 81colon <strong>and</strong> rectum in wo<strong>men</strong> vs. <strong>men</strong>.Overall, wo<strong>men</strong> had a greater prevalence of constipation-associated<strong>symptoms</strong>, particularly bloating <strong>and</strong>ab<strong>do</strong>minal distension, than <strong>men</strong>. Men had a greaterprevalence of diarrhoea-associated <strong>symptoms</strong> of loose ⁄ -watery stools <strong>and</strong> increased stool frequency in the IBSonly studies, but not in the general population studies.This is consistent with studies demonstrating a female67, 82, 83pre<strong>do</strong>minance in IBS-C <strong>and</strong> chronic constipation.82, 84 Several studies have found that wo<strong>men</strong> haveslower colonic transit than <strong>men</strong>. 85–87The generally higher IBS symptom reporting in wo<strong>men</strong>than <strong>men</strong> may be due to several reasons. Since wo<strong>men</strong>with IBS tend to have significantly more healthcare visitsthan <strong>men</strong>, 88 studies which used healthcare-based recruit<strong>men</strong>tmethods may underestimate the symptom prevalencein <strong>men</strong>. Another plausible explanation is thatwo<strong>men</strong> tend to recall their <strong>symptoms</strong> better than <strong>men</strong>. 89However, this is not likely to explain why constipationassociated<strong>symptoms</strong> were reported more commonly inwo<strong>men</strong> than in <strong>men</strong>, while diarrhoea-associated <strong>symptoms</strong>were reported more often in <strong>men</strong>. Gender differenceshave been demonstrated in GI function, including12 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>Table 5 | Evidence table of studies comparing hormone supple<strong>men</strong>t effect on IBSStudyTreat<strong>men</strong>t groups(N) PopulationMenopausalstatus Study design Age (years) SettingIBSdiagnosticcriteria Symptoms QARuigomez et al. 48 IBS HRT users(405); IBS HRTnever users(255)IBS Not specified Prospective 50–69 1° care Not specified IBS <strong>symptoms</strong> were similaramong users of HRT <strong>and</strong> HRTnever users (data notprovided)15Palomba et al. 49 Leuprolide acetatedepot (LAD) plustibolone (36);LAD plus placebo(37); placebo(39)IBS Pre<strong>men</strong>opausal RCT 25.5 (mean) 2° care Rome II There was an improve<strong>men</strong>tfrom baseline <strong>and</strong> vs. placeboin ab<strong>do</strong>minal discomfort <strong>and</strong>distension, nausea, frequency<strong>and</strong> consistency, diarrhoea,constipation <strong>and</strong> bloating forboth treat<strong>men</strong>t groups17Gonenne et al. 50 Placebo (12),progesterone(13), estradiol(12), combinedprogesterone <strong>and</strong>estradiol (12)Controls Post<strong>men</strong>opausal RCT 40–65 Not specified N ⁄ A Treat<strong>men</strong>teffect of looser stoolconsistency scores withprogesterone alone, estradiolalone <strong>and</strong>progesterone + estradiol;Greater ease of passagescores for estradiol alone; Notreat<strong>men</strong>t effect on stoolfrequency, stool consistencyor sense of incompletepassage24Heitkemper et al. 38 IBS oralcontraceptive(56); IBS non-OCP (93)IBS Pre<strong>men</strong>opausal Prospective 32.5 (mean) GeneralpopulationRome I OCP users reported less severeab<strong>do</strong>minal pain than non-OCPusers but this difference didnot maintain significance aftermultiple comparisons. Therewere no significantdifferences in other individualGI <strong>symptoms</strong>16RCT, ran<strong>do</strong>mized controlled trial; 1°, primary; 2°, secondary; 3°, tertiary; HRT, hormone replace<strong>men</strong>t therapy; OCP, oral-contraceptive pills; N ⁄ A, not applicable.Ali<strong>men</strong>t Pharmacol Ther 13ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.transit time, visceral perception, brain activation patterns<strong>and</strong> colonic mucosal mast cell count 12, 13, 81, 90, 91 whichcan conceivably contribute to the greater prevalence ofIBS <strong>symptoms</strong> in wo<strong>men</strong> <strong>and</strong> the gender differences in<strong>bowel</strong> habits.Most Western studies reported a higher prevalence ofindividual IBS <strong>symptoms</strong> in wo<strong>men</strong> compared with<strong>men</strong>. 26, 27, 29, 30, 35, 36 Similarly, eight of the ten Easternstudies found that more wo<strong>men</strong> reported individual IBS<strong>symptoms</strong> than <strong>men</strong> 9, 31, 33, 34, 51, 53, 56, 58 ; however oneof these studies also reported higher prevalences of loosestools <strong>and</strong> increased stool frequency in <strong>men</strong>. 33 These studieswere conducted mainly in community <strong>and</strong> universityclinic populations, although one surveyed secondary clinicpatients. Interestingly, two studies did not find a genderdifference in individual <strong>symptoms</strong>, but reported a higherratio of wo<strong>men</strong>-to-<strong>men</strong> with Rome positive IBS (1.3–1.8:1). 25, 54 One of these studies was conducted in a ruralcommunity in Bangladesh 25 <strong>and</strong> the other in an urbancommunity in Turkey. 