2009 ADR v2 Atlas of ESRD - United States Renal Data System
2009 ADR v2 Atlas of ESRD - United States Renal Data System
2009 ADR v2 Atlas of ESRD - United States Renal Data System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
5<br />
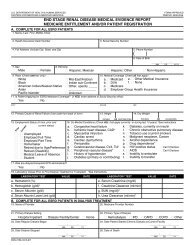
App A<br />
pg 362<br />
ondary payor (MSP) with EGHP, MSP non-EGHP, Medicare Advantage<br />
(Medicare + Choice), Medicaid, or a combination <strong>of</strong> payers. With<br />
this approach, the USRDS is now able to apply payor status information<br />
in all outcome analyses using the “as-treated” model (see the<br />
discussion <strong>of</strong> Chapter Eleven).<br />
PRIMARY CAUSE OF RENAL FAILURE<br />
Information on the primary cause <strong>of</strong> renal failure is obtained<br />
directly from the ME form. For the <strong>ADR</strong> we use eight categories,<br />
with ICD-9-CM codes as follows:<br />
4 diabetes: 250.00 and 250.01<br />
4 hypertension: 403.9, 440.1, and 593.81<br />
4 glomerulonephritis: 580.0, 580.4, 582.0, 582.1, 582.9, 583.1, 583.2,<br />
583.4, and 583.81<br />
4 cystic kidney: 753.13, 753.14, and 753.16<br />
4 other urologic: 223.0, 223.9, 590.0, 592.0, 592.9, and 599.6<br />
4 other cause: all other ICD-9-CM codes covered in the list <strong>of</strong><br />
primary causes on the ME form, with the exception <strong>of</strong> 799.9<br />
4 unknown cause: 799.9 and ICD-9-CM codes not covered in<br />
the list <strong>of</strong> primary causes on the ME form<br />
4 missing cause: no ICD-9-CM code listed<br />
RACE & ETHNICITY<br />
<strong>Data</strong> on patient race and ethnicity are obtained from the ME form,<br />
the CMS Medicare Enrollment <strong>Data</strong>base, and the REMIS/REBUS identification<br />
file. Because they are addressed in separate questions on<br />
the ME form, racial and ethnic categories can overlap.<br />
Patient ethnicity became a required field on the 1995 revised ME<br />
form; because data for 1995 are incomplete, information on Hispanic<br />
patients is presented starting in 1996. The non-Hispanic category<br />
includes all non-Hispanics and patients with unknown ethnicity.<br />
Because <strong>of</strong> the small number <strong>of</strong> <strong>ESRD</strong> patients <strong>of</strong> some races,<br />
as well as the construction <strong>of</strong> the U.S. census data, we concentrate<br />
on white, African American, Native American (includes Alaskan<br />
Native), and Asian (includes Pacific Islander) populations. <strong>Data</strong> on<br />
patients <strong>of</strong> other races will be presented as their numbers increase.<br />
EGHP COHORT<br />
As mentioned, EGHP data in this year’s <strong>ADR</strong> are derived from the<br />
MarketScan and Ingenix I3 databases. To examine the demographic<br />
segment not represented by Medicare, we use enrollment information<br />
to construct yearly cohorts <strong>of</strong> enrollees younger than 65. To ensure<br />
that we select enrollees with the potential to generate claims evidence<br />
appropriate to the demands <strong>of</strong> analytical methods, rules for inclusion<br />
also include 12 months <strong>of</strong> continuous coverage in a commercial<br />
fee-for-service plan, and, for medication analyses, continuous prescription<br />
drug coverage. Comorbidities are identified using claims.<br />
Patients with at least one inpatient claim or at least two outpatient<br />
claims during the period <strong>of</strong> interest and with a diagnosis code <strong>of</strong> a<br />
particular comorbidity are identified as having that comorbidity.<br />
<strong>ESRD</strong> COHORT IN THE EGHP POPULATION<br />
As the MarketScan and I3 databases provide no identifiable data elements,<br />
we cannot link them directly to the USRDS <strong>ESRD</strong> registry. To<br />
identify <strong>ESRD</strong> patients we thus use a process similar to that <strong>of</strong> the<br />
registry. Transplant patients are identified by evidence <strong>of</strong> a kidney<br />
transplant procedure or an adverse graft event, and chronic dialysis<br />
patients by evidence <strong>of</strong> continuous history <strong>of</strong> dialysis therapy, with at<br />
least three consecutive months <strong>of</strong> dialysis service and with dialysis<br />
service claims in at least 70 percent <strong>of</strong> treatment months. Treatment<br />
