Anemia in Heart Failure: Pathophysiology, Pathogenesis, Treatment ...
Anemia in Heart Failure: Pathophysiology, Pathogenesis, Treatment ...
Anemia in Heart Failure: Pathophysiology, Pathogenesis, Treatment ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
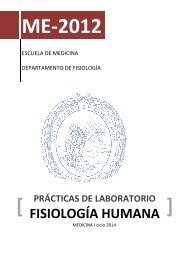
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>Inflammatory StimulusSerumAmyloid AIL-6 Pro<strong>in</strong>flammatory Cytok<strong>in</strong>esCRP↓ Availability of Ironfor ErythropoiesisPattern of Chronic<strong>Anemia</strong>Hepcid<strong>in</strong>↓ Intest<strong>in</strong>al Iron Absorption↓ Mobilization Iron↑ Cell Entrapment-Macrophages, Hepatocytes↓ Transferr<strong>in</strong> SaturationFigure 2. Inflammatory mechanisms <strong>in</strong> chronic anemia: critical role of<strong>in</strong>terleuk<strong>in</strong> 6 (IL-6) and hepcid<strong>in</strong>.CRP <strong>in</strong>dicates C-reactive prote<strong>in</strong>.defense aga<strong>in</strong>st microorganisms. As iron is not released<strong>in</strong>to the circulation, the availability to erythroid precursorsis reduced. 34,35 High hepcid<strong>in</strong> concentrations cause cellulariron overload, as occurs <strong>in</strong> hemochromatosis, andcontribute to the typical pattern of chronic anemia. Todate, there is no data on the hepcid<strong>in</strong> levels <strong>in</strong> HF patients,but the recent <strong>in</strong>troduction of commercially availablemethods for its measurement <strong>in</strong>dicates that <strong>in</strong>formationwill be made available <strong>in</strong> the near future. At the presenttime, there are no drug <strong>in</strong>terventions applicable tohepcid<strong>in</strong>.DrugsThe pathogenesis of anemia <strong>in</strong> HF also <strong>in</strong>volvesdifferent groups of drugs. Among the most importantones, because of their widespread utilization, are theangiotens<strong>in</strong>-convert<strong>in</strong>g enzyme (ACE) <strong>in</strong>hibitors and theangiotens<strong>in</strong> II receptor antagonists (angiotens<strong>in</strong> receptorblockers [ARB]).A number of studies have suggested that ACE <strong>in</strong>hibitors<strong>in</strong>duce or worsen anemia. In the Studies of Left VentricularDysfunction (SOLVD), which <strong>in</strong>volved 6000 patients, itwas observed that, although treatment with enalapril hada protective effect <strong>in</strong> terms of overall mortality, it wasassociated with a decrease <strong>in</strong> hematocrit and an <strong>in</strong>crease<strong>in</strong> the risk of new-onset anemia. Strik<strong>in</strong>gly, <strong>in</strong> this study,the overall mortality rate was 108% higher <strong>in</strong> the patientswho developed new-onset anemia. In contrast, <strong>in</strong> a Spanishseries <strong>in</strong>volv<strong>in</strong>g the prospective follow-up of 337 patientswho had been admitted to the hospital for HF over a20-month period, the relationship between ACE <strong>in</strong>hibitorsand anemia did not reach statistical significance. 37 Otherauthors have reported a decrease <strong>in</strong> the circulat<strong>in</strong>g EPO<strong>in</strong> patients treated with ACE <strong>in</strong>hibitors. 38-40The pharmacological <strong>in</strong>hibition of the RAAS canproduce a decrease <strong>in</strong> the hematocrit, which is negligible<strong>in</strong> patients with normal renal function, 41 but more marked<strong>in</strong> <strong>in</strong>dividuals with CRD. 42 While angiotens<strong>in</strong> I (AT1)antagonists 17 produce effects similar to those of the ACE<strong>in</strong>hibitors, 43 there are no formal studies compar<strong>in</strong>g thelatter with ARB <strong>in</strong> the anemia of HF.The decrease <strong>in</strong> hematocrit as a consequence of theuse of ACE <strong>in</strong>hibitors reaches its nadir <strong>in</strong> the first 3 monthsof treatment, but the level tends to rema<strong>in</strong> stable over thelong term. The discont<strong>in</strong>uation of these drugs leads tothe normalization of the hematocrit with<strong>in</strong> 3 to 4 months.Table 2 shows the possible mechanisms by which block<strong>in</strong>gthe RAAS can produce anemia.Prostagland<strong>in</strong>s have a stimulatory effect onerythropoiesis; thus, the adm<strong>in</strong>istration of nonsteroidalanti<strong>in</strong>flammatory drugs can pave the way for anemiathrough events other than the chronic blood loss alsocaused by these drugs. Once aga<strong>in</strong>, there are no studiesspecifically focus<strong>in</strong>g on this aspect, and one relevantissue is the possible role of aspir<strong>in</strong> <strong>in</strong> promot<strong>in</strong>g anemia,a question that could be addressed without undertak<strong>in</strong>gnew specific studies, by process<strong>in</strong>g the data of the exist<strong>in</strong>glarge series or by metaanalysis.HOW DOES ANEMIA INFLUENCETHE PROGNOSIS OF HEART FAILURE?In patients with HF, anemia is a risk factor formortality, 10 hospital admission, and severity, 7,29 anddoubles the risk associated with other factors, such asdiabetes mellitus, age, smok<strong>in</strong>g, and a low ejectionfraction. 44 In HF, there a l<strong>in</strong>ear relationship between themortality 6 and the hemoglob<strong>in</strong>/hematocrit levels. 45A number of authors report specific values for the <strong>in</strong>crease<strong>in</strong> risk of death or of a major event, <strong>in</strong>clud<strong>in</strong>g hospitaladmission, for each decrease of 1% <strong>in</strong> hematocrit. 13,44Others 46-49 affirm that an <strong>in</strong>crease <strong>in</strong> hemoglob<strong>in</strong> of1 g/dL reduces the risk of death at 1 year by 40%, witha decrease <strong>in</strong> the risk of hospital admission for HF of21%. These data constitute a solid argument for thetreatment of anemia <strong>in</strong> HF. However, they are not sufficientto enable us to establish the optimal hemoglob<strong>in</strong> level toachieve the maximum benefit with the least possibleTABLE 2. Possible <strong>Anemia</strong>-Induc<strong>in</strong>g Mechanismsof Angiotens<strong>in</strong>-Convert<strong>in</strong>g Enzyme Antagonistsand Angiotens<strong>in</strong> I Antagonists*RenalDecrease <strong>in</strong> the synthesis of endogenous EPOBone marrowDecrease <strong>in</strong> the response to EPOInhibition of the growth of erythroid precursorsChange <strong>in</strong> the response to treatment with rHuEPODecrease <strong>in</strong> IGF-1 levelsInhibition of the catabolism of N-acetyl-seryl-aspartyl-prol<strong>in</strong>e,a peptide that reduces the proliferation of precursorsof the red cell series*EPO <strong>in</strong>dicates erythropoiet<strong>in</strong>; IGF-1, <strong>in</strong>sul<strong>in</strong>-like growth factor 1; rHuEPO,recomb<strong>in</strong>ant human erythropoiet<strong>in</strong>.852 Rev Esp Cardiol. 2007;60(8):848-60
