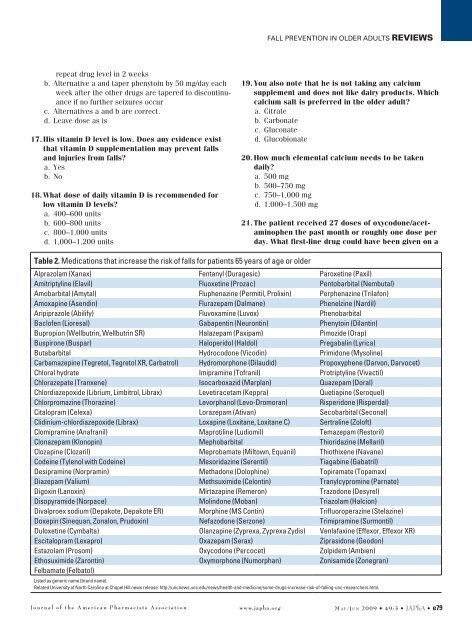
<strong>Fall</strong> prevention <strong>in</strong> older adults Reviewsrepeat drug level <strong>in</strong> 2 weeksb. Alternative a and taper phenyto<strong>in</strong> by 50 mg/day eachweek after <strong>the</strong> o<strong>the</strong>r drugs are tapered to discont<strong>in</strong>uanceif no fur<strong>the</strong>r seizures occurc. Alternatives a and b are correct.d. Leave dose as is17. His vitam<strong>in</strong> D level is low. Does any evidence existthat vitam<strong>in</strong> D supplementation may prevent fallsand <strong>in</strong>juries from falls?a. Yesb. No18. What dose of daily vitam<strong>in</strong> D is recommended <strong>for</strong>low vitam<strong>in</strong> D levels?a. 400–600 unitsb. 600–800 unitsc. 800–1,000 unitsd. 1,000–1,200 units19. You also note that he is not tak<strong>in</strong>g any calciumsupplement and does not like dairy products. Whichcalcium salt is preferred <strong>in</strong> <strong>the</strong> older adult?a. Citrateb. Carbonatec. Gluconated. Glucobionate20. How much elemental calcium needs to be takendaily?a. 500 mgb. 500–750 mgc. 750–1,000 mgd. 1,000–1,500 mg21. The patient received 27 doses of oxycodone/acetam<strong>in</strong>ophen<strong>the</strong> past month or roughly one dose perday. What first-l<strong>in</strong>e drug could have been given on aTable 2. <strong>Medication</strong>s that <strong>in</strong>crease <strong>the</strong> risk of falls <strong>for</strong> patients 65 years of age or olderAlprazolam (Xanax) Fentanyl (Duragesic) Paroxet<strong>in</strong>e (Paxil)Amitriptyl<strong>in</strong>e (Elavil) Fluoxet<strong>in</strong>e (Prozac) Pentobarbital (Nembutal)Amobarbital (Amytal) Fluphenaz<strong>in</strong>e (Permitil, Prolix<strong>in</strong>) Perphenaz<strong>in</strong>e (Trilafon)Amoxap<strong>in</strong>e (Asend<strong>in</strong>) Flurazepam (Dalmane) Phenelz<strong>in</strong>e (Nardil)Aripiprazole (Abilify) Fluvoxam<strong>in</strong>e (Luvox) PhenobarbitalBaclofen (Lioresal) Gabapent<strong>in</strong> (Neuront<strong>in</strong>) Phenyto<strong>in</strong> (Dilant<strong>in</strong>)Bupropion (Wellbutr<strong>in</strong>, Wellbutr<strong>in</strong> SR) Halazepam (Paxipam) Pimozide (Orap)Buspirone (Buspar) Haloperidol (Haldol) Pregabal<strong>in</strong> (Lyrica)Butabarbital Hydrocodone (Vicod<strong>in</strong>) Primidone (Mysol<strong>in</strong>e)Carbamazep<strong>in</strong>e (Tegretol, Tegretol XR, Carbatrol) Hydromorphone (Dilaudid) Propoxyphene (Darvon, Darvocet)Chloral hydrate Imipram<strong>in</strong>e (Tofranil) Protriptyl<strong>in</strong>e (Vivactil)Chlorazepate (Tranxene) Isocarboxazid (Marplan) Quazepam (Doral)Chlordiazepoxide (Librium, Limbitrol, Librax) Levetiracetam (Keppra) Quetiap<strong>in</strong>e (Seroquel)Chlorpromaz<strong>in</strong>e (Thoraz<strong>in</strong>e) Levorphanol (Levo-Dromoran) Risperidone (Risperdal)Citalopram (Celexa) Lorazepam (Ativan) Secobarbital (Seconal)Clid<strong>in</strong>ium-chlordiazepoxide (Librax) Loxap<strong>in</strong>e (Loxitane, Loxitane C) Sertral<strong>in</strong>e (Zoloft)Clomipram<strong>in</strong>e (Anafranil) Maprotil<strong>in</strong>e (Ludiomil) Temazepam (Restoril)Clonazepam (Klonop<strong>in</strong>) Mephobarbital Thioridaz<strong>in</strong>e (Mellaril)Clozap<strong>in</strong>e (Clozaril) Meprobamate (Miltown, Equanil) Thiothixene (Navane)Code<strong>in</strong>e (Tylenol with Code<strong>in</strong>e) Mesoridaz<strong>in</strong>e (Serentil) Tiagab<strong>in</strong>e (Gabatril)Desipram<strong>in</strong>e (Norpram<strong>in</strong>) Methadone (Doloph<strong>in</strong>e) Topiramate (Topamax)Diazepam (Valium) Methsuximide (Celont<strong>in</strong>) Tranylcyprom<strong>in</strong>e (Parnate)Digox<strong>in</strong> (Lanox<strong>in</strong>) Mirtazap<strong>in</strong>e (Remeron) Trazodone (Desyrel)Disopyramide (Norpace) Mol<strong>in</strong>done (Moban) Triazolam (Halcion)Divalproex sodium (Depakote, Depakote ER) Morph<strong>in</strong>e (MS Cont<strong>in</strong>) Trifluoroperaz<strong>in</strong>e (Stelaz<strong>in</strong>e)Doxep<strong>in</strong> (S<strong>in</strong>equan, Zonalon, Prudox<strong>in</strong>) Nefazodone (Serzone) Trimipram<strong>in</strong>e (Surmontil)Duloxet<strong>in</strong>e (Cymbalta) Olanzap<strong>in</strong>e (Zyprexa, Zyprexa Zydis) Venlafax<strong>in</strong>e (Effexor, Effexor XR)Escitalopram (Lexapro) Oxazepam (Serax) Ziprasidone (Geodon)Estazolam (Prosom) Oxycodone (Percocet) Zolpidem (Ambien)Ethosuximide (Zaront<strong>in</strong>) Oxymorphone (Numorphan) Zonisamide (Zonegran)Felbamate (Felbatol)Listed as generic name (brand name).Related University of North Carol<strong>in</strong>a at Chapel Hill news release: http://uncnews.unc.edu/news/health-and-medic<strong>in</strong>e/some-drugs-<strong>in</strong>crease-risk-of-fall<strong>in</strong>g-unc-researchers.html.Journal of <strong>the</strong> American Pharmacists Association www.japha.org M a y /Ju n 2009 • 49:3 • JAPhA • e79
Reviews <strong>Fall</strong> prevention <strong>in</strong> older adultsregular basis to possibly decrease <strong>the</strong> need <strong>for</strong> <strong>the</strong>oxycodone?a. Acetam<strong>in</strong>ophenb. Propoxyphenec. Tramadold. Alternative a and topical NSAID22. What laxative may need to be given on a regularbasis <strong>for</strong> this patient to decrease <strong>the</strong> need <strong>for</strong> enemas?a. Fiberb. PEGc. Sorbitold. Alternative b or c is correct.23. What drug may need to be added to prevent occultgastro<strong>in</strong>test<strong>in</strong>al bleed<strong>in</strong>g from <strong>the</strong> ASA?a. Antacidsb. H 2blockersc. A PPId. None of <strong>the</strong> above alternatives is effective <strong>in</strong> decreas<strong>in</strong>gASA bleed<strong>in</strong>g.Answer key: 11–13. d; 14. c; 15. d; 16. c; 17. a; 18. d; 19. a; 20.d; 21. a; 22. d; 23. cCase discussion. This patient illustrates <strong>the</strong> complexity ofan older patient’s drug regimen and <strong>the</strong> sequence of eventsthat can occur. This patient was be<strong>in</strong>g treated by five differentphysicians dur<strong>in</strong>g <strong>the</strong> course of his home care, assisted-liv<strong>in</strong>gplacement, and subsequent nurs<strong>in</strong>g home placement. Afterreview<strong>in</strong>g <strong>the</strong> prescrib<strong>in</strong>g sequence, dates, and suspected adversedrug events that occurred <strong>in</strong> this patient, <strong>the</strong> pharmacistcan discuss <strong>the</strong>se f<strong>in</strong>d<strong>in</strong>gs with <strong>the</strong> attend<strong>in</strong>g prescribers andhopefully ensure that <strong>the</strong> primary care cl<strong>in</strong>ician is knowledgeableabout and agrees with <strong>the</strong> changes suggested. This team<strong>in</strong>tervention can improve <strong>the</strong> quality of <strong>the</strong> patient’s overallhealth care. Careful taper<strong>in</strong>g to discont<strong>in</strong>uance or lower doseof <strong>the</strong> medications that contributed to falls and fracture risk(antipsychotics, oxycodone and phenyto<strong>in</strong>, and memant<strong>in</strong>e)is appropriate <strong>in</strong> this patient. His seizures were attributed tohis stroke, use of <strong>the</strong> CNS stimulant methylphenidate, and ahigher dose of memant<strong>in</strong>e that was subsequently decreasedbecause of his renal function. He had some suspected seizureactivity at phenyto<strong>in</strong> 100 mg, and his dose was <strong>in</strong>creased backto 150 mg/day. His cognitive impairment was ascribed to <strong>the</strong>total psychoactive load, especially olanzap<strong>in</strong>e, quetiap<strong>in</strong>e, andoxycodone and phenyto<strong>in</strong> toxicity. His anemia was thought toresult from a history of GERD and tak<strong>in</strong>g ASA without gastroprotection,and a PPI was added. His constipation was consideredto result from <strong>in</strong>adequate fluid <strong>in</strong>take, <strong>the</strong> antipsychotics,and oxycodone, and a PEG laxative was started. His daytimesleep<strong>in</strong>g and nighttime <strong>in</strong>somnia were considered to