Orthopedic Trauma in Pregnancy - The Journal of Family Practice
Orthopedic Trauma in Pregnancy - The Journal of Family Practice
Orthopedic Trauma in Pregnancy - The Journal of Family Practice

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
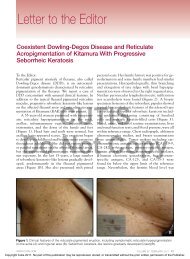
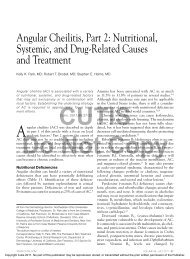
A Review Paper<strong>Orthopedic</strong> <strong>Trauma</strong> <strong>in</strong> <strong>Pregnancy</strong>Pratik Desai, MD, and Michael Suk, MD, JD, MPHAbstract<strong>Trauma</strong> susta<strong>in</strong>ed dur<strong>in</strong>g pregnancy can trigger uncerta<strong>in</strong>tyand anxiety for patient and orthopedic surgeonalike. In particular, orthopedic-related <strong>in</strong>juriesraise concerns about preoperative, <strong>in</strong>traoperative, andpostoperative care. In this article, we review commonconcerns about radiation exposure, leukemia,pa<strong>in</strong> management, anticoagulation, and anesthesia.One f<strong>in</strong>d<strong>in</strong>g is that radiation risk is m<strong>in</strong>imal when obta<strong>in</strong><strong>in</strong>gx-rays for operative plann<strong>in</strong>g, provided that the cumulativedose is with<strong>in</strong> 5 rad. We also address safety concernsabout patient position<strong>in</strong>g and staff radiation exposure.In addition, we found that most anesthetics used <strong>in</strong>pregnancy are category C (ie, safe). Perioperative opioiduse for pa<strong>in</strong> management is recommended with little risk.Regard<strong>in</strong>g anticoagulation, low-molecular-weight hepar<strong>in</strong>and fondapar<strong>in</strong>ux are the safest choices. Last, pregnancyis not a contra<strong>in</strong>dication to operative management <strong>of</strong> pelvicand acetabular fractures.<strong>Pregnancy</strong> elicits a component <strong>of</strong> musculoskeletalpa<strong>in</strong> or discomfort for most women that has beenwell chronicled. In 1994, Heckman and Sassard 1concisely reviewed musculoskeletal conditionsencountered dur<strong>in</strong>g pregnancy, such as low back pa<strong>in</strong>, carpaltunnel syndrome, de Querva<strong>in</strong> tenosynovitis, leg cramps, andhip pa<strong>in</strong>. <strong>The</strong>y also commented on changes occurr<strong>in</strong>g dur<strong>in</strong>gpregnancy <strong>of</strong> preexist<strong>in</strong>g musculoskeletal conditions, suchas rheumatoid arthritis and ankylos<strong>in</strong>g spondylitis. S<strong>in</strong>cetheir review appeared, other authors <strong>in</strong> the nonorthopedic literaturehave commented on similar conditions and physicalexam<strong>in</strong>ation maneuvers to elicit them. 2<strong>The</strong> case that we describe here led us to search the literaturefor answers to practical concerns <strong>in</strong> global fracturemanagement dur<strong>in</strong>g pregnancy. It quickly became clearthat this search would be labor-<strong>in</strong>tensive and would yieldmany sources but few from the orthopedic literature. We<strong>in</strong>clude our f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> this article, which can be considereda useful resource for orthopedic surgeons.Dr. Desai is a Resident, Department <strong>of</strong> Orthopaedics andRehabilitation, and Dr. Suk is Assistant Pr<strong>of</strong>essor and Director,Orthopaedic <strong>Trauma</strong> Service, Department <strong>of</strong> Orthopaedics andRehabilitation, University <strong>of</strong> Florida Health Science Center,Jacksonville, Florida.Requests for repr<strong>in</strong>ts: Pratik Desai, MD, Department <strong>of</strong>Orthopaedics and Rehabilitation, 655 W 8th St, ACC Build<strong>in</strong>g, 2ndFloor, University <strong>of</strong> Florida Health Science Center, Jacksonville,FL 32209 (tel, 904-244-7757; fax, 904-244-3457; e-mail, pratik.desai@jax.ufl.edu).Am J Orthop. 2007;36(11):E160-E166. Copyright QuadrantHealthCom Inc. 2007. All rights reserved.We <strong>in</strong>clude practical considerations perta<strong>in</strong><strong>in</strong>g to preoperative,operative, and postoperative management <strong>of</strong>orthopedic <strong>in</strong>jury dur<strong>in</strong>g pregnancy. Through a review <strong>of</strong>the literature <strong>of</strong> the past 25 years, we provide the orthopediccommunity with current <strong>in</strong>formation from multidiscipl<strong>in</strong>arysources to assist <strong>in</strong> global fracture management.We focus on concerns <strong>in</strong>volv<strong>in</strong>g radiation exposure,anesthesia, pa<strong>in</strong> control, anticoagulation, and treatment <strong>of</strong>pelvic/acetabular fractures.