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>complications. An <strong>in</strong>terest<strong>in</strong>g question is the fact that thedecrease <strong>in</strong> hematocrit could be a marker for other factorsthat <strong>in</strong>crease the mortality <strong>in</strong> patients with severe HF, forexample, CRD. 44MECHANISMS BY WHICH ANEMIA CANINCREASE THE MORBIDITY AND MORTALITYIN HEART FAILUREAga<strong>in</strong>, we are faced by the lack of sufficient scientificevidence. Lower hemoglob<strong>in</strong> concentrations are associatedwith a poorer hemodynamic function, <strong>in</strong>creases <strong>in</strong> serumurea nitrogen and creat<strong>in</strong><strong>in</strong>e, decreases <strong>in</strong> album<strong>in</strong>,cholesterol and body mass <strong>in</strong>dex, a worse functionalclass, and a lower VO 2(peak oxygen consumption). 6,10,13A relationship between anemia and a less favorable coursehas been reported <strong>in</strong> patients with CRD, 50 asymptomaticleft ventricular dysfunction, 45 and advanced HF. 7,13 Thereare not sufficient data <strong>in</strong> cases of severe systolicdysfunction.In patients with preserved ventricular function, thehyperdynamic state can play a role <strong>in</strong> ventricularhypertrophy, which, <strong>in</strong> turn, can promote a disproportionbetween the oxygen supply to the myocardium and the<strong>in</strong>creased ventricular mass, a circumstance that is critical<strong>in</strong> the presence of significant coronary artery disease.Cardiac output has been found to be sharply <strong>in</strong>creased,with hemoglob<strong>in</strong> < 10 mg/dL (hematocrit < 30%-33%). 44In the Prospective Randomized Amlodip<strong>in</strong>e SurvivalEvaluation (PRAISE), anemia is associated with deathdue to pump failure. Studies carried out <strong>in</strong> animals showthat an ischemic or hypertrophic heart is more vulnerableto slight decreases <strong>in</strong> hemoglob<strong>in</strong> than a normal heart,with a marked deterioration <strong>in</strong> the ischemia and themyocardial dysfunction. Under these conditions, thetreatment with EPO is even more <strong>in</strong>terest<strong>in</strong>g because ofits cytoprotective properties with respect to themyocardium. 9,51,52In a recent review, Roig po<strong>in</strong>ted out that anemia couldpr<strong>in</strong>cipally be a marker of advanced disease, s<strong>in</strong>ce it isassociated above all with a worse functional class, andthat its correction improves the symptoms, but notnecessarily the mortality rate. 11 On the other hand, it hasbeen shown that hemoglob<strong>in</strong> is, <strong>in</strong> itself, an <strong>in</strong>dependentpredictive factor of mortality <strong>in</strong> HF, <strong>in</strong> both anemic andpolycythemic <strong>in</strong>dividuals. 53 Even more important, thehematocrit range that we should consider as excessive<strong>in</strong> patients with HF and, <strong>in</strong> particular with ischemic heartdisease, has yet to be clearly established.In HF, anemia also <strong>in</strong>fluences hospital admissions, anda relationship between the hemoglob<strong>in</strong> levels and thenumber of admissions due to HF over the preced<strong>in</strong>g yearhas been observed; <strong>in</strong> this respect, low hematocrit maybe more of a risk factor for hospital admission than formortality. 47-49<strong>Anemia</strong> can favor the progression of CRD <strong>in</strong> patientswith HF 38 and be, <strong>in</strong> itself, a risk factor 50 and a predictorfor the development of HF <strong>in</strong> patients with end-stageCRD. 44 In turn, renal function, together with the ejectionfraction and the NYHA class, may be an <strong>in</strong>direct markerof cardiac function. 25,26 F<strong>in</strong>ally, anemia (hemoglob<strong>in</strong>< 13 g/dL is an <strong>in</strong>dependent predictor of the exercisecapacity <strong>in</strong> HF, whereas <strong>in</strong> patients with hemoglob<strong>in</strong> >13g/dL, there is no correlation between VO 2andhemoglob<strong>in</strong>. 54Cellular and Molecular Biologyof Erythropoiet<strong>in</strong> Production: Hypoxia,Transcription Factors, and Other RegulatoryStimuliErythropoiesisProduction characteristics, site, and stimuli. Theproduction and action of EPO are the critical po<strong>in</strong>ts oferythropoiesis. Erythropoiet<strong>in</strong> is a glycoprote<strong>in</strong> that, <strong>in</strong>extrauter<strong>in</strong>e life, is produced nearly exclusively <strong>in</strong> theperitubular fibroblasts of the renal cortex, without directcontact with the capillaries and tubular cells. 55,56 The EPOgene belongs to a set of hypoxia-sensitive genes that areoverexpressed when there is a decrease <strong>in</strong> the cellularpartial pressure of oxygen (pO 2). 57 The production ofEPO exhibits circadian fluctuations and the kidney<strong>in</strong>tervenes <strong>in</strong> its catabolism. Hypoxia can lead to a severalhundred-fold <strong>in</strong>crease <strong>in</strong> EPO. In the experimental sett<strong>in</strong>g,the <strong>in</strong>crease <strong>in</strong> the <strong>in</strong>tensity of hypoxia is accompaniedby an exponential <strong>in</strong>crease <strong>in</strong> the number of fibroblastsexpress<strong>in</strong>g the EPO gene. 58 There are no data concern<strong>in</strong>gthis f<strong>in</strong>d<strong>in</strong>g <strong>in</strong> models of HF.Why <strong>in</strong> the kidneys? The possible physiological reasonsand consequences of the localization of EPO production<strong>in</strong> the kidney is a question that has not been fully resolved.The simple fact that blood is made up of red cells andplasma provides a clue: what the organism regulates isthe proportion of plasma that is constituted by circulat<strong>in</strong>gred cells (hematocrit). The specific mechanisms of thiscoord<strong>in</strong>ation are relatively unknown, although we assumethat there is an <strong>in</strong>trarenal connection between the pathwaysthat monitor and regulate the fluid volume and those thatcontrol the erythroid cell volume. 56 In other words, thecapacity of the kidney to detect the status of theextracellular volume (ECV) and produce EPO enablesit to “create” a normal hematocrit level. This phenomenonmay be of importance <strong>in</strong> HF, <strong>in</strong> which the accumulationof extracellular fluid and hemodilution can change the“perception” of the hematocrit on the part of the kidney.On the other hand, the kidney extracts only a small partof the oxygen delivered to it, a circumstance that makesit possible to detect slight changes <strong>in</strong> oxygenation.Moreover, the constancy of the ratio of the work performed(oxygen consumption) to the renal blood flow (oxygendelivery) makes it possible to separate the renal pO 2fromthe metabolic activity, mean<strong>in</strong>g that the regulation ofRev Esp Cardiol. 2007;60(8):848-60 853
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>EPO synthesis can be reasonably, although not totally,<strong>in</strong>dependent of the reabsorptive activity.Basel<strong>in</strong>e hematopoietic stimulation orig<strong>in</strong>ates <strong>in</strong> thephysiological destruction of red blood cells, but itsgreatest <strong>in</strong>tensity is observed <strong>in</strong> hemorrhage. <strong>Anemia</strong>of HF is usually mild, persistent and adaptive. Thus,its effects would be analogous to m<strong>in</strong>or hemorrhagewith limited, but long-term, hemodynamic impact. Thekidney has to restore volume depend<strong>in</strong>g on the amountof fluid lost and produce red cells to replace those lost,but noth<strong>in</strong>g more. Moreover, it has to be able to discernthe proportion <strong>in</strong> which fluid is conserved and new redcells are produced. The jo<strong>in</strong>t regulation of these 2mechanisms is more complex than that of eachseparately, and is 1 of the keys to research <strong>in</strong> a diseaselike HF.What makes up the cha<strong>in</strong> of signals and mechanismsthat <strong>in</strong>crease endogenous erythropoiet<strong>in</strong>? Thephysiological sequence <strong>in</strong>volved <strong>in</strong> the stimulation ofEPO production is based on 2 transcription factors thatcan be activated by hypoxia, hypoxia-<strong>in</strong>ducible factors 1,and 2 (HIF-1 and HIF-2). 59,60 Hypoxia-<strong>in</strong>ducible factor1 is a molecule that regulates an overall multigenicresponse, rather than isolated effects. The great advance<strong>in</strong> recent years has been the discovery that transcriptionallyactive HIF-1 depends on a group of non-heme-irondependentprolyl hydroxylases that constitute the trueoxygen-sens<strong>in</strong>g mechanism. 59,61 . In contrast, HIF-2appears to play a selective role <strong>in</strong> EPO expression, whichis practically abolished <strong>in</strong> the knockouts for this gene. 61,62The activation state of HIF <strong>in</strong> HF is unknown, andthere are no data published concern<strong>in</strong>g its measurement.Thus, references to its role are limited to supposition,firm, but still conjectural. Although the patient with HFcan go through periods of systemic hypoxia, they areusually transient; brief hypoxia does not constitute astrong enough stimulus for susta<strong>in</strong>ed EPO <strong>in</strong>duction. 