becaused by <strong>the</strong> adverse drug reaction sequence of <strong>the</strong> olanzap<strong>in</strong>elead<strong>in</strong>g to oversedation, <strong>the</strong>n methylphenidate was startedto “perk him up” accord<strong>in</strong>g to one prescriber, which led to <strong>the</strong>need <strong>for</strong> quetiap<strong>in</strong>e from ano<strong>the</strong>r prescriber tak<strong>in</strong>g call over<strong>the</strong> weekend. All of <strong>the</strong> mentioned medication changes haveled to an improvement <strong>in</strong> his cognition (he now recognizesfamily and friends), constipation (no impactions, <strong>for</strong>med stooldaily), anemia (Hb 12.8 g/dL), and phenyto<strong>in</strong> (8 µg/mL), andno falls or seizures have occurred on <strong>the</strong> follow<strong>in</strong>g regimen:Activity. The patient was up on a walker with assistance threetimes a day, be<strong>for</strong>e meals, and be<strong>for</strong>e bed, was not napp<strong>in</strong>gmore than 15 to 20 m<strong>in</strong>utes after meals, and was engag<strong>in</strong>g <strong>in</strong>craft activities <strong>in</strong> <strong>the</strong> morn<strong>in</strong>g and afternoon. He was us<strong>in</strong>g abedside ur<strong>in</strong>al and shav<strong>in</strong>g and shower<strong>in</strong>g daily.<strong>Medication</strong>s. Acetam<strong>in</strong>ophen 500 mg was given every 4 hours(6:00 am, 10:00 am, 2:00 pm, 6:00 pm, and 10:00 pm), and<strong>the</strong> patient could have a sixth dose as a “sleep aid” if he awokedur<strong>in</strong>g <strong>the</strong> night no sooner than 2:00 am; 5% ketoprofen gelwas applied <strong>in</strong> “pencil eraser size” to knees and shoulderstwice daily.■■ PEG powder (Miralax): one capful with full glass of waterevery morn<strong>in</strong>g■■ Memant<strong>in</strong>e: 10 mg every morn<strong>in</strong>g■■ Phenyto<strong>in</strong>: 150 mg daily at bedtime■■ASA: 81 mg daily■■ Iron sulfate: 325 mg with ascorbic acid 500 mg everymorn<strong>in</strong>g■■ Calcium citrate: 630 mg with vitam<strong>in</strong> D 400 units withTable 3. Key po<strong>in</strong>ts of current article assess<strong>in</strong>g fall prevention <strong>in</strong> older adult patients 1–54Multifactorial risk assessment is a helpful tool to evaluate fall risk.Psychoactive/psychotropic polypharmacy greatly <strong>in</strong>creases fall risk; carefully <strong>in</strong>ventory and reduce, taper, and/or discont<strong>in</strong>ue medicationsthat may be associated with falls and that do not cause adverse drug withdrawal events.Do not abruptly stop medications; taper<strong>in</strong>g doses drug by drug, one at a time is recommended. A rule of thumb is 10%–25% of <strong>the</strong> daily doseevery week to 2 weeks depend<strong>in</strong>g on <strong>the</strong> half-life of <strong>the</strong> drug. The longer <strong>the</strong> half-life, <strong>the</strong> longer <strong>the</strong> taper<strong>in</strong>g period may be (e.g., diazepamand fluoxet<strong>in</strong>e have half-lives of <strong>the</strong> parent drug and active metabolite that exceed 150 hours). 49Consider PRN medications as a possible cause if a fall occurred with<strong>in</strong> 1 week of use and <strong>the</strong> medications were longer-act<strong>in</strong>g BZs (e.g.,diazepam) or antipsychotics.OBRA ‘90 mandates two to three taper<strong>in</strong>g attempts of anxiolytics and antipsychotics with<strong>in</strong> <strong>the</strong> first 6–12 months of long-term care facilityplacement <strong>in</strong> <strong>the</strong> United States.<strong>Fall</strong>s may be reduced by at least 70% by psychoactive medication <strong>in</strong>terventions. 17 Recommend treatment of anemia and calcium citrate/vitam<strong>in</strong> D supplements <strong>in</strong> every older adult.Abbreviations used: BZ, benzodiazep<strong>in</strong>e; OBRA ‘90, Omnibus Budget Reconciliation Act of 1990; PRN, as needed.e80 • JAPhA • 49:3 • M a y /Ju n 2009www.japha.orgJournal of <strong>the</strong> American Pharmacists Association