“[This paper provides] areview <strong>of</strong> the literature <strong>of</strong>the past 25 years.”Case ExampleA woman <strong>in</strong> her early 20s with a 24-week <strong>in</strong>trauter<strong>in</strong>epregnancy (IUP) susta<strong>in</strong>ed an isolated closed femur fractureas an unrestra<strong>in</strong>ed driver <strong>in</strong> a motor vehicle collisionand presented to the trauma center at our <strong>in</strong>stitution. Shehad no prior medical or surgical history. On physicalexam<strong>in</strong>ation, she had a visible deformity about her rightthigh without any open wounds. She was neurovascularly<strong>in</strong>tact. X-rays showed a midshaft femur fracture with moderatedisplacement. Focused assessment with sonographyfor trauma (FAST study) revealed good fetal motion andfetal <strong>in</strong>dices (Figures 1, 2). A consultation with obstetricianswas obta<strong>in</strong>ed because <strong>of</strong> questions about fetal monitor<strong>in</strong>gand risks associated with <strong>in</strong>tramedullary nail<strong>in</strong>g,anesthesia, pa<strong>in</strong> medication, and anticoagulation. In theirjudgment, fetal monitor<strong>in</strong>g was unnecessary, as the fetuswas still nonviable (≤24 weeks IUP). No anticoagulationwas necessary, as the patient was ambulatory immediatelyafter surgery. <strong>The</strong> patient had no other associated <strong>in</strong>juries,and a multidiscipl<strong>in</strong>ary decision was made to take thepatient emergently to the operat<strong>in</strong>g room.A retrograde <strong>in</strong>tramedullary nail was placed withoutcomplications under fluoroscopic guidance (Figure 3).<strong>The</strong> patient was discharged on postoperative day 3. At 34weeks gestation, she began weight-bear<strong>in</strong>g as toleratedand had m<strong>in</strong>or knee pa<strong>in</strong>.Radiation ExposureOne <strong>of</strong> the most anxiety-provok<strong>in</strong>g aspects <strong>of</strong> fracturecare for patient and physician is radiation exposure to themother and fetus and possible teratogenesis.Risk PerceptionResults from numerous studies <strong>of</strong> nuclear bomb survivorshave shown that the teratogenicity <strong>of</strong> radiation is dose-E160 <strong>The</strong> American <strong>Journal</strong> <strong>of</strong> <strong>Orthopedic</strong>s ®
P. Desai and M. SukABFigure 3. Anteroposterior (A) and lateral (B) postoperativex-rays.Figure 1. Ultrasound at 24-week <strong>in</strong>trauter<strong>in</strong>e pregnancy.AFigure 2. Lateral (A) and anteroposterior (B) x-rays <strong>of</strong> <strong>in</strong>jury.Bdependent. In addition, the most critical and vulnerable period<strong>in</strong> utero for central nervous system damage is 8 to 15 weeks<strong>of</strong> gestation. However, <strong>in</strong> a recent review <strong>of</strong> the literature,De Santis and colleagues 3 found that, though ioniz<strong>in</strong>g radiationrepresents a possible teratogen to the fetus, “<strong>in</strong>advertentexposure[s] from diagnostic procedures <strong>in</strong> pregnancy … donot <strong>in</strong> most cases <strong>in</strong>crease the natural risk <strong>of</strong> congenital anomalies.”Furthermore, they recommended that, if a maternal<strong>in</strong>dication for radiologic imag<strong>in</strong>g exists, and the <strong>in</strong>formationcannot be obta<strong>in</strong>ed by other methods, the physician shouldnot hesitate to order such studies. <strong>The</strong> only caveat they <strong>of</strong>feredwas that maternal thyroid gland exposure to diagnostic radiationwas associated with slight decreases <strong>in</strong> birth weight.Physicians’ perceptions <strong>of</strong> teratogenic risk associatedwith radiation exposure <strong>in</strong> early pregnancy were recentlystudied. 4 Four hundred family physicians and 100 obstetricianswere asked about their perceptions <strong>of</strong> risk to <strong>of</strong>fspr<strong>in</strong>gassociated with any abdom<strong>in</strong>al pla<strong>in</strong> x-ray or computedtomography (CT) scan. Although subjects were <strong>in</strong>formed<strong>of</strong> the basel<strong>in</strong>e <strong>of</strong> 1% to 3% risk <strong>of</strong> major malformations <strong>in</strong>any pregnancy, results proved that the perceived risks wereunrealistically high and warranted education <strong>of</strong> the medicalcommunity. Forty-four percent <strong>of</strong> family physicians and11% <strong>of</strong> obstetricians estimated the risk to be higher than5% with abdom<strong>in</strong>al x-ray, and 61% <strong>of</strong> family physiciansand 34% <strong>of</strong> obstetricians estimated the risk to be higher than5% with abdom<strong>in</strong>al CT. Undoubtedly, such misperceptionscan lead to <strong>in</strong>creased maternal anxiety and <strong>in</strong>correct recommendationsto term<strong>in</strong>ate pregnancy. <strong>The</strong> American College <strong>of</strong>Obstetricians and Gynecologists 5 provided guidel<strong>in</strong>es for x-ray exam<strong>in</strong>ations or exposure dur<strong>in</strong>g pregnancy (Table I).Imag<strong>in</strong>g Guidel<strong>in</strong>esUnits generally used to measure the effects <strong>of</strong> x-ray <strong>in</strong>cluderad, roentgen equivalents man (rem), gray (Gy), and sievert(Sv). In the literature, any <strong>of</strong> these units may be used, and itis therefore important to understand their conversions. Forthe purpose <strong>of</strong> diagnostic x-rays, 1 Gy = 1 Sv = 100 rad =100 rem. Fetal risks <strong>of</strong> growth restriction, anomalies, andabortions are not <strong>in</strong>creased with ioniz<strong>in</strong>g radiation exposures<strong>of</strong> less than 5 rad. 5 Growth retardation, microcephaly,and mental retardation are observable at