57On the other hand, the measurement of tissue oxygenationis a challenge that has yet to be resolved by cl<strong>in</strong>icalresearch and the tissue oxygen levels reached dur<strong>in</strong>gperiods of decompensation and compensation <strong>in</strong> HF arebasically unknown.Hypoxia-<strong>in</strong>ducible factor 1 is activated by means ofphosphorylation under hypoxic conditions. It acts bytransactivat<strong>in</strong>g more than 70 genes, at least 4 of whichare highly relevant to the f<strong>in</strong>al effect of EPO: the transferr<strong>in</strong>gene, supply<strong>in</strong>g iron to the erythroid cells; the vascularendothelial growth factor (VEGF) gene, a cofactor <strong>in</strong> thestimulation of these same cells and a determ<strong>in</strong><strong>in</strong>g element<strong>in</strong> angiogenesis and tissue perfusion; the tyros<strong>in</strong>ehydroxylase gene, <strong>in</strong>volved <strong>in</strong> dopam<strong>in</strong>e synthesis andrespiratory regulation; and the nitric oxide synthase gene,which ma<strong>in</strong>ta<strong>in</strong>s normal arterial blood pressure underthe potentially pressor effect of EPO. 63Hypoxia-<strong>in</strong>ducible factor 1 is activated at oxygenconcentrations of around 4% to 5% (saturation of 30 to35 mm Hg). 64 The presence of elevated EPO levels <strong>in</strong>patients with HF can be taken as an <strong>in</strong>direct sign of HIFstimulation, but, as yet, there is no direct scientificevidence <strong>in</strong> this respect.Hemodynamics and Erythropoiet<strong>in</strong>The blood flow rate <strong>in</strong> the kidneys is elevated(approximately 20% of the cardiac output). In the renalmedulla, the pO 2is permanently under 10 mm Hg,whereas <strong>in</strong> the cortex, it is more variable, with a meanclose to the threshold for HIF stimulation (30 mm Hg).Changes <strong>in</strong> these concentrations are determ<strong>in</strong>ant <strong>in</strong><strong>in</strong>duction of the EPO gene. 65 Thus, it is assumed that, <strong>in</strong>patients with more severe HF (NYHA functional classIII-IV), s<strong>in</strong>ce the renal flow rate is reduced, the decreasedperitubular oxygen tension would be the ma<strong>in</strong> stimulusto trigger EPO production. 17 Other studies po<strong>in</strong>t out theassociation between EPO synthesis <strong>in</strong> HF and renalhemodynamic dysfunction, although no correlationbetween plasma EPO levels and arterial pO 2, oxygensaturation, or glomerular filtration has been found. 66Role of Angiotens<strong>in</strong> IIIn HF, the low renal output stimulates ren<strong>in</strong> production,and this, <strong>in</strong> turn, that of angiotens<strong>in</strong> II (Ang II). A higherAng II level results <strong>in</strong> greater sodium reabsorption and,thus, an <strong>in</strong>creased adenos<strong>in</strong>e triphosphate and oxygenconsumption, secondary to the <strong>in</strong>creased tubularreabsorptive function. In healthy subjects, the EPOconcentrations are correlated with the proximal tubularsodium reabsorption rate. 67 Diuretics that act on Henle’sloop, the distal tubule and collect<strong>in</strong>g duct (furosemide,hydrochlorothiazide, and amiloride, respectively) do notaffect EPO formation. In contrast, acetazolamide, whichacts on the proximal tubule, significantly decreases EPOproduction <strong>in</strong> response to normobaric hypoxia andfunctional anemia. 67These data are consistent with the simultaneity of the<strong>in</strong>crease <strong>in</strong> EPO levels and the poorer prognosis of HF. 68Thus, if proximal hyperreabsorption is proportional tothe degree of decompensation <strong>in</strong> HF, it can be assumedthat those patients who are decompensated will reabsorbmore sodium and will produce more EPO. To date, studiesaddress<strong>in</strong>g this assumption have not been performed <strong>in</strong>humans.One relevant question is whether the changes observed<strong>in</strong> Ang II are due to a direct stimulation of the peritubularfibroblasts that synthesize EPO or to hemodynamic effects<strong>in</strong>duced by Ang II. In vitro, <strong>in</strong> HepG2 tumor cells, whichexpress AT1 receptors, Ang II, and the AT1 antagonist,losartan, have no effects on EPO production, acircumstance that supports the idea that the <strong>in</strong> vivo effectsof Ang II are ma<strong>in</strong>ly due to hemodynamic changes. 69However, there are data that <strong>in</strong>dicate that Ang II is capableof activat<strong>in</strong>g HIF-1α to levels even higher than those854 Rev Esp Cardiol. 2007;60(8):848-60
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>generated by hypoxia. 70 The adm<strong>in</strong>istration of exogenousAng II, which <strong>in</strong>creases HIF-1 and its target gene, VEGF,also <strong>in</strong>creases the EPO concentrations <strong>in</strong> a dose-dependentmanner. 71 Likewise, transgenic mice carry<strong>in</strong>g both humanren<strong>in</strong> and human angiotens<strong>in</strong>ogen have persistenterythrocytosis, via the AT1 receptor. 72 These results canbe expla<strong>in</strong>ed by f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> <strong>in</strong> vitro studies that establishthat Ang II not only plays a role <strong>in</strong> EPO production, butalso stimulates erythroid precursors by means of AT1activation <strong>in</strong> the erythroid burst-form<strong>in</strong>g units. 41 Despitethe fact that we have all this <strong>in</strong>formation, it can be saidthat, as a whole, the effect of Ang II on anemia has yetto be fully def<strong>in</strong>ed.Signal<strong>in</strong>g <strong>in</strong> Erythropoiet<strong>in</strong> ProductionThe regulation of EPO production is controlled by anenhancer that b<strong>in</strong>ds HIF-1 and, thus, is referred to asHRE (hypoxia responsive element). In addition, thereare elements that coregulate gene expression, theimportance of which is still not fully known, but thatmight expla<strong>in</strong> the differences <strong>in</strong> EPO mRNA synthesisobserved under conditions equivalent to hypoxia. Amongthem, we should mention two transcription factors, GATAand nuclear factor kappa beta (NFκβ), which negativelyregulate the expression of EPO mRNA. These 2 factorscan be <strong>in</strong>creased <strong>in</strong> the presence of <strong>in</strong>flammation, andthus, constitute plausible explanations for the decrease<strong>in</strong> EPO synthesis <strong>in</strong> <strong>in</strong>flammatory conditions. With respectto the stimulation of EPO gene expression, it should bementioned that there is an <strong>in</strong>verse relationship betweenGATA and nitric oxide, a circumstance that <strong>in</strong>dicates arole of the decrease <strong>in</strong> the latter <strong>in</strong> the reduced EPOproduction. 73Erythropoiet<strong>in</strong> Signal<strong>in</strong>g <strong>in</strong> its Target CellsErythropoiet<strong>in</strong> signals through a receptor with prote<strong>in</strong>k<strong>in</strong>ase activity, which mediates proliferative andantiapoptotic effects <strong>in</strong> the erythroid precursors. For theformer, EPO stimulates the Ras/mitogen-activated prote<strong>in</strong>k<strong>in</strong>ase (MAPK) pathway and, above all, the Janus k<strong>in</strong>ase2 (JAK2) pathway, which acts without <strong>in</strong>termediarymetabolites on transcription factors of the STAT (signaltransducer and activator of transcription) family, especiallySTAT5. The antiapoptotic effects can also employ theJAK2/STAT pathway, but the ma<strong>in</strong> enzymatic step occurs<strong>in</strong> phosphatidyl<strong>in</strong>ositol-3 k<strong>in</strong>ase. There are EPO receptors(EPO-R) <strong>in</strong> the erythroblasts, but they are also found <strong>in</strong>the placenta, heart, ret<strong>in</strong>a, bra<strong>in</strong>, and endothelial cells. 74The EPO-R is a transmembrane receptor that sharesproperties with the receptors of other hematopoieticfactors. While the <strong>in</strong>tracellular transduction of EPO isknown to take place, there are considerable gaps <strong>in</strong> ourknowledge with respect to how this hormone regulatesthe survival, proliferation and differentiation of erythroidprogenitor cells. 