months are defined from the first dialysis claim to the earliest <strong>of</strong><br />
kidney transplant, death, or end <strong>of</strong> enrollment. Both inpatient and<br />
outpatient claims are evaluated for evidence <strong>of</strong> dialysis service history.<br />
The first <strong>ESRD</strong> service date is set to the earliest <strong>of</strong> the first dialysis<br />
service date or the transplant date. If neither is available, the start<br />
<strong>of</strong> enrollment is used. Incidence is defined by a first <strong>ESRD</strong> service<br />
date at least 60 days after the start <strong>of</strong> enrollment.<br />
Précis<br />
For Figure p.1 we identify chronic kidney disease (CKD), cardiovascular<br />
disease (CVD), and diabetes in patients from the 5 percent<br />
Medicare sample using methods described for Chapter Eleven; these<br />
methods are also used to determine diabetic status and CVD in the<br />
<strong>ESRD</strong> population. Costs for the “cost year” are determined for the<br />
entire calendar year for patients who have fee-for-service coverage<br />
and Medicare as primary payor. Because this analysis combines the<br />
<strong>ESRD</strong> cohort with the 5 percent Medicare sample, <strong>ESRD</strong> patients in<br />
the 5 percent sample are excluded.<br />
Methods for the portion <strong>of</strong> Table p.a that addresses Medicare<br />
spending are addressed in the discussion <strong>of</strong> Chapter Eleven. Total<br />
transplant counts shown in Table p.a include all transplants performed<br />
in 2007 as reported by the OPTN. Transplants <strong>of</strong> unknown<br />
donor type are excluded from by-donor counts. New waiting list<br />
counts include all patients added to the waiting list for a kidneyalone<br />
or a kidney-pancreas transplant in 2007; patients added at<br />
multiple centers are counted once. The total N on the waiting list<br />
includes all patients listed for a kidney-alone or kidney-pancreas<br />
transplant as <strong>of</strong> December 31, 2007, regardless <strong>of</strong> when they first<br />
listed. If patients are added to the list in early 2007 and removed<br />
from the list before the end <strong>of</strong> the year, it is possible for a group to<br />
have more new patients than existing patients, as seen in patients<br />
age 0–17. Median time on the list is shown for patients listed on<br />
December 31, 2007.<br />
Adjusted rates in Figures p.4–5 and p.8 are adjusted for age, gender,<br />
and race.<br />
Figure p.6 shows the point prevalent by-year wait list counts for<br />
those listed for a kidney-alone transplant, and displays the median<br />
time to transplant, as well as the 25 th and 75 th percentiles for time<br />
to transplant, among patients transplanted during the given year.<br />
Time to transplant is computed using Kaplan-Meier methodology.<br />
QUALITY OF CARE<br />
Figure p.12 presents the monthly distribution <strong>of</strong> patients by mean<br />
hemoglobin group, with each month containing all patients with<br />
at least one valid EPO claim during the month. The hemoglobin is<br />
calculated as the reported hematocrit value divided by three. Figure<br />
p.13 shows the mean hemoglobin, by month, for prevalent dialysis<br />
patients with EPO claims, along with the monthly EPO dose per week<br />
for patients with 20 or fewer administrations per month. The mean<br />
EPO dose is adjusted in the same way used in Chapter Five, with a<br />
patient’s time at risk including only those days in which he or she<br />
is not in an inpatient hospital setting.<br />
For Figure p.14, an archived PMMIS quarterly dialysis record is<br />
used to track transfusions in <strong>ESRD</strong> patients before 1991. The percentage<br />
<strong>of</strong> hemodialysis patients receiving transfusions is calculated<br />
as the number receiving at least one transfusion in a given quarter<br />
divided by the number with at least one dialysis record in that quarter.<br />
Since the archived data are current only to the third quarter <strong>of</strong><br />
1995, we emulate this method, using Medicare claims generated by<br />
<strong>ESRD</strong> facilities, to update the data.<br />
Figure p.15 includes prevalent hemodialysis patients in the <strong>ESRD</strong><br />
CPM database who have at least one valid URR measurement. For