exposures higherthan 50 rad. 6 Putt<strong>in</strong>g this <strong>in</strong> perspective <strong>in</strong>volves be<strong>in</strong>gaware <strong>of</strong> the estimated fetal exposure from common radiologicprocedures 5 (Table II).Pla<strong>in</strong> x-rays generally result <strong>in</strong> fetal exposures <strong>in</strong> the milliradrange. Moreover, x-rays <strong>of</strong> extremities (ie, humerus,forearm, tibia) allow placement <strong>of</strong> a lead apron over thepatent to further m<strong>in</strong>imize exposure doses. Exposure fromCT depends on slice thickness and therefore the number <strong>of</strong>necessary cuts. Spiral CT has the added dimension <strong>of</strong> pitch,but, with customary use <strong>of</strong> pitch higher than or equal to 1,the exposure dose <strong>of</strong> conventional and spiral CT is the same.It was recently reported that exposure from CT is 1.5 rad butcan be reduced to as little as 250 millirad. 7November 2007 E161
<strong>Orthopedic</strong> <strong>Trauma</strong> <strong>in</strong> <strong>Pregnancy</strong>Table I. Guidel<strong>in</strong>es for X-Ray Exam<strong>in</strong>ation or Exposure Dur<strong>in</strong>g <strong>Pregnancy</strong>1. Women should be counseled that x-ray exposure from a s<strong>in</strong>gle diagnostic procedure does not result <strong>in</strong> harmful fetal effects.2. Specifically, exposure to less than 5 rad has not been associated with an <strong>in</strong>crease <strong>in</strong> fetal anomalies or pregnancy loss.3. Concern about high-dose ioniz<strong>in</strong>g radiation exposure should not prevent medically <strong>in</strong>dicated diagnostic x-ray procedures from be<strong>in</strong>gperformed <strong>in</strong> pregnancy.4. Other imag<strong>in</strong>g procedures not associated with ioniz<strong>in</strong>g radiation (magnetic resonance imag<strong>in</strong>g, ultrasonography) should be considered<strong>in</strong>stead <strong>of</strong> x-rays when appropriate, as they are not known to be l<strong>in</strong>ked with adverse fetal effects.5. Use <strong>of</strong> radioactive isotopes <strong>of</strong> iod<strong>in</strong>e is contra<strong>in</strong>dicated dur<strong>in</strong>g pregnancy.6. Radiopaque and paramagnetic contrast agents are unlikely to cause harm and may be <strong>of</strong> diagnostic benefit, but these agents should beused only if the potential benefit justifies the potential risk to the fetus.Data from ACOG Committee on Obstetric <strong>Practice</strong>. ACOG Committee Op<strong>in</strong>ion. Number 299, September 2004 (replaces No. 158, September 1995). Guidel<strong>in</strong>esfor diagnostic imag<strong>in</strong>g dur<strong>in</strong>g pregnancy. Obstet Gynecol. 2004;104(3):647-651.Table II. Radiation Exposure Doses for <strong>Orthopedic</strong> X-Rays*ProcedureFetal ExposureChest x-ray (anteroposterior/lateral)Abdom<strong>in</strong>al pla<strong>in</strong> x-rayHip x-ray (s<strong>in</strong>gle view)Head or chest CTAbdomen and lumbar sp<strong>in</strong>e CTPelvis CTAnteroposterior pelvisComplete sp<strong>in</strong>e series*CT, computed tomography.0.02-0.07 mrad100 mrad200 mrad
P. Desai and M. SukTable III. Categories <strong>of</strong> Medication Safety <strong>in</strong> <strong>Pregnancy</strong>A Well-controlled studies show no risk <strong>in</strong> first trimester; no evidence <strong>of</strong> risk <strong>in</strong> later pregnancy.B Animal and human studies do not show fetal risk; no controlled studies confirm risk <strong>in</strong> pregnancy; no evidence <strong>of</strong> risk <strong>in</strong> later pregnancy.C Animal studies show adverse fetal effects; no controlled studies <strong>in</strong> pregnancy.D Studies show fetal damage; use may be acceptable when conditions threaten woman’s life.X Studies <strong>in</strong> animals and humans show fetal damage; absolutely contra<strong>in</strong>dicated <strong>in</strong> pregnancy.Data from Hart MA. Help! My orthopaedic patient is pregnant! Orthop Nurs. 2005;24(2):108-114.Table IV. Pert<strong>in</strong>ent Risk Factors forDevelopment <strong>of</strong> Thromboemboli<strong>Pregnancy</strong><strong>Family</strong> historyIncreased maternal agePrior deep venous thrombosisCesarean sectionThrombophiliaData from Robertson L, Greer I. Thromboembolism <strong>in</strong> pregnancy. Curr Op<strong>in</strong>Obstet Gynecol. 2005;17(2):113-116.nant patients. For pla<strong>in</strong> x-rays, this precaution is achievedby plac<strong>in</strong>g the 0.5-mm lead apron on the surface <strong>of</strong> theabdomen/pelvis. <strong>The</strong>se differences are attributable to thedirectional source <strong>of</strong> the ioniz<strong>in</strong>g radiation. Direct patientshield<strong>in</strong>g is not typically used <strong>in</strong> CT because <strong>of</strong> the rotationalnature <strong>of</strong> the exposure. 13Staff SafetyBesides patient concerns, concerns <strong>of</strong> the orthopedic surgeonand support<strong>in</strong>g staff <strong>of</strong> childbear<strong>in</strong>g age must also be considered.In a recent study <strong>in</strong> Greece, <strong>The</strong>ocharopoulos andcolleagues 14 used an anthropomorphic phantom consist<strong>in</strong>g <strong>of</strong>a synthetic skeleton embedded <strong>in</strong> tissue-equivalent materialsto calculate pregnancy workloads on the basis <strong>of</strong> a 2-mSvexposure limit to a gravid abdomen and to correlate embryodose with the read<strong>in</strong>g <strong>of</strong> a pregnancy-dedicated dosimeter.