75The <strong>in</strong>hibitory effect of apoptosis does not only concernthe erythroblasts. In this respect, it has recently beendemonstrated that EPO is a potent trophic and apoptoticfactor, with protective effects <strong>in</strong> bra<strong>in</strong> and ret<strong>in</strong>al cells,<strong>in</strong> the renal epithelium and, as mentioned above, <strong>in</strong>myocardial cells, as well. 51Resistance to Erythropoiet<strong>in</strong>In studies that relate an <strong>in</strong>crease <strong>in</strong> EPO to a poorerprognosis <strong>in</strong> HF (severity and mortality), the patientswith elevated erythropoiet<strong>in</strong> levels are usually moreanemic. In the absence of bleed<strong>in</strong>g, this suggests peripheralresistance to the action of endogenous EPO. 68 Thecirculat<strong>in</strong>g EPO concentrations, as well as the severityof anemia, <strong>in</strong>crease <strong>in</strong> parallel with the NYHA functionalclass 38 and, thus, we should look for additional pathogenicelements to expla<strong>in</strong> the anemia.Other factors that have been implicated <strong>in</strong> thepathogenesis of resistance to EPO <strong>in</strong> HF are the mediationof cytok<strong>in</strong>es and generalized bone marrow dysfunction. 11,44The latter has been postulated on the basis of the decreasedleukocyte/lymphocyte counts <strong>in</strong> patients with HF andanemia, but its importance is marg<strong>in</strong>al.The causes for resistance to EPO <strong>in</strong> HF should bestudied <strong>in</strong> accordance with f<strong>in</strong>d<strong>in</strong>gs associated with otherdiseases (Table 3). There are no studies that systematicallyanalyze resistance to exogenous EPO <strong>in</strong> HF, a subjectthat requires a specific exam<strong>in</strong>ation.PHARMACOLOGICAL TREATMENTOF ANEMIA IN HEART FAILURETo date, there are no studies that systematically comparedifferent treatment regimens <strong>in</strong> the anemia of HF. Theresults of the survey that we mentioned above <strong>in</strong>dicatethat only a m<strong>in</strong>ority of cardiologists and <strong>in</strong>ternists employrecomb<strong>in</strong>ant erythropoiesis-stimulat<strong>in</strong>g agents (ESA)and <strong>in</strong>travenous iron. For this reason, we have based ourstudy on the experience accumulated <strong>in</strong> the nephrologysett<strong>in</strong>g, with over 15 years of cont<strong>in</strong>uous use of ESA,<strong>in</strong>travenous iron, and other supplements. The nephrologysocieties have at least 2 large practice guidel<strong>in</strong>es, theKidney Disease Outcome Quality Initiative (KDOQI) 76-78<strong>in</strong> the United States, and the European guidel<strong>in</strong>es,which provide a considerable body of knowledge, withaspects that are reasonably adaptable to the cardiologysett<strong>in</strong>g.Exist<strong>in</strong>g Erythropoiesis-Stimulat<strong>in</strong>g Agentsand Those Be<strong>in</strong>g DevelopedThe first generation of ESA <strong>in</strong>cluded recomb<strong>in</strong>antEPO-alpha (Epogen, Amgen; and Procrit/Eprex, Johnson& Johnson/Janssen-Cilag) and EPO-beta (NeoRecormon,Roche). The demand for longer-act<strong>in</strong>g ESA led to thedevelopment of darbepoet<strong>in</strong> (Aranesp, Amgen), aRev Esp Cardiol. 2007;60(8):848-60 855
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>hyperglycosylated derivative with a 3-fold longer halflife,thus mak<strong>in</strong>g it possible to adm<strong>in</strong>ister weekly,bimonthly, or even monthly <strong>in</strong>jections; the efficacy ofthe latter periodicity has been tested <strong>in</strong> HF patients. 80A pegylated derivative, a cont<strong>in</strong>uous erythropoiesis receptoractivator (CERA, Roche), with an even longer half-life, 52,81will soon be made commercially available. Other highly<strong>in</strong>terest<strong>in</strong>g products capable of <strong>in</strong>duc<strong>in</strong>g hematopoiesisare <strong>in</strong> an advanced state of development. These <strong>in</strong>cludethe synthetic EPO receptor agonist developed by Affymax,Hematide, a peptide that is not related to the compoundsutilized up to now and that has been shown to producelong-term erythroid <strong>in</strong>duction (1 month), with goodtolerance and stability at room temperature. F<strong>in</strong>ally,FibroGen is develop<strong>in</strong>g a new approach to the problemof anemia, which <strong>in</strong>volves the stabilization of HIF-1 bymeans of prolyl hydroxylase <strong>in</strong>hibitors of small molecularsize. In HF, the important potential advantages of agentsof this type do not lie solely <strong>in</strong> their oral adm<strong>in</strong>istration,but <strong>in</strong> the <strong>in</strong>duction not only of EPO, but of the multiplegenes <strong>in</strong>volved <strong>in</strong> the antianemic and hypoxic response. 52,81Recently, for the purpose of act<strong>in</strong>g exclusively on thetrophic effects (see below), EPO derivatives that have aweak action <strong>in</strong> erythroid precursors, but are potent <strong>in</strong>other cell types, are be<strong>in</strong>g developed.TREATMENT WITH ERYTHROPOIETININ HEART FAILURE PATIENTSAND ITS CONSEQUENCESThe critical po<strong>in</strong>ts of the treatment of anemia <strong>in</strong> HFare the pharmacological tools and the therapeutic target,that is, the po<strong>in</strong>t of optimal yield. While this target hasto be <strong>in</strong>dividualized, to date, there is not sufficientconsensus as to the optimal hemoglob<strong>in</strong> and hematocritvalues to be reached and ma<strong>in</strong>ta<strong>in</strong>ed. 6,7 There arehemoglob<strong>in</strong> levels that are not considered to be harmful<strong>in</strong> normal subjects, but are deleterious <strong>in</strong> HF. 6 It is alsonecessary to take <strong>in</strong>to account the fact that a rapid <strong>in</strong>crease<strong>in</strong> hematocrit or its <strong>in</strong>crease beyond normal levels worsensthe prognosis. Available studies <strong>in</strong>dicate that a hematocritvalue of around 35%-36% and a hemoglob<strong>in</strong> level ofapproximately 12 g/dL are safe. 7,9Among the beneficial effects of treatment with EPO, 7,11different authors po<strong>in</strong>t out that the correction of anemia<strong>in</strong>creases the ejection fraction, decreases left ventricularmass and improves the oxygen-carry<strong>in</strong>g capacity andoxygen utilization (peak consumption) dur<strong>in</strong>g exercise,thus lengthen<strong>in</strong>g its duration. 82 It also improves the NYHAclass and myocardial ischemia dur<strong>in</strong>g the stress test,stabilizes the creat<strong>in</strong><strong>in</strong>e levels, enables the reduction ofthe doses of diuretics and iron, and improves the qualityof life <strong>in</strong>dex. All these effects play a role <strong>in</strong> the reduction<strong>in</strong> the number and duration of hospital stays. 13,29,82 In astudy <strong>in</strong> which subcutaneous EPO and <strong>in</strong>travenous ironwere adm<strong>in</strong>istered to HF patients <strong>in</strong> NYHA functionclass III-IV with a hemoglob<strong>in</strong> level < 12 g/dL who hadTABLE 3. Common Causes of Resistanceto Erythropoiet<strong>in</strong>*Blood lossIron deficiency: absolute and relativeChronic renal disease: also provokes endogenous EPO deficiencyAcute and chronic <strong>in</strong>flammationAntagonist agents: ACE <strong>in</strong>hibitors, nonsteroidal anti<strong>in</strong>flammatorydrugsMalnutrition and deficiency of factors, such as vitam<strong>in</strong> B 12,folic acidBone marrow depression*ACE <strong>in</strong>dicates angiotens<strong>in</strong>-convert<strong>in</strong>g enzyme; EPO, erythropoiet<strong>in</strong>.not responded to conventional therapy, the correction ofanemia was associated with a marked improvement <strong>in</strong>cardiac function and a reduction <strong>in</strong> the number of hospitaladmissions and the use of diuretics. 