54 Thus, this meta-analysis supportsa higher overall prevalence of IBS <strong>symptoms</strong> in wo<strong>men</strong>than in <strong>men</strong> in Western <strong>and</strong> Eastern countries, althoughthe differences are relatively modest. This review overcomesthe limitations of previous epidemiological investigations9, 26–28, 30–36, 47 because data from studiesconducted in both Eastern <strong>and</strong> Western populations areincluded. However, additional studies are needed to investigatehow the interactions <strong>between</strong> genetic, environ<strong>men</strong>tal<strong>and</strong> ⁄ or cultural factors contribute to gender differences inIBS <strong>symptoms</strong> <strong>and</strong> may differ across diverse cultures.The relatively small, but significant gender differencesin the prevalence of individual IBS <strong>symptoms</strong> suggeststhat gender effects may be confounded by other factorsthat significantly influence the presence of IBS <strong>symptoms</strong>.These include psychological <strong>and</strong> social factors thatcan affect symptom reporting, health care seeking <strong>and</strong>global outcomes in IBS. 92 For example, studies havereported that a previous history of abuse <strong>and</strong> other traumaticevents or stressors are associated with more severepain <strong>and</strong> greater symptom severity in IBS. 93–96Limitations of our meta-analysis include the extensiveheterogeneity of the studies, which may in part explainthe low RR estimates. For example, the diagnostic criteriaused for IBS varied <strong>between</strong> studies. This is notablebecause gender differences in the prevalence of IBS <strong>vary</strong>according to criteria used. 97 In a population-based,cross-sectional survey study in Olmstead County, Minnesota,there was a greater prevalence of wo<strong>men</strong> with IBSif the Manning criteria were used, but a higher prevalenceof <strong>men</strong> with IBS if the Rome criteria were used. 98Menstrual cycle effect on IBS <strong>symptoms</strong>Our systematic review found that IBS <strong>symptoms</strong> areheightened at time of <strong>men</strong>ses. Enhanced visceral perceptionat <strong>men</strong>ses is supported by the finding of decreasedsensory thresholds to rectal distension compared withother phases of the <strong>men</strong>strual cycle. 40 One plausiblemechanism that is supported by some animal <strong>and</strong>human studies is that declining or low ovarian hormonelevels at time of <strong>men</strong>ses may underlie the increased GI<strong>symptoms</strong> <strong>and</strong> discomfort across the <strong>men</strong>strual cycle. 99A study by Laessle <strong>and</strong> colleagues 100 showed that progesteronelevels negatively correlated with pain-related<strong>symptoms</strong> (i.e. back pain <strong>and</strong> headache) which supportsthat lower levels of female sex hormones are associatedwith greater somatic pain. It is conceivable that wo<strong>men</strong>have more prevalent <strong>and</strong> severe IBS <strong>symptoms</strong> at time of<strong>men</strong>ses when progesterone (<strong>and</strong> oestrogen) decline fromhigh to low levels. There are other possible mechanismsinvolved in GI function to explain these findings. Forexample, gender differences exist in postpr<strong>and</strong>ial serotoninlevels in IBS-D 101, 102 <strong>and</strong> in colonic mucosal mastcell counts in IBS. 91 Both have been found to correlatewith IBS <strong>symptoms</strong> <strong>and</strong> potentially have a key role in thepathophysiology of IBS. 103 In addition, mast cell secretionis affected by both oestrogen <strong>and</strong> progesterone. 104Although more studies reported increased diarrhoea attime of <strong>men</strong>ses than increased constipation, there weretwo retrospective recall studies which found that somewo<strong>men</strong> reported increased diarrhoea <strong>and</strong> others reportedincreased constipation (Table 4). 42, 45 It is possible thatan increase in a particular <strong>bowel</strong> habit would be reportedby IBS patients with that pre<strong>do</strong>minant <strong>bowel</strong> subtype.For example, wo<strong>men</strong> with IBS-D may be more likely toreport increased diarrhoea than constipation, while IBS-C patients may be more likely to report increased constipation.However, this information was not availablein the studies to determine if this could explain thesefindings.Despite a relatively adequate number of studies, metho<strong>do</strong>logicallimitations in these studies could have affectedthe results. Half of the studies were based on symptomrecall. As wo<strong>men</strong> are likely to report a greater severity of<strong>symptoms</strong> retrospectively than prospectively, 105 the retrospectivestudies may overestimate the effect of <strong>men</strong>strualcycle on IBS <strong>symptoms</strong> <strong>and</strong> are less accurate thanprospective assess<strong>men</strong>t. In addition, confirmation of<strong>men</strong>strual cycle phase should be performed using ovulationkits, although this was only <strong>do</strong>ne in two of the 12studies. A review of the effect of <strong>men</strong>strual cycle phaseon experi<strong>men</strong>tal pain response found a lack of st<strong>and</strong>ard-14 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>ized operational definitions for identifying <strong>men</strong>strualcycle phases. 