<strong>The</strong>ir study, based on treatment <strong>of</strong> a closed femur fracture,produced valuable results. <strong>The</strong> authors concluded that scatterradiation dur<strong>in</strong>g fluoroscopically assisted femur surgery ismore pronounced on the side ipsilateral to the operative site.<strong>The</strong>y also stated that fears <strong>of</strong> occupationally exposed personnelare unjustified if standard 0.5-mm lead-equivalent apronsare worn, and they concluded, “<strong>Pregnancy</strong> will not <strong>in</strong>hibit thework<strong>in</strong>g career <strong>of</strong> the staff and does not provide grounds forpr<strong>of</strong>essional discrim<strong>in</strong>ation.” Other methods <strong>of</strong> fetus protectionare 14 :●• Mov<strong>in</strong>g from treated side to contralateral side results <strong>in</strong> 13- to 57-fold decrease <strong>in</strong> exposure.●• Mov<strong>in</strong>g 0.5 m cephalad from entry beam reduces surgeonexposure 13-fold.●• Mov<strong>in</strong>g 1.5 m away from table reduces exposure by factor <strong>of</strong> 26on ipsilateral side and by factor <strong>of</strong> 6 on contralateral side.●• Exposure is <strong>in</strong>significant more than 2 m from source <strong>of</strong> radiation.Data from <strong>The</strong>ocharopoulos N, Damilakis J, Peris<strong>in</strong>akis K, PapadokostakisG, Hadjipavlou A, Gourtsoyiannis N. Image-guided reconstruction <strong>of</strong> femoralfractures: is the staff progeny safe? Cl<strong>in</strong> Orthop. 2005;(430):182-188.AnesthesiaEach year, more than 75,000 pregnant women undergo nonobstetricsurgery. It is well established that many pregnantwomen are safely anesthetized daily without adverse effectsto fetus or mother. 15 Concerns about operative anesthesiama<strong>in</strong>ly surround teratogenicity <strong>of</strong> anesthetic agents used.Currently, drug categories are used to determ<strong>in</strong>e and labelmedications with respect to fetal risk 16 (Table IV).Nearly all anesthetics and analgesics used <strong>in</strong> pregnancyare category C. 16 Almost all teratogenic medications have thesame effect on animals as on humans, which makes animalstudy results very reliable and applicable. Moreover, anestheticsused <strong>in</strong> pregnancy are known to cause a variety <strong>of</strong> physiologicchanges, <strong>of</strong> which the surgeon and the anesthesiologistshould be aware. 17 In 1989, report<strong>in</strong>g on a study <strong>of</strong> 5405operations dur<strong>in</strong>g pregnancy and anesthesia-related outcomes,Mazze and Kallen 18 concluded that the <strong>in</strong>cidence <strong>of</strong> malformationsand stillbirths was not <strong>in</strong>creased <strong>in</strong> the <strong>of</strong>fspr<strong>in</strong>g <strong>of</strong>women hav<strong>in</strong>g surgery. However, there was <strong>in</strong>creased <strong>in</strong>cidence<strong>of</strong> low and very low birthweight <strong>in</strong>fants, and the authorsconcluded, “Nonobstetric operations dur<strong>in</strong>g pregnancy arenot without hazard.” Rosen 19 studied the effects <strong>of</strong> anestheticagents on the fetus and concluded that the adverse effects onthe fetus are mostly the result <strong>of</strong> underly<strong>in</strong>g disease and notthe agent used.Position<strong>in</strong>g and Monitor<strong>in</strong>gIssuesIt is well documented that, whenever possible, the patientshould be placed on the operative table <strong>in</strong> lateral decubitusposition dur<strong>in</strong>g the second or third trimester so as toavoid unnecessary compression <strong>of</strong> the <strong>in</strong>ferior vena cavaby the gravid uterus. 20 Other options <strong>in</strong>clude plac<strong>in</strong>g awedge under the right hip or tilt<strong>in</strong>g the operat<strong>in</strong>g table.<strong>The</strong> need for fetal monitor<strong>in</strong>g is generally answered by gestationalage and viability <strong>of</strong> the fetus. Fetal heart rate (FHR) monitor<strong>in</strong>gcan prove useful <strong>in</strong> identify<strong>in</strong>g <strong>in</strong>traoperative conditionscaus<strong>in</strong>g impairment <strong>in</strong> uteroplacental blood flow and thereforefetal oxygenation. 15 However, many obstetricians feel that<strong>in</strong>traoperative FHR monitor<strong>in</strong>g has little use because maternalderangements can be assessed and treated without it. 21 Also, ithas been shown that no change <strong>in</strong> fetal outcome has ever beenestablished through <strong>in</strong>traoperative FHR monitor<strong>in</strong>g. 22Consult!It is useful to consult obstetricians whenever there is uncerta<strong>in</strong>tyabout these matters and to consistently use a multidiscipl<strong>in</strong>aryapproach to patient care.November 2007 E161 E163