9Of special <strong>in</strong>terest is the improvement <strong>in</strong> the exercisecapacity <strong>in</strong> patients with moderate-to-severe HF be<strong>in</strong>gtreated with EPO, with an <strong>in</strong>crease <strong>in</strong> the oxygen deliveryand a reduction <strong>in</strong> oxidative stress. 82 In patients withchronic HF, a functionally important relationship hasbeen reported between a hemoglob<strong>in</strong> < 13 g/dL andexercise capacity; it is highly <strong>in</strong>terest<strong>in</strong>g to observe thatthis relationship does not exist when the hemoglob<strong>in</strong> is> 13 g/dL. 54Some of the undesirable effects of EPO reported <strong>in</strong>the past, such as, for example, hypertension, thromboses,and pure red cell aplasia, have disappeared or have beenreduced to a m<strong>in</strong>imum. Despite its angiogenic effects, 74there are no consistent data that allow us to attribute aworsen<strong>in</strong>g of malignant tumors or diabetic ret<strong>in</strong>opathyto EPO.In the economic aspect, the cost of treatment with EPOand iron is lower than that of hospital readmission, 29 butthere are no specific studies on this question, and theyare necessary.THE PHARMACOLOGY OF ERYTHROPOIETINThe exist<strong>in</strong>g preparations can be adm<strong>in</strong>istered eithersubcutaneously or <strong>in</strong>travenously, although for practicalreasons, the former is preferred; discomfort at the <strong>in</strong>jectionsite is m<strong>in</strong>imal. It is essential to keep <strong>in</strong> m<strong>in</strong>d theimportance of ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g the cold cha<strong>in</strong> at 4 o C topreserve a high efficacy. 83The duration of the effect of EPO (up to 1 week) isshorter than that of darbepoet<strong>in</strong>, which lasts 15 to 30days, although the therapeutic yield is equivalent. The<strong>in</strong>dications for EPO, orig<strong>in</strong>ally limited to patients withCRD, are be<strong>in</strong>g extended to all the groups that mightbenefit, <strong>in</strong>clud<strong>in</strong>g patients with myelodysplastic syndromeor human immunodeficiency virus, premature <strong>in</strong>fantsand cancer patients undergo<strong>in</strong>g chemotherapy, as wellas <strong>in</strong> cases of sickle cell anemia, prior to autologous856 Rev Esp Cardiol. 2007;60(8):848-60
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>donation, as perioperative adjuvant therapy and <strong>in</strong> HF. 52In CRD, a condition <strong>in</strong> which the experience is moreextensive, the standard doses for <strong>in</strong>itial EPO therapy are400 U/kg bw/week and 15-200 U/kg bw/week,adm<strong>in</strong>istered <strong>in</strong>travenously and subcutaneously,respectively, divided <strong>in</strong>to 1 to 3 doses per week. 84However, there is less <strong>in</strong>formation on the doses to beadm<strong>in</strong>istered <strong>in</strong> HF. Thus, regimens similar to those tested<strong>in</strong> CRD are be<strong>in</strong>g used, and will have to be verified overthe course of time.IRON THERAPYSome authors susta<strong>in</strong> that it is practically obligatoryto add <strong>in</strong>travenous iron therapy to treatment with EPO 9,29to prevent possible iron deficiency secondary to the<strong>in</strong>crease <strong>in</strong> hematopoiesis. The additive effect of thecomb<strong>in</strong>ation of iron and EPO may not be achieved withoral iron. 85,86 However, there is a lack of data to enableus to predict which patients will fail to absorb oral iron,and it is to be hoped that hepcid<strong>in</strong> measurements willhelp to resolve this question. The exist<strong>in</strong>g <strong>in</strong>travenousiron preparations, iron gluconate (Ferrlecit, Rhone-Poulenc, 62.5 mg elemental iron), and iron sucrose(Venofer, Uriach, 100 mg elemental iron), have practicallyno collateral effects if used <strong>in</strong> reasonable doses, forexample, 1 vial a week, <strong>in</strong> cycles of 6 to 9 vials, depend<strong>in</strong>gon the ferrit<strong>in</strong> levels. These doses that we mention aremore conservative than others that have been employed,but they take <strong>in</strong>to account the possibility of <strong>in</strong>duction ofoxidative effects due to the adm<strong>in</strong>istration of largequantities of iron via a nonphysiological route, the<strong>in</strong>travenous route. As a comparative datum for dos<strong>in</strong>g, ablood transfusion supplies approximately 250 mg ofelemental iron, which eventually becomes part of theiron <strong>in</strong> the organism due to the gradual destruction of thetransfused red blood cells.On the other hand, certa<strong>in</strong> recent data <strong>in</strong>dicate that,at least <strong>in</strong> some patients, iron deficiency is the majorpathogenic factor <strong>in</strong> anemia. In these cases, adjuvanttreatment with EPO would not be necessary, as ispo<strong>in</strong>ted out <strong>in</strong> recent communications, whichdemonstrate improvements <strong>in</strong> anemia with iron therapyalone, 87 and <strong>in</strong> prelim<strong>in</strong>ary results from cl<strong>in</strong>ical studiespend<strong>in</strong>g publication or still underway, such as FERRIC-HF and IRON-HF. 88,89 The possible iron deficiency,absolute or relative, can become more marked due toother additional factors, such as losses secondary toantiplatelet/anticoagulant therapy and aspir<strong>in</strong>-<strong>in</strong>ducedgastritis. 7,10,20 Moreover, right HF can favor deficientabsorption or nutritional deficiencies <strong>in</strong>volv<strong>in</strong>g elementsnecessary for erythroid maturation, such as vitam<strong>in</strong>B 12and folic acid, and iron itself. 11 There are no recentstudies on the prevalence of vitam<strong>in</strong> deficiencies <strong>in</strong><strong>in</strong>dividuals with HF, but the current appraisal is thatthese pathogenic elements of anemia are of limitedimportance <strong>in</strong> this context.ERYTHROPOIETIN CAN IMPROVE HEARTFAILURE NOT ONLY BY CORRECTINGANEMIAErythropoiet<strong>in</strong> has cytoprotective effects on cardiacendothelium 74 and muscle. The EPO-R is present aboveall dur<strong>in</strong>g the fetal period, although it is also found <strong>in</strong>smaller amounts <strong>in</strong> the adult heart. 83 On this basis,treatment with EPO could prevent cardiomyocyteapoptosis and stimulate the production of myocardialblood vessels. In vitro and animal studies <strong>in</strong>dicate thatEPO is capable of reduc<strong>in</strong>g the apoptotic cell deathassociated with coronary ischemia/reperfusion. 90 Onehighly <strong>in</strong>terest<strong>in</strong>g possibility is that EPO stimulatesneovascularization, <strong>in</strong> part, because it <strong>in</strong>creases themobilization of endothelial progenitor cells from thebone marrow to the blood. 