106 More studies with an optimal studydesign (e.g. use of ovulation kits, prospective daily symptomassess<strong>men</strong>t, sufficient sample sizes) are needed totruly assess the validity of the <strong>men</strong>strual cycle effect onIBS <strong>symptoms</strong>.Menopausal status effect on IBS <strong>symptoms</strong>Due to the small number of studies that compared GI<strong>symptoms</strong> in pre- <strong>and</strong> post<strong>men</strong>opausal wo<strong>men</strong>, there isinsufficient evidence to determine the effect of <strong>men</strong>opausalstatus on IBS <strong>symptoms</strong>. However, the limiteddata suggest that pre<strong>men</strong>opausal wo<strong>men</strong> with IBS aremore likely to experience nausea than post<strong>men</strong>opausalwo<strong>men</strong> with IBS. This finding is supported by studieswhich have shown that nausea <strong>and</strong> vomiting thatoccurred post-operatively, 107, 108 <strong>and</strong> during pregnancy,are associated with high levels oestrogen109, 110<strong>and</strong> ⁄ or progesterone levels.In one study, healthy post<strong>men</strong>opausal wo<strong>men</strong>reported gas <strong>and</strong> excessive flatulence significantly morethan pre<strong>men</strong>opausal wo<strong>men</strong>. 46 To our knowledge, therehave been no studies that have compared intestinal gasclearance or colon transit times in pre- <strong>and</strong> post<strong>men</strong>opausalwo<strong>men</strong>.Effect of hormone supple<strong>men</strong>t on IBS <strong>symptoms</strong>The available studies provided limited information <strong>and</strong>therefore a conclusion on the effects of hormone supple<strong>men</strong>tationcannot be definitively determined. However,the available evidence suggests that use of OCPs <strong>and</strong> aGnRH agonist by pre<strong>men</strong>opausal wo<strong>men</strong> may be protectiveof IBS <strong>symptoms</strong>, although further studies areneeded. These medications act differently on the hypothalamic–pituitary–gonadalaxis. OCPs prevent ovulationbecause the progesterone derivative inhibits the release ofGnRH by the hypothalamus thereby decreasing therelease of follicular-stimulating hormone (FSH) <strong>and</strong>luteinizing hormone (LH) by the anterior pituitary, an<strong>do</strong>estrogen inhibits follicular develop<strong>men</strong>t. In contrast,leuprolide, the GnRH agonist, stimulates the release ofFSH <strong>and</strong> LH, which suppress the secretion of ovarianhormones. Un<strong>do</strong>ubtedly, more studies are needed todetermine conclusively the effect of hormone supple<strong>men</strong>tson IBS <strong>symptoms</strong>.CONCLUSIONOur study demonstrates that wo<strong>men</strong> overall have agreater prevalence of IBS <strong>symptoms</strong> than <strong>men</strong>, particularlythose associated with constipation. However,within the IBS patient group, <strong>men</strong> have more diarrhoea<strong>symptoms</strong> than wo<strong>men</strong>. There are some limitations inthe quality, metho<strong>do</strong>logy <strong>and</strong> number of studies evaluatingthe effect of <strong>men</strong>strual cycle, hormone supple<strong>men</strong>tation<strong>and</strong> <strong>men</strong>opausal status on IBS <strong>symptoms</strong>.Notably, most studies relied on symptom recall. Nonetheless,existing data raise the possibility that there maybe a female sex hormone effect on IBS <strong>symptoms</strong> aswell as on GI function. It is plausible that this maycontribute to the increased prevalence <strong>and</strong> greater vulnerabilityto develop IBS, the higher prevalence of constipation<strong>symptoms</strong> <strong>and</strong> the increased severity of<strong>symptoms</strong> at time of <strong>men</strong>ses in wo<strong>men</strong>. In addition tothe need for more, well-designed studies, there shouldbe a greater attempt to recruit adequate <strong>and</strong> comparablenumbers of <strong>men</strong> <strong>and</strong> wo<strong>men</strong> with <strong>and</strong> without IBS,<strong>and</strong> attention should be paid to assessing <strong>and</strong> controllingfor <strong>men</strong>strual cycle phase <strong>and</strong> <strong>men</strong>opausal statusin clinical study design as they can potentially affectstudy results.ACKNOWLEDGEMENTSDeclaration of personal interests: The authors thankMelissa Alberto <strong>and</strong> Teresa Olivas for their assistancein the preparation of the work. Mopelola Adeyemohas nothing to declare. Brennan Spiegel has served asa consultant for Prometheus Laboratories, Astra-Zeneca,TAP, Takeda, Ironwood, <strong>and</strong> Novartis. He hasreceived research funding from Takeda, Rose, Prometheus,Amgen, Shire, <strong>and</strong> Novartis. Lin Chang hasserved as a consultant for