Form A: diabetes and nutrition history - St. Anthony's Medical Center
Form A: diabetes and nutrition history - St. Anthony's Medical Center
Form A: diabetes and nutrition history - St. Anthony's Medical Center
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
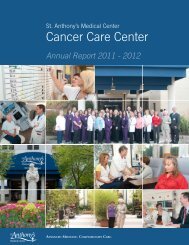
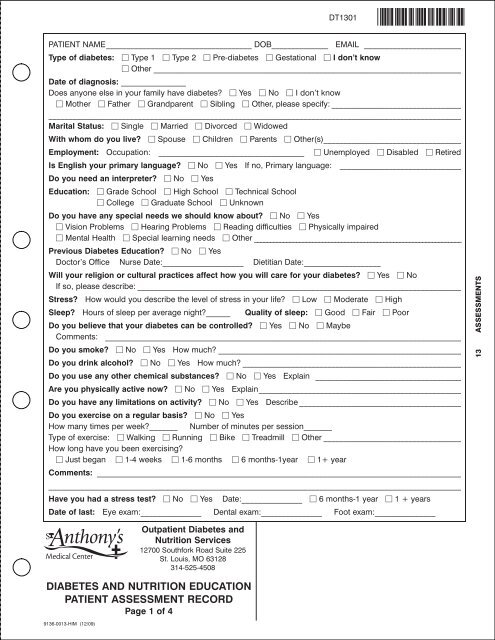
DT1301PATIENT NAME____________________________________ DOB______________ EMAIL ________________________Type of <strong>diabetes</strong>: Type 1 Type 2 Pre-<strong>diabetes</strong> Gestational I don’t know Other ____________________________________________________________________________Date of diagnosis: ________________Does anyone else in your family have <strong>diabetes</strong>? Yes No I don’t know Mother Father Gr<strong>and</strong>parent Sibling Other, please specify: ______________________________________________________________________________________________________________________________________Marital <strong>St</strong>atus: Single Married Divorced WidowedWith whom do you live? Spouse Children Parents Other(s)__________________________________Employment: Occupation: ____________________________________ Unemployed Disabled RetiredIs English your primary language? No Yes If no, Primary language: ______________________________Do you need an interpreter? No YesEducation: Grade School High School Technical School College Graduate School UnknownDo you have any special needs we should know about? No Yes Vision Problems Hearing Problems Reading difficulties Physically impaired Mental Health Special learning needs Other ________________________________________________________________Previous Diabetes Education? No YesDoctor’s Office Nurse Date:____________________ Dietitian Date:___________________Will your religion or cultural practices affect how you will care for your <strong>diabetes</strong>? Yes NoIf so, please describe: ________________________________________________________________________________<strong>St</strong>ress? How would you describe the level of stress in your life? Low Moderate HighSleep? Hours of sleep per average night?______ Quality of sleep: Good Fair PoorDo you believe that your <strong>diabetes</strong> can be controlled? Yes No MaybeComments: ________________________________________________________________________________________Do you smoke? No Yes How much? ____________________________________________________________Do you drink alcohol? No Yes How much? ______________________________________________________Do you use any other chemical substances? No Yes Explain ____________________________________Are you physically active now? No Yes Explain__________________________________________________Do you have any limitations on activity? No Yes Describe ________________________________________Do you exercise on a regular basis? No YesHow many times per week?_______ Number of minutes per session_______Type of exercise: Walking Running Bike Treadmill Other __________________________________How long have you been exercising? Just began 1-4 weeks 1-6 months 6 months-1year 1+ yearComments: ________________________________________________________________________________________________________________________________________________________________________________________________Have you had a stress test? No Yes Date:_______________ 6 months-1 year 1 + yearsDate of last: Eye exam:_______________ Dental exam:_______________ Foot exam:_______________13 ASSESSMENTSDIABETES AND NUTRITION EDUCATIONPATIENT ASSESSMENT RECORDPage 1 of 49136-0013-HIM (12/09)Outpatient Diabetes <strong>and</strong>Nutrition Services12700 Southfork Road Suite 225<strong>St</strong>. Louis, MO 63128314-525-4508
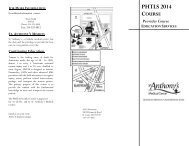
Do you check your blood sugar? Yes No If yes, what meter do you use? __________________________When? ______________________________________________________________________________________________How Often? More than once/day Several times/week Less than once/week____________________________________________________________________________________________________________________________________________________________________________________________________________Have you had symptoms of high blood sugar? Yes No I don’t know If yes, please check below. Extreme Thirst Frequent urination Blurred vision Drowsiness Other: __________________________________________________________________________________________________________________________________________________________________________________________________________________________________Have you had symptoms of low blood sugar? Yes No I don’t know If yes, please check below. Shakiness Fast Heartbeat Sweating Lightheadedness Other: ____________________________If yes, how often? More than once a week Once a month More than once a month Less than once a yearDo symptoms occur at specific times? Yes