<strong>Orthopedic</strong> <strong>Trauma</strong> <strong>in</strong> <strong>Pregnancy</strong>Pa<strong>in</strong> ManagementDef<strong>in</strong>itive orthopedic fixation can result <strong>in</strong> significant postoperativeand <strong>in</strong>jury-associated pa<strong>in</strong>. It is common practiceto use narcotics and muscle relaxants <strong>in</strong> the immediateperioperative and postoperative periods to provide comfortto the patient. Naturally, pregnancy raises questions aboutuse <strong>of</strong> such medications.Goodman 21 claimed that perioperative opioid use shouldraise little concern about teratogenicity. <strong>The</strong> risk for neonaterespiratory depression is only pert<strong>in</strong>ent “if deliveryoccurs at the same time as the surgery.” Much <strong>of</strong> the literatureconcern<strong>in</strong>g opioids is <strong>in</strong> the sett<strong>in</strong>g <strong>of</strong> labor pa<strong>in</strong>.A recent systematic review <strong>of</strong> the literature suggested thatepidurals provide better pa<strong>in</strong> relief than systemic medication.However, meperid<strong>in</strong>e (Demerol) is the most commonlyused systemic opioid worldwide, and questions stillexist about its efficacy and side effect pr<strong>of</strong>ile. In addition,none <strong>of</strong> the studies compar<strong>in</strong>g pethid<strong>in</strong>e with other opioidshas been conv<strong>in</strong>c<strong>in</strong>g. 23<strong>The</strong>re are no reports associat<strong>in</strong>g muscle relaxants withteratogenicity. <strong>The</strong> positively charged depolariz<strong>in</strong>g and nondepolariz<strong>in</strong>gagents do not cross the placenta. 22 However,Hart 16 claimed that cyclobenzapr<strong>in</strong>e (Flexeril) is the “onlyknown safe muscle relaxant for use <strong>in</strong> pregnant women.”Nonsteroidal anti-<strong>in</strong>flammatory drugs are contra<strong>in</strong>dicatedbecause <strong>of</strong> their effects on the ductus arteriosus,and they can <strong>in</strong>hibit labor <strong>in</strong> the third trimester. From anorthopedic standpo<strong>in</strong>t, they have been repeatedly shown tobe deleterious to fracture union. <strong>The</strong>refore, acetam<strong>in</strong>ophenis recommended for m<strong>in</strong>or pa<strong>in</strong> relief.Gestational age plays a major role <strong>in</strong> determ<strong>in</strong><strong>in</strong>g whichmedications are safe dur<strong>in</strong>g each phase <strong>of</strong> fetal development.It is important to keep <strong>in</strong> m<strong>in</strong>d that medication risklabels can change dur<strong>in</strong>g a 9-month pregnancy, depend<strong>in</strong>gon the vulnerability <strong>of</strong> the fetus <strong>in</strong> any given trimester. 16“...medication risk labels canchange dur<strong>in</strong>g a 9-monthpregnancy, depend<strong>in</strong>g on thevulnerability <strong>of</strong> the fetus <strong>in</strong> anygiven trimester. 16 ”AnticoagulationVenous thromboembolic disease consists <strong>of</strong> deep venousthrombosis (DVT) and pulmonary embolism (PE). Estimatedannual <strong>in</strong>cidence <strong>in</strong> the general population is approximately0.1%. 24 This percentage is <strong>in</strong>creased 5- to 6-fold <strong>in</strong> pregnancy,as all 3 components <strong>of</strong> the Virchow triad can be found<strong>in</strong> pregnancy. 25 <strong>Orthopedic</strong> trauma, and subsequent operative<strong>in</strong>tervention, can necessitate vary<strong>in</strong>g periods <strong>of</strong> immobilization.Given the hypercoaguable state <strong>of</strong> pregnancy, anticoagulationbecomes a critical issue. In fact, untreated DVTshave been shown to lead to PEs <strong>in</strong> 16% <strong>of</strong> patients and havebecome the lead<strong>in</strong>g cause <strong>of</strong> maternal death. 26 Important riskfactors are listed <strong>in</strong> Table V. 27Choice <strong>of</strong> anticoagulant is <strong>of</strong> critical importance <strong>in</strong> pregnancy.Warfar<strong>in</strong> is known to cross the placenta and potentiallycause fetal bleed<strong>in</strong>g and teratogenicity. 28 Unfractionatedhepar<strong>in</strong> (UFH) has been classified a high-alert drug bythe Institute for Safe Medic<strong>in</strong>e <strong>Practice</strong>s because <strong>of</strong> thepharmacologic properties <strong>of</strong> the agent as well as the risk <strong>of</strong>medical errors <strong>in</strong> anticoagulation management us<strong>in</strong>g UFH.“...untreated DVTs have...become the lead<strong>in</strong>g cause <strong>of</strong>maternal death. 26 ”UFH is associated with hepar<strong>in</strong>-<strong>in</strong>duced thrombocytopenia(HIT), bleed<strong>in</strong>g, and osteopenia with long-term therapy. 29Accord<strong>in</strong>g to a study reported by Hawk<strong>in</strong>s and Evans, 303 <strong>of</strong> every 100 patients on long-term UFH therapy mayexperience symptomatic vertebral fractures, and 30% mayexperience a reduction <strong>in</strong> bone density lead<strong>in</strong>g to osteopeniaand/or osteoporosis.A clear alternative to UFH is low-molecular-weighthepar<strong>in</strong> (LMWH), which is associated with lower <strong>in</strong>cidence<strong>of</strong> HIT and osteoporosis. It is recommended that LMWHdos<strong>in</strong>g be closely monitored with the assistance <strong>of</strong> a pharmacistbecause <strong>of</strong> volume distribution changes encountered<strong>in</strong> pregnancy. 