Prometheus Laboratories,Takeda, Forest, Albireo, McNeil, Rose Pharma, Glaxo-SmithKline, Salix, Ocera <strong>and</strong> Movetis. She has receivedresearch funding from Takeda, Rose <strong>and</strong> Prometheus.Declaration of funding interests: This study was fundedby NIH Grants Nos P50 DK64539 <strong>and</strong> R24AT002681.SUPPORTING INFORMATIONAdditional Supporting Information may be found in theonline version of this article:Appendix S1. Down <strong>and</strong> Black checklist for measuringstudy quality.Please note: Wiley-Blackwell are not responsible forthe content or functionality of any supporting materialssupplied by the authors. Any queries (other than missingmaterial) should be directed to the corresponding authorfor the article.Ali<strong>men</strong>t Pharmacol Ther 15ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.REFERENCES1. Drossman DA. The functional gastrointestinaldisorders <strong>and</strong> the Rome IIIprocess. Gastroenterology 2006; 130:1377–90.2. Kang JY. Systematic review: the influenceof geography <strong>and</strong> ethnicity in<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>. Ali<strong>men</strong>tPharmacol Ther 2005; 21: 663–76.3. Camilleri M, Choi MG. Review article:<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>. Ali<strong>men</strong>t PharmacolTher 1997; 11: 3–15.4. Talley NJ. Irritable <strong>bowel</strong> <strong>syndrome</strong>:definition, diagnosis <strong>and</strong> epidemiology.Baillieres Best Pract Res Clin Gastroenterol1999; 13: 371–84.5. Thompson DG. GLP-1 <strong>and</strong> the gut. Gut2000; 46: 591.6. Muller-Lissner SA, Bollani S, BrummerRJ, et al. Epidemiological aspects of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> in Europe <strong>and</strong>North America. Digestion 2001; 64:200–4.7. Drossman DA, Camilleri M, Mayer EA,Whitehead WE. AGA technical reviewon <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>. Gastroenterology2002; 123: 2108–31.8. Husain N, Chaudhry IB, Jafri F, NiazSK, To<strong>men</strong>son B, Creed F. A population-basedstudy of <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>in a non-Western population.Neurogastroenterol Motil 2008; 20:1022–9.9. Han SH, Lee OY, Bae SC, et al. Prevalenceof <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> inKorea: population-based survey usingthe Rome II criteria. J GastroenterolHepatol 2006; 21: 1687–92.10. Chang L, Heitkemper MM. Genderdifferences in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Gastroenterology 2002; 123: 1686–701.11. Talley NJ, Zinsmeister AR, Melton IIILJ. Irritable <strong>bowel</strong> <strong>syndrome</strong> in a community:symptom subgroups, risk factors,<strong>and</strong> health care utilization. Am JEpidemiol 1995; 142: 76–83.12. Viramontes BE, Camilleri M, McKinzieS, Pardi DS, Burton D, Thomforde GM.Gender-related differences in slowingcolonic transit by a 5-HT 3 antagonistin subjects with diarrhea-pre<strong>do</strong>minant<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>. Am J Gastroenterol2001; 96: 2671–9.13. Rao SS, Sadeghi P, Beaty J, Kavlock R,Ackerson K. Ambulatory 24-h colonicmanometry in healthy humans. Am JPhysiol Gastrointest Liver Physiol 2001;280: G629–39.14. Soffer EE, Kongara K, Achkar JP,Gannon J. Colonic motor function inhumans is not affected by gender. DigDis Sci 2000; 45: 1281–4.15. Drossman DA, Chey W, Panas R,Wahle A, Scott C, Ueno R. Lubiprostonesignificantly improves symptomrelief rates in adults with <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> <strong>and</strong> constipation(IBS-C): data from two twelve week,ran<strong>do</strong>mized, placebo controlled <strong>do</strong>ubleblind trials. Gastroenterology 2007;132: 2586–7.16. Chang L, Ameen VZ, Dukes GE,McSorley DJ, Carter EG, Mayer EA. A<strong>do</strong>se-ranging, phase II study of the efficacy<strong>and</strong> safety of alosetron in <strong>men</strong>with diarrhea-pre<strong>do</strong>minant IBS. Am JGastroenterol 2005; 100: 115–23.17. Andresen V, Montori VM, Keller J,West CP, Layer P, Camilleri M. Effectsof 5-hydroxytryptamine (serotonin)type 3 antagonists on symptom relief<strong>and</strong> constipation in nonconstipated <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>: a systematicreview <strong>and</strong> meta-analysis of ran<strong>do</strong>mizedcontrolled trials. Clin GastroenterolHepatol 2008; 6: 545–55.18. Heitkemper MM, Chang L. Do fluctuationsin ovarian hormones affect gastrointestinal<strong>symptoms</strong> in wo<strong>men</strong> with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>? Gend Med2009; 6(Suppl 2): 152–67.19. Gwee KA. Irritable <strong>bowel</strong> <strong>syndrome</strong> indeveloping countries – a disorder ofcivilization or colonization?Neurogastroenterol Motil 2005; 17:317–24.20. Downs SH, Black N. The feasibility ofcreating a checklist for the assess<strong>men</strong>tof the metho<strong>do</strong>logical quality both ofran<strong>do</strong>mised <strong>and</strong> non-ran<strong>do</strong>mised studiesof health care interventions. J EpidemiolCommunity Health 1998; 52:377–84.21. McMillan AM, Lan<strong>do</strong>rf KB, Barrett JT,Menz HB, Bird AR. Diagnostic imagingfor chronic plantar heel pain: a systematicreview <strong>and</strong> meta-analysis. J FootAnkle Res 2009; 2: 32.22. Strazzullo P, D’Elia L, K<strong>and</strong>ala NB,Cappuccio FP. Salt intake, stroke, <strong>and</strong>cardiovascular disease: meta-analysis ofprospective studies. BMJ 2009; 339:b4567.23. Tonelli M, Wiebe N, Hemmelgarn B,et al. Trace ele<strong>men</strong>ts in hemodialysispatients: a systematic review <strong>and</strong> metaanalysis.BMC Med 2009; 7: 25.24. Egger M, Altman DG, Smith GD, eds.Systematic reviews in health care: metaanalysisin context. 