No____________________________________________________________________________________________________________________________________________________________________________________________________________If you take insulin, please answer the following:Type of Insulin Time Taken Amount_________________________________________________ ____________________ ___________________________________________________________________ ____________________ ___________________________________________________________________ ____________________ __________________What type of injection device do you use? syringe pen pump inhalerDo you have an insulin-to-carbohydrate ratio? No Yes:________ units per _______gmDo you take extra insulin if your blood sugar is high before a meal or at other times? No Yes If yes, please complete the chart on right.Where to you inject your insulin? <strong>St</strong>omach Arm Leg ButtocksWhere do you store the insulin that you are now using?__________________________Where do you store unopened insulin?_________________________________________Where do you dispose of your needle/lancets/syringes?__________________________Do you wear a medical alert? Yes NoBlood Glucose + Insulin__________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________DIABETES AND NUTRITION EDUCATIONPATIENT ASSESSMENT RECORDPage 2 of 49136-0013-HIM (12/09)Outpatient Diabetes <strong>and</strong>Nutrition Services12700 Southfork Road Suite 225<strong>St</strong>. Louis, MO 63128314-525-4508
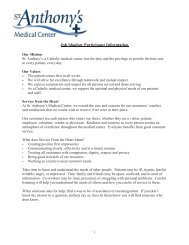
DT1301Please list any medications including vitamins <strong>and</strong> nonprescription items. Or we will copy your list.Name Name Name________________________________ ________________________________ ________________________________________________________________ ________________________________ ________________________________________________________________ ________________________________ ________________________________________________________________ ________________________________ ________________________________HEALTH HISTORY (Check all of the following that apply): Allergies _____________ Arthritis Bloating Cancer ______________ Celiac Disease Circulation problems Constipation Crohn’s Disease Diabetes duringpregnancy Diarrhea Diverticulitis Erectile dysfunction Eye problems Heart disease Hiatal hernia High blood pressure High cholesterol/triglycerides Kidney problems Liver problems Loss of feeling/tinglingin h<strong>and</strong>s & feet Mental health problems Respiratory problems Sleep problems <strong>St</strong>roke Thyroid problems Other ____________________________________________________________Please list any significant hospitalizations:Date: ____________ Description:________________________________________________________________________Date: ____________ Description:________________________________________________________________________Are you planning on becoming pregnant in the near future? N/A Yes NoOther/Comments regarding medical <strong>history</strong>:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Date of next appointment with your doctor:____________________Height ____________Weight ____________ Most weight? ____________ Desired weight? ____________Has your weight changed in the past three months? Yes NoIf yes, I’ve Lost Gained ________ poundsWho cooks meals?________________________________Who grocery shops?________________________________Usual number of meals/day _____________ snacks _____________How many times a week do you eat out or buy carry outs? _____________List any food allergies or intolerances: ________________________________________________________________LIST FOOD AND/OR BEVERAGES YOU HAVE EATEN IN THE LAST 24 HOURS:13 ASSESSMENTSBreakfast/Time:____________ Lunch/Time:____________ Dinner/Time:____________Snacks/Time:____________ Snacks/Time:____________ Snacks/Time:____________Patient Signature:_____________________________________________ Date_______________ Time_______________DIABETES AND NUTRITION EDUCATIONPATIENT ASSESSMENT RECORDPage 3 of 49136-0013-HIM (12/09)Outpatient Diabetes <strong>and</strong>Nutrition Services12700 Southfork Road Suite 225<strong>St</strong>. Louis, MO 63128314-525-4508
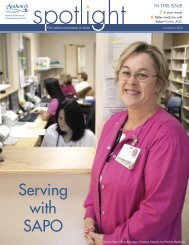
MilkMeatCheeseEggsFruitsJuicesNon-<strong>St</strong>archy Vegetables<strong>St</strong>archesWhole GrainsFatsDesserts/SweetsSugar/Sugar SubstitutesSnack FoodsSodas/Sweetened BeveragesWaterAlcoholBELOW IS FOR OFFICE USE ONLYDay Week TypeEducator Comments/Notes: ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________<strong>Form</strong> Reviewed by: Educator Name:________________________________Reviewed by: Educator Name: ____________________________________Initials:_________ Date:_______________Initials:_________ Date:_______________DIABETES AND NUTRITION EDUCATIONPATIENT ASSESSMENT RECORDPage 4 of 49136-0013-HIM (12/09)Outpatient Diabetes <strong>and</strong>Nutrition Services12700 Southfork Road Suite 225<strong>St</strong>. Louis, MO 63128314-525-4508