31 It is also recommended that treatment bestopped 24 hours before delivery to allow for safe epiduralanesthesia and to prevent excessive bleed<strong>in</strong>g. 28Another alternative is fondapar<strong>in</strong>ux, a synthetic antithromboticagent that specifically b<strong>in</strong>ds to antithromb<strong>in</strong>.Fondapar<strong>in</strong>ux has been shown to be as effective as LMWHwith respect to anticoagulation and to lack a negative effecton bone. 30Last, a more <strong>in</strong>vasive option is temporary placement <strong>of</strong><strong>in</strong>ferior vena cava filters. Kawamata and colleagues 32 recentlyfound that use <strong>of</strong> this practice <strong>in</strong> 11 patients produced nosymptomatic pulmonary thromboembolism dur<strong>in</strong>g or afterpregnancy. All filters were placed suprarenally and removedsuccessfully, and there were no reported complications.Pelvic and Acetabular <strong>Trauma</strong>In 1980, Golan and colleagues 33 exam<strong>in</strong>ed a series <strong>of</strong> 15patients who susta<strong>in</strong>ed trauma <strong>in</strong> late pregnancy. Five <strong>of</strong>the 15 susta<strong>in</strong>ed pelvic fractures, with the most commonpattern <strong>in</strong>volv<strong>in</strong>g the pubic rami. In this study, fetal outcomeswere mixed, with 2 <strong>of</strong> 5 babies surviv<strong>in</strong>g, 2 deathsoccurr<strong>in</strong>g <strong>in</strong> utero secondary to placental abruption, and 1death occurr<strong>in</strong>g secondary to uter<strong>in</strong>e rupture. However, <strong>of</strong>significance is that the 2 live births, though premature, weredelivered vag<strong>in</strong>ally without adverse events. Authors <strong>of</strong>more recent case reports have described open reduction and<strong>in</strong>ternal fixation <strong>of</strong> acetabular fractures <strong>in</strong> this sett<strong>in</strong>g withgood outcomes. 34,35 Dunlop and colleagues 36 chronicledE164 E162 <strong>The</strong> American <strong>Journal</strong> <strong>of</strong> <strong>Orthopedic</strong>s ®
P. Desai and M. Sukoperative treatment <strong>of</strong> a female 24 weeks pregnant with acomm<strong>in</strong>uted transverse and posterior wall acetabular fracture.<strong>The</strong> patient suffered no adverse outcomes to the fetus,delivered vag<strong>in</strong>ally at 39 weeks, and was weight-bear<strong>in</strong>g 12weeks after surgery. However, the authors stated, “Whilewe would not recommend that all pregnant patients withacetabular fractures should undergo open reduction <strong>in</strong>ternalfixation, it is an option … that should be <strong>of</strong>fered.” Kloenand colleagues 20 also reported that complex acetabularfractures can be treated operatively and uneventfully andresult <strong>in</strong> vag<strong>in</strong>al childbirth.In general, all patients should be counseled about therisks and benefits <strong>of</strong> their surgery. However, <strong>in</strong> pregnantpatients, additional considerations apply.In a retrospective follow-up <strong>of</strong> 7 patients with pelvicfractures <strong>in</strong> pregnancy, Pape and colleagues 37 found that 2<strong>of</strong> 3 mothers with surviv<strong>in</strong>g fetuses had modifications tothe treatment <strong>of</strong> their pelvic <strong>in</strong>juries <strong>in</strong> the <strong>in</strong>terest <strong>of</strong> fetalwell-be<strong>in</strong>g. One patient with an anterior column posteriorhemitransverse fracture pattern was not eligible for surgerybecause <strong>of</strong> coagulopathy <strong>in</strong>duced by amniotic fluid. Shewas treated nonoperatively and went on to uneventful heal<strong>in</strong>gand full weight-bear<strong>in</strong>g. <strong>The</strong> second patient had multipleorthopedic <strong>in</strong>juries, <strong>in</strong>clud<strong>in</strong>g unilateral zone 2 sacrumfractures and ipsilateral anterior pelvic r<strong>in</strong>g fractures. Sheunderwent operative treatment <strong>of</strong> bilateral open femur fractures,and the pelvic r<strong>in</strong>g <strong>in</strong>jury was treated with an externalfixator because <strong>of</strong> concerns about excessive ioniz<strong>in</strong>g radiation.Last, Leggon and colleagues 38 reviewed the literatureon pelvic and acetabular fractures (N = 101), found thatthese <strong>in</strong>juries were associated with a higher mortality rateamong fetuses (35%) than mothers (9%), and concludedthat mechanism <strong>of</strong> <strong>in</strong>jury and <strong>in</strong>jury severity <strong>in</strong>fluencedmortality, whereas fracture classification, fracture type,pregnancy trimester, and era <strong>of</strong> reviewed literature did notcorrelate with mortality.Clearly, there are multiple approaches to treat<strong>in</strong>g a pregnantpatient. Care must be taken to evaluate the well-be<strong>in</strong>g<strong>of</strong> the mother and the fetus to optimize outcomes. Whetherto provide operative