2nd ed. Lon<strong>do</strong>n:BMJ Publish Group, 2001.25. Masud MA, Hasan M, Khan AK.Irritable <strong>bowel</strong> <strong>syndrome</strong> in a ruralcommunity in Bangladesh: prevalence,<strong>symptoms</strong> pattern, <strong>and</strong> health care seekingbehavior. Am J Gastroenterol 2001;96: 1547–52.26. Bouchoucha M, Devroede G, Dorval E,Faye A, Arhan P, Arsac M. Differentseg<strong>men</strong>tal transit times in patients with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> <strong>and</strong> ‘‘normal’’colonic transit time: is there a correlationwith <strong>symptoms</strong>? Tech Coloproctol2006; 10: 287–96.27. Talley NJ, Zinsmeister AR, Van Dyke C,Melton LJ. Epidemiology of colonic<strong>symptoms</strong> <strong>and</strong> <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Gastroenterology 1991; 101:927–34.28. Talley NJ, Boyce P, Jones M. Identificationof distinct upper <strong>and</strong> lower gastrointestinalsymptom groupings in anurban population. Gut 1998; 42: 690–5.29. Taub E, Cuevas JL, Cook EW, CrowellM, Whitehead WE. Irritable <strong>bowel</strong> <strong>syndrome</strong>defined by factor analysis. Gender<strong>and</strong> race comparisons. Dig Dis Sci1995; 40: 2647–55.30. Tuteja AK, Talley NJ, Joos SK, TolmanKG, Hickam DH. Ab<strong>do</strong>minal bloatingin employed adults: prevalence, risk factors,<strong>and</strong> association with other <strong>bowel</strong>disorders. Am J Gastroenterol 2008; 103:1241–8.31. Zuckerman MJ, Nguyen G, Ho H,Nguyen L, Gregory GG. A survey of<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> in Vietnamusing the Rome criteria. Dig Dis Sci2006; 51: 946–51.32. Lee OY, Mayer EA, Schmulson M,Chang L, Naliboff B. Gender-related differencesin IBS <strong>symptoms</strong>. Am J Gastroenterol2001; 96: 2184–93.33. Lu CL, Chang FY, Lang HC, ChenCY, Luo JC, Lee SD. Gender differenceon the <strong>symptoms</strong>, health-seekingbehaviour, social impact <strong>and</strong> sleepquality in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>: aRome II-based survey in an apparenthealthy adult Chinese population inTaiwan. Ali<strong>men</strong>t Pharmacol Ther 2005;21: 1497–505.34. Si JM, Wang LJ, Chen SJ, Sun LM, DaiN. Irritable <strong>bowel</strong> <strong>syndrome</strong> consultersin Zhejiang province: the <strong>symptoms</strong>pattern, pre<strong>do</strong>minant <strong>bowel</strong> habit subgroups<strong>and</strong> quality of life. World J Gastroenterol2004; 10: 1059–64.35. Smith RC, Greenbaum DS, VancouverJB, et al. Gender differences inManning criteria in the <strong>irritable</strong> <strong>bowel</strong><strong>syndrome</strong>. Gastroenterology 1991; 100:591–5.36. Thompson WG. Gender differences in<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>s. Eur J GastroenterolHepatol 1997; 9: 299–302.16 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd
Meta-analysis: gender variance in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>37. Chang L, Lee OY, Naliboff B, SchmulsonM, Mayer EA. Sensation of bloating<strong>and</strong> visible ab<strong>do</strong>minal distension inpatients with <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Am J Gastroenterol 2001; 96: 3341–7.38. Heitkemper MM, Cain KC, Jarrett ME,Burr RL, Hertig V, Bond EF. Symptomsacross the <strong>men</strong>strual cycle in wo<strong>men</strong>with <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>. Am JGastroenterol 2003; 98: 420–30.39. Heitkemper MM, Jarrett M, Cain KC,Shaver J, Walker E, Lewis L. Daily gastrointestinal<strong>symptoms</strong> in wo<strong>men</strong> with<strong>and</strong> without a diagnosis of IBS. Dig DisSci 1995; 40: 1511–9.40. Houghton LA, Lea R, Jackson N,Whorwell PJ. The <strong>men</strong>strual cycleaffects rectal sensitivity in patients with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> but not healthyvolunteers. Gut 2002; 50: 471–4.41. Jackson NA, Houghton LA, WhorwellPJ, Currer B. Does the <strong>men</strong>strual cycleaffect anorectal physiology? Dig Dis Sci1994; 39: 2607–11.42. Kane SV, Sable K, Hanauer SB. The<strong>men</strong>strual cycle <strong>and</strong> its effect oninflammatory <strong>bowel</strong> disease <strong>and</strong> <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>: a prevalence study.Am J Gastroenterol 1998; 93: 1867–72.43. Lee SY, Kim JH, Sung IK, et al. Irritable<strong>bowel</strong> <strong>syndrome</strong> is more common inwo<strong>men</strong> regardless of the <strong>men</strong>strualphase: a Rome II-based survey. J KoreanMed Sci 2007; 22: 851–4.44. Simmons L, Heitkemper M, Shaver J.Gastrointestinal function during the<strong>men</strong>strual cycle. Health Care Wo<strong>men</strong>Int 1988; 9: 201–9.45. Whitehead WE, Cheskin LJ, Heller BR,et al. Evidence for exacerbation of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> during <strong>men</strong>ses.Gastroenterology 1990; 98: 1485–9.46. Triadafilopoulos G, Finlayson M, GrelletC. Bowel dysfunction in post<strong>men</strong>opausalwo<strong>men</strong>. Wo<strong>men</strong> Health 1998;27: 55–66.47. Barakzai MD, Gregory J, Fraser D. Theeffect of culture on symptom reporting:Hispanics <strong>and</strong> <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.J Am Acad Nurse Pract 2007; 19:261–7.48. Ruigomez A, Garcia Rodriguez LA, JohanssonS, Wall<strong>and</strong>er MA. Is hormonereplace<strong>men</strong>t therapy associated with anincreased risk of <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>?Maturitas 2003; 44: 133–40.49. Palomba S, Orio F Jr., Manguso F, et al.Leuprolide acetate treat<strong>men</strong>t with <strong>and</strong>without coadministration of tibolone inpre<strong>men</strong>opausal wo<strong>men</strong> with <strong>men</strong>strualcycle-related <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Fertil Steril 2005; 83: 1012–20.50. Gonenne J, Esf<strong>and</strong>yari T, Camilleri M,et al. Effect of female sex hormonesupple<strong>men</strong>tation <strong>and</strong> withdrawal ongastrointestinal <strong>and</strong> colonic transit inpost<strong>men</strong>opausal wo<strong>men</strong>. NeurogastroenterolMotil 2006; 18: 911–8.51. Kim YJ, Ban DJ. Prevalence of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>, influence of lifestylefactors <strong>and</strong> <strong>bowel</strong> habits in Korean collegestudents. Int J Nurs Stud 2005; 42:247–54.52. S<strong>and</strong>ler RS, Stewart WF, Liberman JN,Ricci JA, Zorich NL. Ab<strong>do</strong>minal pain,bloating, <strong>and</strong> diarrhea in the UnitedStates: prevalence <strong>and</strong> impact. Dig DisSci 2000; 45: 1166–71.53. Tan YM, Goh KL, Muhidayah R, OoiCL, Salem O. Prevalence of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> in young adult Malaysians:a survey among medical students. JGastroenterol Hepatol 2003; 18: 1412–6.54. Celebi S, Acik Y, Deveci SE, et al. Epidemiologicalfeatures of <strong>irritable</strong> <strong>bowel</strong><strong>syndrome</strong> in a Turkish urban society. JGastroenterol Hepatol 2004; 19: 738–43.55. Cain KC, Jarrett ME, Burr RL, Rosen S,Hertig VL, Heitkemper MM. Genderdifferences in gastrointestinal, psychological,<strong>and</strong> somatic <strong>symptoms</strong> in <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>. Dig Dis Sci 2009;54: 1542–9.56. Perveen I, Hasan M, Masud MA, BhuiyanMM, Rahman MM. Irritable <strong>bowel</strong><strong>syndrome</strong> in a Bangladeshi urban community:prevalence <strong>and</strong> health careseeking pattern. Saudi J Gastroenterol2009; 15: 239–43.57. Houghton LA, Brown H, Atkinson W,et al. 5-hydroxytryptamine signalling in<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> with diarrhoea:effects of gender <strong>and</strong> <strong>men</strong>strualstatus. Ali<strong>men</strong>t Pharmacol Ther 2009;30: 919–29.58. Shen L, Kong H, Hou X. Prevalence of<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> <strong>and</strong> its relationshipwith psychological stress statusin Chinese university students. J GastroenterolHepatol 2009; 24: 1885–90.59. Schmulson M, Adeyemo M, Gutierrez-Reyes G, et al. Differences in gastrointestinal<strong>symptoms</strong> according to genderin Rome II positive IBS <strong>and</strong> dyspepsiain a Latin American population. Am JGastroenterol 2010; 105: 925–32.60. Ringel Y, Williams RE, Kalilani L, CookSF. Prevalence, characteristics, <strong>and</strong>impact of bloating <strong>symptoms</strong> inpatients with <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Clin Gastroenterol Hepatol 2009; 7: 68–72.61. L<strong>and</strong>is JR, Koch GG. A review of statisticalmethods in the analysis of data arisingfrom observer reliability studies, Parts I<strong>and</strong> II. Stat Neerl 1975; 29: 101–23.62. Hinds JP, Stoney B, Wald A. Does genderor the <strong>men</strong>strual cycle affect colonictransit? Am J Gastroenterol 1989; 84:123–6.63. Altman G, Cain KC, Motzer S, JarrettM, Burr R, Heitkemper M. Increased<strong>symptoms</strong> in female IBS patients withdys<strong>men</strong>orrhea <strong>and</strong> PMS. GastroenterolNurs 2006; 29: 4–11.64. Hungin AP, Chang L, Locke GR, DennisEH, Barghout V. Irritable <strong>bowel</strong><strong>syndrome</strong> in the United States: prevalence,symptom patterns <strong>and</strong> impact.Ali<strong>men</strong>t Pharmacol Ther 2005; 21:1365–75.65. Ford AC, Forman D, Bailey AG, AxonAT, Moayyedi P. Irritable <strong>bowel</strong> <strong>syndrome</strong>:a 10-yr natural history of <strong>symptoms</strong><strong>and</strong> factors that influenceconsultation behavior. Am J Gastroenterol2007; 102: 1–11.66. Neal