90CURRENT PERSPECTIVESAt this po<strong>in</strong>t, the issue can be summarized by say<strong>in</strong>gthat multiple partial data <strong>in</strong>dicate that the correction ofanemia provides tangible benefits <strong>in</strong> the natural historyand symptoms of heart failure, but that it is necessary toestablish the limits of these benefits and developsufficiently complex models for the application ofdiagnostic methods and treatment.The extensive material available justifies undertak<strong>in</strong>gtherapeutic efforts to correct anemia <strong>in</strong> HF. However, thedegree of uncerta<strong>in</strong>ty <strong>in</strong> fundamental aspects, bothpathogenic and those concern<strong>in</strong>g the therapeutic targets,is still significant. It is clear, as Roig stressed <strong>in</strong> this samejournal, 11 that one relevant aspect of anemia <strong>in</strong> HF is itscondition as a marker of severity. While prelim<strong>in</strong>arystudies <strong>in</strong>dicate that the treatment of anemia with ESAhas potentially beneficial effects, the available <strong>in</strong>formationdoes not enable us to reach more def<strong>in</strong>itive conclusions.In recent months, 2 large studies on anemia of CRDhave been published 91,92 ; the result<strong>in</strong>g data not only donot encourage the restoration of normal hemoglob<strong>in</strong>levels (13 g/dL), but <strong>in</strong>dicate that, despite the improvement<strong>in</strong> the functional class, there may be a greater number ofcardiovascular complications <strong>in</strong> patients <strong>in</strong> whom thecorrection of anemia is more complete. Other reportshad demonstrated that the tendency toward thedevelopment of left ventricular hypertrophy is not reversedwith the achievement of hemoglob<strong>in</strong> over 12 g/dL. Toillustrate the degree of controversy <strong>in</strong>volved, these datado not support the elevation of the treatment thresholdadvocated by the NKF <strong>in</strong> its 2006 guidel<strong>in</strong>es 15 and haveled to the proposal for the new version that we mentionedabove.With regard to issues specifically related to HF, at theEuropean Society of Cardiology meet<strong>in</strong>g held <strong>in</strong> 2006,data from another 2 double-bl<strong>in</strong>d, randomized, placebocontrolledstudies focus<strong>in</strong>g on the treatment of anemiaof HF with darbepoet<strong>in</strong> were provided. 93 All theRev Esp Cardiol. 2007;60(8):848-60 857
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>participants had an ejection fraction of 40% or less anda hemoglob<strong>in</strong> level of 9-12.5 g/dL, and HF had to havebeen diagnosed at least 3 months earlier. When the475 patients were analyzed as a whole, the <strong>in</strong>dividualswho had received darbepoet<strong>in</strong> alfa exhibited a significant<strong>in</strong>crease <strong>in</strong> their hemoglob<strong>in</strong> levels. However, while theydid not experience more adverse events than the placebogroup, they did not show a significant improvement <strong>in</strong>the 3 parameters for symptom evaluation (NYHAfunctional class, patient global assessment and theM<strong>in</strong>nesota Liv<strong>in</strong>g with <strong>Heart</strong> <strong>Failure</strong> Questionnaire).These results provide data to establish the limit toimprovement that can be expected with the treatment ofanemia.Together, these studies constitute a call to order toprevent us from overrat<strong>in</strong>g the positive role of thetreatments for anemia or, more exactly, support the needto improve the diagnostic accuracy and the correct choiceof the therapeutic tools. In summary, we can concludethat the correction of values <strong>in</strong>dicative of severe anemia(hemoglob<strong>in</strong> less than 10 g/dL) is beneficial, but that theachievement of values that surpass that level may notoffer additional advantages. The results of the largemulticenter studies that are currently be<strong>in</strong>g performedor are gett<strong>in</strong>g underway will probably help us to clarifyimportant practical aspects that have yet to be resolved.The largest of these studies (RED-HF) is now be<strong>in</strong>gcarried out. Its objective is to evaluate the effects ofdarbepoet<strong>in</strong> alfa on the morbidity and mortality rates <strong>in</strong>3400 patients with HF us<strong>in</strong>g a randomized, placebocontrolleddesign, which we hope will make it possibleto consolidate evidence-based treatment strategies.REFERENCES1. Szachniewicz J, Petruk-Kowalczyk J, Majda J, Kaczmarek A,Reczuch K, Kalra PR, et al. <strong>Anemia</strong> as an <strong>in</strong>dependent predictor ofpoor outcome <strong>in</strong> patients with chronic heart failure. Int J Cardiol.2003;90:303-8.2. Hunt SA, Baker DW, Ch<strong>in</strong> MH, C<strong>in</strong>quegrani MP, Feldman AM,Francis GS, et al. ACC/AHA guidel<strong>in</strong>es for the evaluation andmanagement of chronic heart failure: Executive Summary.Circulation. 2001;104:2996-3007.3. Hunt SA. ACC/AHA guidel<strong>in</strong>es for the evaluation and managementof chronic heart failure. J Am Coll Cardiol. 2005;46:e1-82.4. Crespo Leiro MG, Jiménez-Navarro M, Cabrera F, Sánchez PL.Insuficiencia cardiaca en el año 2006. Rev Esp Cardiol. 2007;60: 58-67.5. Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, KomajdaM, et al. Guías de práctica clínica sobre el diagnóstico y tratamientode la <strong>in</strong>suficiencia cardiaca crónica. Versión resumida (actualización2005). Rev Esp Cardiol. 2005;58:1062-92.6. Komajda M. Prevalence of anemia <strong>in</strong> patients with chronic heartfailure and their cl<strong>in</strong>ical characteristics. J Card Fail. 2004;10:S1-4.7. Pascual Hernández D, Serrano Sánchez JA, García Robles JA, MuñozAguilera R, Prieto Arévalo R. <strong>Anemia</strong> e <strong>in</strong>suficiencia cardiaca.Manual de <strong>in</strong>suficiencia cardiaca (diagnóstico y tratamiento de unapatología en expansión). Madrid: Just <strong>in</strong> Time; 2004. p. 70-3.8. Cohn JN, Tognoni G. A randomized trial of the angiotens<strong>in</strong>-receptorblocker valsartan <strong>in</strong> chronic heart failure. N Engl J Med. 2001;345:1667-75.9. Silverberg DS, Wexler D, Blum M, Keren G, Sheps D, LeibovitchE, et al. The Use of subcutaneous erythropoiet<strong>in</strong> and <strong>in</strong>travenousiron for the treatment of the anemia of severe, resistant congestiveheart failure improves cardiac and renal function and functionalcardiac class, and markedly reduces hospitalizations.J Am Coll Cardiol. 2000;35:1737-44.10. Ezekowitz A, McAlister FA, Armstrong PW. <strong>Anemia</strong> is common<strong>in</strong> heart failure and is associated with poor outcomes: <strong>in</strong>sights froma cohort of 12 065 patients with new-onset heart failure. Circulation.2003;107:223-5.11. Roig E. La anemia en la <strong>in</strong>suficiencia cardiaca. ¿Es un marcador degravedad o un objetivo terapéutico? Rev Esp Cardiol. 2005;58:10-2.12. Wisniacki N, Aimson P, Lyle M. Is anemia a cause of heart failure<strong>in</strong> the elderly? <strong>Heart</strong>. 2001;85 Suppl 1:P4.13. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR,Borenste<strong>in</strong> J. <strong>Anemia</strong> Is associated with worse symptoms, greaterimpairment <strong>in</strong> functional capacity and a significant <strong>in</strong>crease <strong>in</strong>mortality <strong>in</strong> patients with advanced heart failure. J Am Coll Cardiol.2002;39:1780–6.14. NKF-K/DOQI Cl<strong>in</strong>ical practice guidel<strong>in</strong>es for anemia of chronickidney disease: update 2000. Am J Kidney Dis. 2001;37(1 Supl1):S182-238.15. Cl<strong>in</strong>ical Practice Guidel<strong>in</strong>es and Cl<strong>in</strong>ical Practice Recommendationsfor <strong>Anemia</strong> <strong>in</strong> Chronic Kidney Disease <strong>in</strong> adults. CPG and CPR 2.1.Hb range. Am J Kidney Dis. 2006;47(5 Suppl 3):S16-85. Availablefrom: www.kidney.org/professionals/KDOQI/guidel<strong>in</strong>es_anemia/cpr21.htm16. Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A,Aguilar JC, et al. Study Group on Diagnosis of the Work<strong>in</strong>g Groupon <strong>Heart</strong> <strong>Failure</strong> of the European Society of Cardiology. The Euro<strong>Heart</strong><strong>Failure</strong> survey programme- a survey on the quality of care amongpatients with heart failure <strong>in</strong> Europe. Part 1: patient characteristicsand diagnosis. Eur <strong>Heart</strong> J. 2003;24:442-63.17. Chatterjee B, Nydegger UE, Mohacsi P. Serum erythropoiet<strong>in</strong> <strong>in</strong>heart failure patients treated with ACE-<strong>in</strong>hibitors or AT(1) antagonists.Eur J <strong>Heart</strong> Fail. 2000;2:393-8.18. Anand IS, Chandrashekhar Y, Ferrari R, Poole-Wilson PA, HarrisPC. <strong>Pathogenesis</strong> of oedema <strong>in</strong> chronic anaemia: studies of bodywater and sodium, renal function, haemodynamics and plasmahormones. Br <strong>Heart</strong> J. 1993;70:357-62.19. Androne AS, Katz SD, Lund L, LaManca J, Hudaihed A, HryniewiczK, et al. Hemodilution is common <strong>in</strong> patients with advanced heartfailure. Circulation. 