versus nonoperative treatment <strong>of</strong>pelvic and acetabular fractures appears to h<strong>in</strong>ge more on<strong>in</strong>jury severity and patient stability than on the nature <strong>of</strong> theorthopedic <strong>in</strong>jury itself. Loegters and colleagues 39 stated,“Surgical treatment <strong>of</strong> an unstable fracture <strong>of</strong> the pelvicr<strong>in</strong>g dur<strong>in</strong>g pregnancy is possible with a justifiable risk tothe mother and child.” We add that surgical treatment <strong>of</strong>these <strong>in</strong>juries is a reasonable option for pregnant patientsto allow for anatomical reduction and <strong>in</strong>creased heal<strong>in</strong>gpotential while keep<strong>in</strong>g term vag<strong>in</strong>al delivery as an option.ConclusionsTreatment <strong>of</strong> the pregnant orthopedic trauma patient generatesmany questions and raises many uncerta<strong>in</strong>ties <strong>in</strong> management.After review<strong>in</strong>g much <strong>of</strong> the up-to-date literature,we can recommend a safe approach to orthopedic surgery<strong>in</strong> the pregnant patient with confidence.Accord<strong>in</strong>g to our f<strong>in</strong>d<strong>in</strong>gs, there is m<strong>in</strong>imal radiation risk<strong>in</strong> obta<strong>in</strong><strong>in</strong>g x-rays for operative plann<strong>in</strong>g, provided thatthe cumulative dose is with<strong>in</strong> 5 rad. Also, safety concernsregard<strong>in</strong>g patient position<strong>in</strong>g and staff radiation exposureshould be taken <strong>in</strong>to consideration.In addition, we found that most anesthetics <strong>in</strong> pregnancyare category C and therefore safe. Perioperative opioiduse for pa<strong>in</strong> management is recommended with little risk.LMWH and fondapar<strong>in</strong>ux are the safest choices for anticoagulation.Last, pregnancy is not a contra<strong>in</strong>dication tooperative management <strong>of</strong> pelvic and acetabular fractures.It is clear that educat<strong>in</strong>g the medical community as wellas the patient about the potential risks and misconceptionsregard<strong>in</strong>g surgery <strong>in</strong> pregnancy will decrease the uncerta<strong>in</strong>tyand anxiety surround<strong>in</strong>g this patient population.Authors’ Disclosure Statement<strong>The</strong> authors report no actual or potential conflict <strong>of</strong> <strong>in</strong>terest<strong>in</strong> relation to this article.References1. Heckman JD, Sassard R. Current concepts review: musculoskeletal considerations<strong>in</strong> pregnancy. J Bone Jo<strong>in</strong>t Surg Am. 1994;76(11):1720-1730.2. Ritchie JR. Orthopaedic considerations dur<strong>in</strong>g pregnancy. Cl<strong>in</strong> ObstetGynecol. 2003;46(2):456-466.3. De Santis M, Di Gianantonio E, Straface G, et al. Ioniz<strong>in</strong>g radiations <strong>in</strong>pregnancy and teratogenesis: a review <strong>of</strong> literature. Reprod Toxicol.2005;20(3):323-329.4. Savithiri R, Bona N, Chandra K, Koren G. Physicians’ perceptions <strong>of</strong> teratogenicrisk associated with radiography and CT dur<strong>in</strong>g early pregnancy. AJRAm J Roentgenol. 2004;182(5):1107-1109.5. ACOG Committee on Obstetric <strong>Practice</strong>. ACOG Committee Op<strong>in</strong>ion.Number 299, September 2004 (replaces No. 158, September 1995).Guidel<strong>in</strong>es for diagnostic imag<strong>in</strong>g dur<strong>in</strong>g pregnancy. Obstet Gynecol.2004;104(3):647-651.6. Brent RL. <strong>The</strong> effects <strong>of</strong> embryonic and fetal exposure to x-ray, microwaves,and ultrasound. Cl<strong>in</strong> Per<strong>in</strong>atol. 1986;13(3):615-648.7. Parry RA, Glaze SA, Archer BR. <strong>The</strong> AAPM/RSNA physics tutorialfor residents. Typical patient radiation doses <strong>in</strong> diagnostic radiology.Radiographics. 1999;19(5):1289-1302.8. De Wilde JP, Rivers AW, Price DL. A review <strong>of</strong> the current use <strong>of</strong> magneticresonance imag<strong>in</strong>g <strong>in</strong> pregnancy and safety implications for the fetus. ProgBiophys Mol Biol. 2005;87(2-3):335-353.9. Burrow G, Hamilton H, Hrubec Z, et al. Study <strong>of</strong> adolescents exposed <strong>in</strong>utero to the atomic bomb, Nagasaki, Japan. I. General aspects: cl<strong>in</strong>icallaboratory data. Yale J Biol Med. 1964;36:430-444.10. Hosh<strong>in</strong>o T, Itoga T, Kato H. Leukemia <strong>in</strong> the <strong>of</strong>fspr<strong>in</strong>g <strong>of</strong> parents exposed tothe atomic bomb at Hiroshima and Nagasaki. Paper presented at: Meet<strong>in</strong>g<strong>of</strong> the Japanese Association <strong>of</strong> Hematology; March 28-30, 1965.11. Naumburg E, Bellocco R, Cnatt<strong>in</strong>gius S, Hall P, Boice JD Jr, Ekbom A.Intrauter<strong>in</strong>e exposure to diagnostic x-rays and risk <strong>of</strong> childhood leukemiasubtypes. Radiat Res. 2001;156(6):718-723.12. Ohtaki K, Kodama Y, Nakano M, et al. Human fetuses do not registerchromosome damage <strong>in</strong>flicted by radiation exposure <strong>in</strong> lymphoid precursorcells except for a small but significant effect at low doses. Radiat Res.2004;161(4):373-379.13. Statkiewicz Shearer MA. Radiation Protection <strong>in</strong> Medical Radiography. St.Louis, MO: Mosby; 2002.14. <strong>The</strong>ocharopoulos N, Damilakis J, Peris<strong>in</strong>akis K, Papadokostakis G,Hadjipavlou A, Gourtsoyiannis N. Image-guided reconstruction <strong>of</strong> femoralfractures: is the staff progeny safe? Cl<strong>in</strong> Orthop. 