KR, Hebden J, Spiller R. Prevalenceof gastrointestinal <strong>symptoms</strong> sixmonths after bacterial gastroenteritis<strong>and</strong> risk factors for develop<strong>men</strong>t of the<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>: postal surveyof patients. BMJ 1997; 314: 779–82.67. Andrews EB, Eaton SC, Hollis KA, et al.Prevalence <strong>and</strong> demographics of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>: results from alarge web-based survey. Ali<strong>men</strong>t PharmacolTher 2005; 22: 935–42.68. Thompson WG, Irvine EJ, Pare P, FerrazziS, Rance L. Functional gastrointestinaldisorders in Canada: firstpopulation-based survey using Rome IIcriteria with suggestions for improvingthe questionnaire. Dig Dis Sci 2002; 47:225–35.69. Sperber AD, Friger M, Shvartzman P,et al. Rates of functional <strong>bowel</strong> disordersamong Israeli Be<strong>do</strong>uins in ruralareas compared with those who movedto permanent towns. Clin GastroenterolHepatol 2005; 3: 342–8.70. Coffin B, Dapoigny M, Cloarec D,Comet D, Dyard F. Relationship<strong>between</strong> severity of <strong>symptoms</strong> <strong>and</strong> qualityof life in 858 patients with <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>. Gastroenterol Clin Biol2004; 28: 11–5.71. Van der Horst VG, Holstege G. Sensory<strong>and</strong> motor components of reproductivebehavior: pathways <strong>and</strong> plasticity. BehavBrain Res 1998; 92: 157–67.72. van der Horst HE, van Dul<strong>men</strong> AM,Schellevis FG, van Eijk JT, Fennis JF,Bleijenberg G. Do patients with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> in primarycare really differ from outpatients with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>? Gut 1997;41: 669–74.73. Simren M, Abrahamsson H, Svedlund J,Bjornsson ES. Quality of life in patientswith <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> seen inreferral centers versus primary care: theimpact of gender <strong>and</strong> pre<strong>do</strong>minant<strong>bowel</strong> pattern. Sc<strong>and</strong> J Gastroenterol2001; 36: 545–52.Ali<strong>men</strong>t Pharmacol Ther 17ª 2010 Blackwell Publishing Ltd
M. A. Adeyemo et al.74. Gwee KA, Wee S, Wong ML, Png DJ.The prevalence, symptom characteristics,<strong>and</strong> impact of <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>in an Asian urban community.Am J Gastroenterol 2004; 99: 924–31.75. Xiong LS, Chen MH, Chen HX, XuAG, Wang WA, Hu PJ. A populationbasedepidemiologic study of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> in South China: stratifiedran<strong>do</strong>mized study by cluster sampling.Ali<strong>men</strong>t Pharmacol Ther 2004;19: 1217–24.76. Lu CL, Chen CY, Lang HC, et al. Currentpatterns of <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>in Taiwan: The Rome II questionnaireon a Chinese population. Ali<strong>men</strong>t PharmacolTher 2003; 17: 217–24.77. Drossman DA, Weinl<strong>and</strong> SR. Com<strong>men</strong>tary:sociocultural factors in medicine<strong>and</strong> gastrointestinal research. Eur J GastroenterolHepatol 2008; 20: 593–5.78. Jain AP, Gupta OP, Jajoo UN, SidhwaHK. Clinical profile of <strong>irritable</strong> <strong>bowel</strong><strong>syndrome</strong> at a rural based teaching hospitalin central India. J Assoc PhysiciansIndia 1991; 39: 385–6.79. Pimparkar BD. Irritable colon <strong>syndrome</strong>.J Indian Med Assoc 1970; 54:95–103.80. Ragnarsson G, Hallbook O, Bodemar G.Ab<strong>do</strong>minal <strong>symptoms</strong> are not related toanorectal function in the <strong>irritable</strong> <strong>bowel</strong><strong>syndrome</strong>. Sc<strong>and</strong> J Gastroenterol 1999;34: 250–8.81. Chang L, Naliboff BD, Labus JS, et al.Effect of sex on perception of rectosigmoidstimuli in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Am J Physiol Regul Integr CompPhysiol 2006; 291: R277–84.82. Jun DW, Park HY, Lee OY, et al. Apopulation-based study on <strong>bowel</strong> habitsin a Korean community: prevalence offunctional constipation <strong>and</strong> self-reportedconstipation. Dig Dis Sci 2006; 51:1471–7.83. Katsinelos P, Lazaraki G, Kountouras J,et al. Prevalence, <strong>bowel</strong> habit subtypes<strong>and</strong> medical care-seeking behaviour ofpatients with <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>in Northern Greece. Eur J GastroenterolHepatol 2009; 21: 183–9.84. Pare P, Ferrazzi S, Thompson WG,Irvine EJ, Rance L. An epidemiologicalsurvey of constipation in Canada: definitions,rates, demographics, <strong>and</strong> predictorsof health care seeking. Am JGastroenterol 2001; 96: 3130–7.85. Metcalf AM, Phillips SF, ZinsmeisterAR, MacCarty RL, Beart RW, WolffBG. Simplified assess<strong>men</strong>t of seg<strong>men</strong>talcolonic transit. Gastroenterology 1987;92: 40–7.86. Meier R, Beglinger C, Dederding JP,et al. Influence of age, gender, hormonalstatus <strong>and</strong> smoking habits oncolonic transit time. NeurogastroenterolMotil 1995; 7: 235–8.87. Lampe JW, Fredstrom SB, Slavin JC,Potter JD. Sex differences in colonicfunction: a ran<strong>do</strong>mised