AFFERENT AND EFFERENT ARTERIOLAR RESISTANCES ...
AFFERENT AND EFFERENT ARTERIOLAR RESISTANCES ...
AFFERENT AND EFFERENT ARTERIOLAR RESISTANCES ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
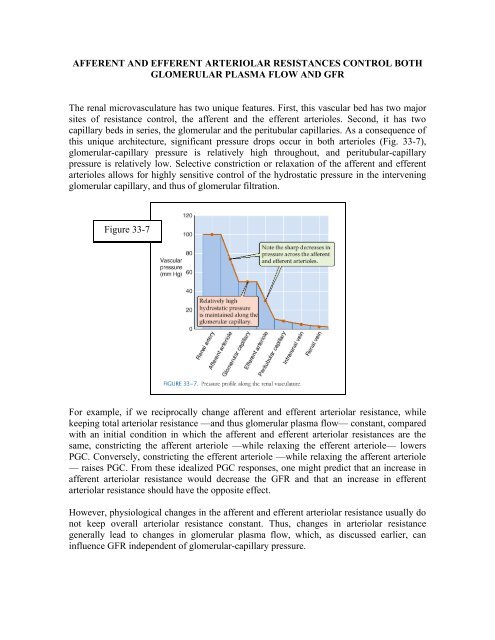
<strong>AFFERENT</strong> <strong>AND</strong> <strong>EFFERENT</strong> <strong>ARTERIOLAR</strong> <strong>RESISTANCES</strong> CONTROL BOTHGLOMERULAR PLASMA FLOW <strong>AND</strong> GFRThe renal microvasculature has two unique features. First, this vascular bed has two majorsites of resistance control, the afferent and the efferent arterioles. Second, it has twocapillary beds in series, the glomerular and the peritubular capillaries. As a consequence ofthis unique architecture, significant pressure drops occur in both arterioles (Fig. 33-7),glomerular-capillary pressure is relatively high throughout, and peritubular-capillarypressure is relatively low. Selective constriction or relaxation of the afferent and efferentarterioles allows for highly sensitive control of the hydrostatic pressure in the interveningglomerular capillary, and thus of glomerular filtration.Figure 33-7For example, if we reciprocally change afferent and efferent arteriolar resistance, whilekeeping total arteriolar resistance —and thus glomerular plasma flow— constant, comparedwith an initial condition in which the afferent and efferent arteriolar resistances are thesame, constricting the afferent arteriole —while relaxing the efferent arteriole— lowersPGC. Conversely, constricting the efferent arteriole —while relaxing the afferent arteriole— raises PGC. From these idealized PGC responses, one might predict that an increase inafferent arteriolar resistance would decrease the GFR and that an increase in efferentarteriolar resistance should have the opposite effect.However, physiological changes in the afferent and efferent arteriolar resistance usually donot keep overall arteriolar resistance constant. Thus, changes in arteriolar resistancegenerally lead to changes in glomerular plasma flow, which, as discussed earlier, caninfluence GFR independent of glomerular-capillary pressure.
There are more realistic effects on RPF and GFR as we change the resistance of a singlearteriole. With a selective increase of afferent arteriolar resistance, both capillary pressureand RPF decrease, leading to a monotonic decline in the GFR. In contrast, a selectiveincrease of efferent arteriolar resistance causes a steep increase in glomerular capillarypressure but also a decrease in RPF. As a result, over the lower range of resistances, GFRincreases with efferent resistance as an increasing PGC dominates. On the other hand, athigher resistances, GFR begins to fall as the effect of a declining RPF dominates. Theseopposing effects on glomerular capillary pressure and RPF account for the biphasicdependence of GFR on efferent resistance.During sympathetic stimulation, or in response to angiotensin II, both afferent and efferentresistances increase. Thus, RPF decreases. The generally opposing effects on GFR ofincreasing both afferent resistance and efferent resistance explain why the combination ofboth keeps GFR fairly constant despite a decline in RPF. There are realistic cases in whichchanges in either the afferent or the efferent arteriolar resistance dominates.A striking case in which a decrease in afferent arteriolar resistance dominates is the largeincrease in RPF that occurs with the loss of renal tissue, as after a nephrectomy in a kidneydonor. GFR in the remnant kidney nearly doubles, owing primarily to a dramatic decreasein the resistance of the afferent arteriole.An example of a predominantly efferent arteriolar effect is seen after administration ofangiotensin II inhibitors (e.g., captopril) to patients with hypertension that is due toincreased endogenous angiotensin levels. Administering such agents not only decreasesblood pressure, but also often leads to a significant fall in GFR. If we imagine that theresultant peak of the GFR curve represents a patient before treatment, then reducing theresistance of the efferent arteriole would indeed cause GFR to decrease.