2005;(430):182-188.15. Kuczkowski K. Nonobstetric surgery dur<strong>in</strong>g pregnancy: what are the risks<strong>of</strong> anesthesia? Obstet Gynecol Surv. 2003;59(1):52-56.16. Hart MA. Help! My orthopaedic patient is pregnant! Orthop Nurs.2005;24(2):108-114.17. Melnick DM, Wahl W, Dalton VK. Management <strong>of</strong> general surgical problems<strong>in</strong> the pregnant patient. Am J Surg. 2004;187(2):170-180.18. Mazze R, Kallen B. Reproductive outcome after anesthesia and operationdur<strong>in</strong>g pregnancy: a registry study <strong>of</strong> 5405 cases. Am J Obstet Gynecol.1989;161(5):1178-1185.November 2007 E161 E165
<strong>Orthopedic</strong> <strong>Trauma</strong> <strong>in</strong> <strong>Pregnancy</strong>19. Rosen MA. Management <strong>of</strong> anesthesia for the pregnant surgical patient.Anesthesiology. 1999;91(4):1159-1163.20. Kloen P, Flik K, Helfet DL. Operative treatment <strong>of</strong> acetabular fracture dur<strong>in</strong>gpregnancy: a case report. Arch Orthop <strong>Trauma</strong> Surg. 2005;125(3):209-212.21. Goodman S. Anesthesia for nonobstetric surgery <strong>in</strong> the pregnant patient.Sem<strong>in</strong> Per<strong>in</strong>atol. 2002;26(2):136-145.22. Horrigan TJ, Villarreal R, We<strong>in</strong>ste<strong>in</strong> L. Are obstetrical personnel requiredfor <strong>in</strong>traoperative fetal monitor<strong>in</strong>g dur<strong>in</strong>g nonobstetric surgery? J Per<strong>in</strong>atol.1999;19(2):124-126.23. Bricker L, Lavender T. Parenteral opioids for labor pa<strong>in</strong> relief: a systemicreview. Am J Obstet Gynecol. 2002;186(5 suppl):S94-S109.24. White RH. <strong>The</strong> epidemiology <strong>of</strong> venous thromboembolism. Circulation.2003;107(suppl I):I4-I8.25. Doyle NM, Monga M. Thromboembolic disease <strong>in</strong> pregnancy. ObstetGynecol Cl<strong>in</strong> North Am. 2004;31(2):319-344.26. Greer IA. <strong>The</strong> challenge <strong>of</strong> thrombophilia <strong>in</strong> maternal–fetal medic<strong>in</strong>e. N EnglJ Med. 2000;342(6):424-425.27. Robertson L, Greer I. Thromboembolism <strong>in</strong> pregnancy. Curr Op<strong>in</strong> ObstetGynecol. 2005;17(2):113-116.28. McRae SJ, G<strong>in</strong>sberg JS. Initial treatment <strong>of</strong> venous thromboembolism.Circulation. 2004;110(suppl I):I3-I9.29. Niccolai CS, Hicks RW, Oertel L, Francis JL; Hepar<strong>in</strong> Consensus Group.Unfractionated hepar<strong>in</strong>: focus on high-alert drug. Pharmacotherapy.2004;24(8 pt 2):146S-155S.30. Hawk<strong>in</strong>s D, Evans J. M<strong>in</strong>imis<strong>in</strong>g the risk <strong>of</strong> hepar<strong>in</strong>-<strong>in</strong>duced osteoporosisdur<strong>in</strong>g pregnancy. Expert Op<strong>in</strong> Drug Saf. 2005;4(3):583-590.31. G<strong>in</strong>sberg JS, Bates SM. Management <strong>of</strong> venous thromboembolism dur<strong>in</strong>gpregnancy. J Thromb Haemost. 2003;1(7):1435-1442.32. Kawamata K, Chiba Y, Tanaka R, Higashi M, Nishigami K. Experience <strong>of</strong>temporary <strong>in</strong>ferior vena cava filters <strong>in</strong>serted <strong>in</strong> the per<strong>in</strong>atal period to preventpulmonary embolism <strong>in</strong> pregnant women with deep ve<strong>in</strong> thrombosis. J VascSurg. 2005;41(4):652-656.33. Golan A, Sandbank O, Teare AJ. <strong>Trauma</strong> <strong>in</strong> late pregnancy. S Afr Med J.1980;57(5):161-165.34. Pals SD, Brown CW, Friermood TG. Open reduction <strong>in</strong>ternal fixation <strong>of</strong> anacetabular fracture dur<strong>in</strong>g pregnancy. J Orthop <strong>Trauma</strong>. 1992;6(3):379-381.35. Yosipovitch Z, Goldberg I, Ventura E, Neri A. Open reduction <strong>of</strong> acetabularfracture <strong>in</strong> pregnancy. A case report. Cl<strong>in</strong> Orthop. 1992;(282):229-232.36. Dunlop DJ, McCahill JP, Blakemore ME. Internal fixation <strong>of</strong> an acetabularfracture dur<strong>in</strong>g pregnancy. Injury. 1997;28(7):481-482.37. Pape, HC, Pohlemann T, Gansslen A, et al. Pelvic fractures <strong>in</strong> pregnantmultiple trauma patients. J Orthop <strong>Trauma</strong>. 2000;14(4):238-244.38. Leggon RE, Wood GS, Indeck MC. Pelvic fractures <strong>in</strong> pregnancy: factors<strong>in</strong>fluenc<strong>in</strong>g maternal and fetal outcomes. J <strong>Trauma</strong>. 2002;53(4):796-804.39. Loegters T, Briem D, Gatzka C, et al. Treatment <strong>of</strong> unstable fractures<strong>of</strong> the pelvic r<strong>in</strong>g <strong>in</strong> pregnancy. Arch Orthop <strong>Trauma</strong> Surg.2005;125(3):204-208.This paper will be judged for the Resident Writer’s Award.E166 E162 <strong>The</strong> American <strong>Journal</strong> <strong>of</strong> <strong>Orthopedic</strong>s ®