trial. Gut 1993;34: 531–6.88. Shih YC, Barghout VE, S<strong>and</strong>ler RS,et al. Resource utilization associatedwith <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> in theUnited States 1987–1997. Dig Dis Sci2002; 47: 1705–15.89. Jonsson B, Gardsell P, Johnell O, Redlund-JohnellI, Sernbo I. Rememberingfractures: fracture registration <strong>and</strong> prob<strong>and</strong>recall in southern Sweden. J EpidemiolCommunity Health 1994; 48:489–90.90. Naliboff BD, Berman S, Chang L, DerbyshireSWG, Suyenobu B, Vogt BA,M<strong>and</strong>elkern MA, Mayer EA. Sex-relateddifferences in IBS patients: centralprocessing of visceral stimuli.Gastroenterology 2003; 124:1738–47.91. Cremon C, Gargano L, Morselli-LabateAM, et al. Mucosal immune activationin <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>: genderdependence<strong>and</strong> association with digestive<strong>symptoms</strong>. Am J Gastroenterol2009; 104: 392–400.92. Levy RL, Olden KW, Naliboff BD, et al.Psychosocial aspects of the functionalgastrointestinal disorders. Gastroenterology2006; 130: 1447–58.93. Drossman DA, Talley NJ, Leserman J,Olden KW, Barreiro MA. Sexual <strong>and</strong>physical abuse <strong>and</strong> gastrointestinalillness. Review <strong>and</strong> recom<strong>men</strong>dations.Ann Intern Med 1995; 123: 782–94.94. Drossman DA, Li Z, Leserman J, ToomeyTC, Hu YJ. Health status by gastrointestinaldiagnosis <strong>and</strong> abusehistory. Gastroenterology 1996; 110:999–1007.95. Drossman DA, Leserman J, Li Z, KeefeF, Hu YJ, Toomey TC. Effects of copingon health outcome among wo<strong>men</strong> withgastrointestinal disorders. PsychosomMed 2000; 62: 309–17.96. Koloski NA, Talley NJ, Boyce PM. Predictorsof health care seeking for <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong> <strong>and</strong> nonulcerdyspepsia: a critical review of the literatureon symptom <strong>and</strong> psychosocial factors.Am J Gastroenterol 2001; 96:1340–9.97. Sperber AD, Shvartzman P, Friger M,Fich A. A comparative reappraisal ofthe Rome II <strong>and</strong> Rome III diagnosticcriteria: are we getting closer to the‘true’ prevalence of <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>?Eur J Gastroenterol Hepatol2007; 19: 441–7.98. Saito YA, Locke GR, Talley NJ,Zinsmeister AR, Fett SL, Melton LJ 3rd.A comparison of the Rome <strong>and</strong> Manningcriteria for case identification inepidemiological investigations of <strong>irritable</strong><strong>bowel</strong> <strong>syndrome</strong>. Am J Gastroenterol2000; 95: 2816–24.99. Heitkemper M, Chang L Do fluctuationsin ovarian hormones affect gastrointestinal<strong>symptoms</strong> in wo<strong>men</strong> with<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>? Gend Med2009; 6: 152–67.100. Laessle RG, Tuschl RJ, Schweiger U,Pirke KM. Mood changes <strong>and</strong> physicalcomplaints during the normal <strong>men</strong>strualcycle in healthy young wo<strong>men</strong>.Psychoneuroen<strong>do</strong>crinology 1990; 15:131–8.101. Li TJ, Yu BP, Dong WG, Luo HS, XuL, Li MQ. Ovarian hormone modulates5-hydroxytryptamine 3 receptorsmRNA expression in rat colon withrestraint stress-induced <strong>bowel</strong> dysfunction.World J Gastroenterol 2004; 10:2723–6.102. Houghton LA, Perry H, Morris J,Whorwell PJ, Keevil B. Plasma 5-hydroxytryptamine concentration varieswith gender <strong>and</strong> <strong>men</strong>strual status in<strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong> patients withdiarrhoea (IBS-D) but not healthy volunteers.Gastroenterology 2008; 134: A-681.103. Barbara G, Stanghellini V, De GiorgioR, et al. Activated mast cells in proximityto colonic nerves correlate withab<strong>do</strong>minal pain in <strong>irritable</strong> <strong>bowel</strong> <strong>syndrome</strong>.Gastroenterology 2004; 126:693–702.104. Vasiadi M, Kempuraj D, Boucher W,Kalogeromitros D, Theoharides TC.Progesterone inhibits mast cell secretion.Int J Immunopathol Pharmacol2006; 19: 787–94.105. Koren G, Maltepe C, Navioz Y, WolpinJ. Recall bias of the <strong>symptoms</strong> of nausea<strong>and</strong> vomiting of pregnancy. Am J ObstetGynecol 2004; 190: 485–8.106. Sherman JJ, LeResche L. Does experi<strong>men</strong>talpain response <strong>vary</strong> across the<strong>men</strong>strual cycle? A metho<strong>do</strong>logicalreview. Am J Physiol Regul Integr CompPhysiol 2006; 291: R245–56.107. Lagiou P, Tamimi R, Mucci LA, TrichopoulosD, Adami HO, Hsieh CC. Nausea<strong>and</strong> vomiting in pregnancy inrelation to prolactin, estrogens, <strong>and</strong> progesterone:a prospective study. ObstetGynecol 2003; 101: 639–44.108. Fujii Y. Postoperative nausea <strong>and</strong> vomiting<strong>and</strong> their sex differences. Masui2009; 58: 59–66.109. Br<strong>and</strong>es JM. First-trimester nausea <strong>and</strong>vomiting as related to outcome ofpregnancy. Obstet Gynecol 1967; 30:427–31.110. Klebanoff MA, Koslowe PA, Kaslow R,Rhoads GG. Epidemiology of vomitingin early pregnancy. Obstet Gynecol 1985;66: 612–6.18 Ali<strong>men</strong>t Pharmacol Therª 2010 Blackwell Publishing Ltd