2003;107:226-9.20. Okonko BS, Anker SD. <strong>Anemia</strong> <strong>in</strong> chronic heart failure: pathogeneticmechanisms. J Cardiac <strong>Failure</strong>. 2004;10 Suppl S:5-9.21. Calvillo L, Lat<strong>in</strong>i R, Kajstura J, Leri A, Anversa P, Ghezzi P, et al.Recomb<strong>in</strong>ant human erythropoiet<strong>in</strong> protects the miocardium fromischemia-perfusion <strong>in</strong>jury and promotes beneficial modell<strong>in</strong>g. ProcNatl Acad Sci USA. 2003;100:4802-6.22. Silverberg DS, Wexler D, Ia<strong>in</strong>a A. The role of anemia <strong>in</strong> theprogression of congestive heart failure. Is there a place forerythropoiet<strong>in</strong> and <strong>in</strong>travenous iron? J Nephrol. 2004;17:749-61.23. Weiss G, Goodnough LT. <strong>Anemia</strong> of chronic disease. N Engl J Med.2005;352:1011-23.24. Nanas JN, Matsouka C, Karageorgopoulos D, Leonti A, TsolakisE, Drakos SG, et al. Etiology of anemia <strong>in</strong> patients with advancedheart failure. J Am Coll Cardiol. 2006 19;48:2485-9.25. Gil P, Justo S, Castilla MA, Criado C, Caramelo C. Cardio-renal<strong>in</strong>sufficiency: the search for management strategies. Curr Op<strong>in</strong>Nephrol Hypertens. 2005;14:442-7.26. Caramelo C, Gil P. Insuficiencia comb<strong>in</strong>ada cardiorrenal: una claveevolutiva y terapéutica en el fallo cardíaco. Rev Esp Cardiol.2006;59:87-90.27. Grigorian Shamagian L, Varela Roman A, Pedreira Pérez M, GómezOtero I, Virgos Lamela A, González-Juanatey JR. El fracaso renales un factor de riesgo <strong>in</strong>dependiente en pacientes hospitalizados por<strong>in</strong>suficiencia cardiaca y se asocia con un peor perfil de riesgocardiovascular. Rev Esp Cardiol. 2006;59:99-108.858 Rev Esp Cardiol. 2007;60(8):848-60
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>28. de Jong PE, Gansevoort RT. Screen<strong>in</strong>g techniques for detect<strong>in</strong>g chronickidney disease. Curr Op<strong>in</strong> Nephrol Hypertens. 2005;14:567-72.29. Silverberg DS, Wexler D, Blum M, Ia<strong>in</strong>a A. The cardio-renal-anemiasydrome. Correct<strong>in</strong>g anemia <strong>in</strong> patients with resistant congestiveheart failure can improve both cardiac and renal function and reducehospitalizations. Cl<strong>in</strong> Nephrol. 2003;60 Suppl 1S:93-102.30. Kazmi WH, Kausz AT, Khan S, Abichandani R, Ruthazer R, ObradorGT, et al. <strong>Anemia</strong>: an early complication of chronic renal<strong>in</strong>sufficiency. Am J Kidney Dis. 2001;38:803-12.31. Hsu CY, McCulloch CE, Curhan GC. Epidemiology of anemiaassociated with chronic renal <strong>in</strong>sufficiency among adults <strong>in</strong> theUnited States: results from the Third National Health and NutritionExam<strong>in</strong>ation Survey. J Am Soc Nephrol. 2002;13:504-10.32. Jelkmann W. Pro<strong>in</strong>flammatory cytok<strong>in</strong>es lower<strong>in</strong>g erythropoiet<strong>in</strong>production. J Interferon Cytok<strong>in</strong>e Res. 1998;18:555-9.33. Goicoechea M, Mart<strong>in</strong> J, De Sequera P, Quiroga JA, Ortiz A, CarreñoV, et al. Role of cytok<strong>in</strong>es <strong>in</strong> the response to erythropoiet<strong>in</strong> <strong>in</strong>hemodyalisis patients. Kidney Int. 1998;54:1337-43.34. Atanasiu V, Manolescu B, Stoian I. Hepcid<strong>in</strong>: central regulator ofiron metabolism. Eur J Haematol. 2007;78:1-10.35. Ganz T. Hepcid<strong>in</strong>: a peptide hormone at the <strong>in</strong>terface of <strong>in</strong>nateimmunity and iron metabolism. Curr Top Microbiol Immunol.2006;306:183-98.36. Ishani A, Ww<strong>in</strong>handL E, Zhao Z, Gilbertson ST, Coll<strong>in</strong>s AJ, YusufS, et al. Angiotens<strong>in</strong>-convert<strong>in</strong>g enzyme <strong>in</strong>hibitor as a risk factorfor the development of anemia, and the impact of <strong>in</strong>cident anemiaon mortality <strong>in</strong> patients with left ventricular dysfunction. J Am CollCardiol. 2005;45:391-9.37. Lupon J, Urrutia A, González B, Herreros J, Altimir S, Coll R, etal. Prognostic significance of hemoglob<strong>in</strong> levels <strong>in</strong> patients withheart failure. Rev Esp Cardiol. 2005;58:48-53.38. Volpe M, Tritto C, Testa U, Rao MA, Martucci R, Mirante A, et al.Blood levels of erythropoiet<strong>in</strong> <strong>in</strong> congestive heart failure andcorrelation with cl<strong>in</strong>ical, hemodynamic, and hormonal profiles. AmJ Cardiol. 1994;74:468-73.39. Jensen JD, Eiskjaer H, Bagger JP, Pedersen EB. Elevated level oferythropoiet<strong>in</strong> <strong>in</strong> congestive heart failure relationship to renalperfusion and plasma ren<strong>in</strong>. J Intern Med. 1993;233:125-30.40. Fyhrquist F, Karpp<strong>in</strong>en K, Honkanen T, Saijonmaa O, Rosenlof K.High serum erythropoiet<strong>in</strong> levels are normalized dur<strong>in</strong>g treatmentof congestive heart failure with enalapril. J Intern Med. 1989;226:257-60.41. Marathias KP, Agroyannis B, Mavromoustakos T, Matsoukas J,Vlahakos DVl. Hematocrit-lower<strong>in</strong>g effect follow<strong>in</strong>g <strong>in</strong>activationof renn<strong>in</strong>-angiotens<strong>in</strong> system with angiotens<strong>in</strong> convert<strong>in</strong>g enzyme<strong>in</strong>hibitors and angiotens<strong>in</strong> receptor blockers. Curr Top Med Chem.2004;4:483-6.42. Albitar S, Gen<strong>in</strong> R, Fen-Chong M, Serveauz M-O, Bourgeon B.High dose enalapril impairs the response to erythropoiet<strong>in</strong> treatment<strong>in</strong> haemodialysis patients. Nephrol Dial Transplant. 1998; 13:1206-10.43. Donnelly SM, Millar JA. Losartan may modulate erythropoiet<strong>in</strong>production. J Ren<strong>in</strong> Angiotens<strong>in</strong> Aldosterone Syst. 2001;2: 255-60.44. Mozaffarian D, Nye R, Levy WC. <strong>Anemia</strong> Predicts Mortality <strong>in</strong> Severe<strong>Heart</strong> <strong>Failure</strong> The Prospective Randomized Amlodip<strong>in</strong>e SurvivalEvaluation (PRAISE). J Am Coll Cardiol. 2003;41:1933-9.45. Mcmurray JJV. What Are the cl<strong>in</strong>ical consequences of anemia <strong>in</strong>patients with chronic heart failure? J Cardiac <strong>Failure</strong>. 2004;10 SupplS:10-12.46. Al-Ahmad A, Rand WM, Manjunath G, Konstam MA, Salem DN,Levey AS, et al. Reduced kidney function and anemia as risk factorsfor mortality <strong>in</strong> patients with left ventricular dysfunction. J Am CollCardiol. 2001;38:955-62.47. Felker GM, Gattis WA, Leimberger JD, Adams KF, Cuffe MS,Gheorghiade M, et al. Usefulness of anemia as a predictor of deathand rehospitalization <strong>in</strong> patients with decompensated heart failure.Am J Cardiol. 2003;92:625-8.48. Lupon J, Urrutia A, González B, Herreros J, Altimir S, Coll R, et al.Significado pronóstico de los valores de hemoblog<strong>in</strong>a en pacientescon <strong>in</strong>suficiencia cardiaca. Rev Esp Cardiol. 2005;58:48-53.49. Kosiborod M, Curtis JP, Wang Y, Smith GL, Masoudi FA, FoodyJM, et al. <strong>Anemia</strong> and outcomes <strong>in</strong> patients with heart failure: astudy from the national heart care project. Arch Intern Med.2005;165:2237-44.50. Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, BarrePE. The impact of anemia on cardiomyopathy, morbidity, and andmortality <strong>in</strong> end-stage renal disease. Am J Kidney Dis. 1996; 28:53-61.51. Chatterjee PK. Pleiotropic renal actions of erythropoiet<strong>in</strong>. Lancet.2005;365:1890-2.52. Macdougall IC, Eckardt KU. Novel strategies for stimulat<strong>in</strong>gerythropoiesis and potential new treatments for anaemia. Lancet.2006;368:947-52.53. Sharmaa R, Francisa DP, Pittb B, Poole-Wilsona PA, Coatsa AJS,Ankera SD. Haemoglob<strong>in</strong> predicts survival <strong>in</strong> patients with chronicheart failure: a substudy of the ELITE II trial. European <strong>Heart</strong>.2004;25:1021-8.54. Kalra PR, Bolger AP, Francis DP, Genth-Zotz S, Sharma R,Ponikowski PP, et al. Effect of anemia on exercise tolerance <strong>in</strong>chronic heart failure <strong>in</strong> men. Am J Cardiol. 2003;91:888-91.55. Lacombe C, Mayeux P. The molecular biology of erythropoiet<strong>in</strong>.Nephrol Dial Transplant. 1999;14 Suppl 2:22-8.56. Fisher JW. Erythropoiet<strong>in</strong>: physiology and pharmacology update.Exp Biol Med. 2003;228:1-14.57. Jelkmann W. Molecular biology of erythropoiet<strong>in</strong>. Intern Med.2004;43:649-59.58. Eckardt KU. Erythropoiet<strong>in</strong> production <strong>in</strong> liver and kidneys. CurrOp<strong>in</strong> Nephrol Hypertens. 1996;5:28-34.59. Caramelo C, Pena Deudero JJ, Castilla A, Justo S, de Solis AJ, NeriaF, et al. Response to hypoxia. A systemic mechanism based on thecontrol of gene expression. Medic<strong>in</strong>a (Buenos Aires). 2006;66:155-64.60. Nangaku M, Eckardt KU. <strong>Pathogenesis</strong> of renal anemia. Sem Nephrol.2006;26:261-8.61. Hirota K, Semenza GL. Regulation of angiogenesis by hypoxia<strong>in</strong>duciblefactor 1. Crit Rev Oncol Hematol. 2006;59:15-26.62. Warnecke C, Zaborowska Z, Kurreck J, Erdmann VA, Frei U,Wiesener M, et al. Differentiat<strong>in</strong>g the functional role of hypoxia<strong>in</strong>duciblefactor (HIF)-1alpha and HIF-2alpha (EPAS-1) by the useof RNA <strong>in</strong>terference: erythropoiet<strong>in</strong> is a HIF-2alpha target gene <strong>in</strong>Hep3B and Kelly cells. FASEB J. 2004;18:1462-4.63. Eckardt KU. Anaemia <strong>in</strong> end-stage renal disease: pathophysiologicalconsiderations. Nephrol Dial Transplant. 2001;16 Suppl 7: 2-8.64. Jiang BJ, Semenza GL, Bauer C, Marti HH. Hypoxia-<strong>in</strong>duciblefactor 1 levels vary exponentially over a physiological relevant rangeof O2 tension. Am J Physiol. 1996;271:C1172-80.65. Eckardt KU, Rosenberger C, Jürgensen JS, Wiesener MS. Role ofhypoxia <strong>in</strong> the pathogenesis of renal disease. Blood Purif. 2003;21:253-7.66. Pham I, Andrivet P, Sediame S, Defouilloy C, Moutereau S, Wirqu<strong>in</strong>V, et al. Increased erythropoiet<strong>in</strong> synthesis <strong>in</strong> patients with COLDor left heart failure is related to alterations <strong>in</strong> renal haemodynamics.Eur J Cl<strong>in</strong> Invest. 2001;31:103-9.67. Eckardt K, Kurtz A, Bauer C. Regulation of erythropoiet<strong>in</strong> productionis related to proximal tubular function. Am J Physiol. 1989;256:F942-7.68. van der Meer P, Voors AA, Lipsic E, Smilde TDJ, van Gilst WH,van Veldhuisen DJ. Prognostic value of plasma erythropoiet<strong>in</strong> onmortality <strong>in</strong> patients with chronic heart failure. J Am Coll Cardiol.2004;44:63-7.69. Benöhr P, Harsch S, Proksch, Gleiter C. Does angiotens<strong>in</strong> II modulateerythropoiet<strong>in</strong> production <strong>in</strong> HepG2 cells? Nephron Exp Nephrol.2004;98:e124-31.70. Levy BI. How to expla<strong>in</strong> the differences between ren<strong>in</strong> angiotens<strong>in</strong>system modulators. Am J Hypertens. 2005;18:134S-41S.71. Grossmann J, Burkhardt R, Harder S, Lenz T, SedLmeyer A,Kl<strong>in</strong>khardt U, et al. Angiotens<strong>in</strong> II <strong>in</strong>fusion <strong>in</strong>creases plasmaerythropoiet<strong>in</strong> levels via an angiotens<strong>in</strong> II type 1 receptor-dependentpathway. Kidney Int. 2001;60:83-6.Rev Esp Cardiol. 2007;60(8):848-60 859
Caramelo C et al. <strong>Anemia</strong> <strong>in</strong> <strong>Heart</strong> <strong>Failure</strong>72. Kato H, Ishida J, Imagawa S, Saito T, Suzuki N, Matsuoka T, et al.Enhanced erythropoiesis mediated by activation of the ren<strong>in</strong>angiotens<strong>in</strong>system via angiotens<strong>in</strong> II type 1a receptor. FASEB J.2005;19:2023-5.73. Nangaku M, Eckardt KU. <strong>Pathogenesis</strong> of renal anemia. Sem<strong>in</strong>Nephrol. 2006;26:261-8.74. Álvarez Arroyo MV, Castilla MA, González Pacheco FR, Tan D,Riesco A, Casado S, et al. Role of vascular endothelial growth factoron erythropoiet<strong>in</strong>-related endothelial cell proliferation. J Am SocNephrol. 1998;9:1998-2004.75. Lacombe C. Resistance to erythropoiet<strong>in</strong>. N Eng J Med. 1996;334:660-2.76. National Kidney Foundation. K/DOQI cl<strong>in</strong>ical practice guidel<strong>in</strong>esfor chronic kidney disease: evaluation, classification, and stratification.kidney disease outcome quality <strong>in</strong>itiative. Am J Kidney Dis. 2002;39Suppl 1:S1-S266.77. KDOQI Cl<strong>in</strong>ical Practice Guidel<strong>in</strong>es and Cl<strong>in</strong>ical PracticeRecommendations for <strong>Anemia</strong> <strong>in</strong> Chronic Kidney Disease. WorkGroup of <strong>Anemia</strong> <strong>in</strong> Chronic Kidney Disease. Am J Kidney Dis.2006;47(5 Suppl 3):S11-145.78. Eschbach JW. <strong>Treatment</strong> of <strong>Anemia</strong> of Chronic Kidney Disease.79. Locatelli F, Aljama P, Bárány P,Canaud B, Carrera F, Eckardt KV,et al. Revised European Best Practice Guidel<strong>in</strong>es for the Managementof Anaemia <strong>in</strong> Patients With Chronic Renal <strong>Failure</strong>. Nephrol DialTransplant. 2004;19 Suppl 2:ii1-47.80. Cleland JG, Sullivan JT, Ball S, Horowitz JD, Agoram B, RosserD, et al. Once-monthly adm<strong>in</strong>istration of darbepoet<strong>in</strong> alfa for thetreatment of patients with chronic heart failure and anemia: apharmacok<strong>in</strong>etic and pharmacodynamic <strong>in</strong>vestigation. J CardiovascPharmacol. 2005;46:155-61.81. Melnikova I. Anaemia therapies. Nature Rev Drug Discovery.2006;5:627-8.82. Manc<strong>in</strong>i DM, Katz SD, Lang CC, LaManca J, Hudaihed A, AndroneAS. Effect of erythropoiet<strong>in</strong> on exercise capacity <strong>in</strong> patients withmoderate to severe chronic heart failure. Circulation. 2003;107:294-9.83. Grabe DW. Update on cl<strong>in</strong>ical practice recommendations and newtherapeutic modalities for treat<strong>in</strong>g anemia <strong>in</strong> patients with chronickidney disease. Am J Health Syst Pharm. 2007;64(13 Suppl 8):S8-14.84. Katz ST, Manc<strong>in</strong>i D, Androne AS, Hryniewicz K. <strong>Treatment</strong> ofanemia <strong>in</strong> patients with chronic heart failure. Circulation. 2003;107:294-9.85. Silverberg DS, Blum M, Agbaria Z, Schwartz D, Zubkov A, Yachn<strong>in</strong>T, et al. Intravenous iron f for the treatment of predialysis anemia.Kidney Int Suppl. 1999;69:S79-85.86. Fishbane S, Frei GL, Maesaka J. Reduction <strong>in</strong> recomb<strong>in</strong>ant humanerythropoiet<strong>in</strong> doses by the use of chronic <strong>in</strong>travenous ironsupplementation. Am J Kidney Dis. 1995;26:41-6.87. Bolger AP, Bartlett FR, Penston HS, O’Leary J, Pollock N, KaprielianR, et al. Intravenous iron alone for the treatment of anemia <strong>in</strong> patientswith chronic heart failure. J Am Coll Cardiol. 2006;48:1225-7.88. Shaw R. Viewpo<strong>in</strong>t: heart failure and anaemia: a concept returns tothe fore. Circulation. 2006 10;114:f157-8.89. Beck-da-Silva L, Rohde LE, Pereira-Barretto AC, De AlbuquerqueD, Bocchi E, Vilas-Boas F, et al. Rationale and design of the IRON-HF study: a randomized trial to assess the effects of ironsupplementation <strong>in</strong> heart failure patients with anemia. J Card Fail.2007;13:14-7.90. van der Meer P, Voors AA, Lipsic E, van Gilst WH, van VeldhuisenDJ. Erytropoiet<strong>in</strong> <strong>in</strong> cardiovascular diseases. Eur <strong>Heart</strong> J. 2004;25:285-91.91. S<strong>in</strong>gh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M,et al; CHOIR Investigators. Correction of anemia with epoet<strong>in</strong> alfa<strong>in</strong> chronic kidney disease. N Engl J Med. 2006;355:2085-98.92. Drueke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, TsakirisD, et al. Normalization of hemoglob<strong>in</strong> level <strong>in</strong> patients with chronickidney disease and anemia. N Engl J Med. 2006; 355:2071-84.93. Coletta AP, T<strong>in</strong> L, Loh PH, Clark AL, Cleland JGF. Cl<strong>in</strong>ical trialsupdate from the European Society of Cardiology heart failure meet<strong>in</strong>g:TNT subgroup analysis, darbepoet<strong>in</strong> alfa, FERRIC-HF and KW-3902. Eur J <strong>Heart</strong> Fail. 2006;8:547-9.860 Rev Esp Cardiol. 2007;60(8):848-60