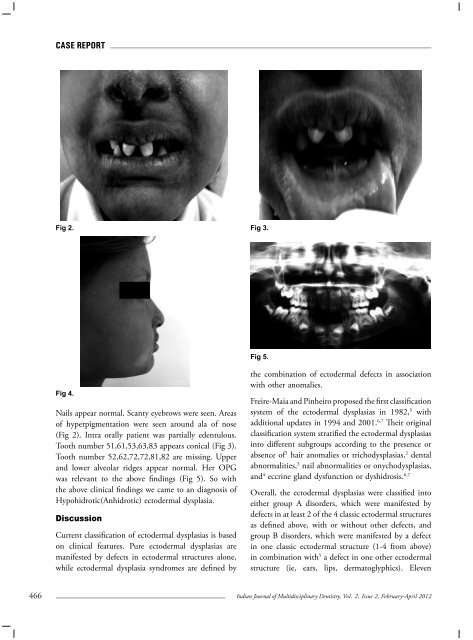
Case ReportFig 2. Fig 3.Fig 5.Fig 4.Nails appear normal. Scanty eyebrows were seen. Areasof hyperpigmentation were seen around ala of nose(Fig 2). Intra orally patient was partially edentulous.Tooth number 51,61,53,63,83 appears conical (Fig 3).Tooth number 52,62,72,72,81,82 are missing. Upperand lower alveolar ridges appear normal. Her OPGwas relevant to the above findings (Fig 5). So withthe above clinical findings we came to an diagnosis ofHypohidrotic(Anhidrotic) ectodermal dysplasia.DiscussionCurrent classification of ectodermal dysplasias is basedon clinical features. Pure ectodermal dysplasias aremanifested by defects in ectodermal structures alone,while ectodermal dysplasia syndromes are defined bythe combination of ectodermal defects in associationwith other anomalies.Freire-Maia and Pinheiro proposed the first classificationsystem of the ectodermal dysplasias in 1982, 5 withadditional updates in 1994 and 2001. 6,7 Their originalclassification system stratified the ectodermal dysplasiasinto different subgroups according to the presence orabsence of 1 hair anomalies or trichodysplasias, 2 dentalabnormalities, 3 nail abnormalities or onychodysplasias,and 4 eccrine gland dysfunction or dyshidrosis. 6,7Overall, the ectodermal dysplasias were classified intoeither group A disorders, which were manifested bydefects in at least 2 of the 4 classic ectodermal structuresas defined above, with or without other defects, andgroup B disorders, which were manifested by a defectin one classic ectodermal structure (1-4 from above)in combination with 5 a defect in one other ectodermalstructure (ie, ears, lips, dermatoglyphics). Eleven466Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 2, February-April 2012
Case Reportgroup A subgroups were defined, each with a distinctcombination of 2 or more ectodermal defects (eg, 2-4, 1-2-3, 1-2-3-4 from above). The group B disorderswere indicated as 1-5, 2-5, 3-5, or 4-5 (from above).We didn’t want to cayegorise according to the abovementioned classification so remained with basic subtypes of Hypohidrotic and Hidrotic. Our case fittedwell with Hyphohidrotic (anhidrotic) ectodermaldysplasia (HAED) with positive clinical findings.Thandani et al 8 (1921) many cases in Hindhu familiesaround Sindhu, India. De Silva et al 9 reported four casesin Ceylon. Many other families have been reported fromIndia. So this case adds up to the previous reportedcases. This case presents with many features suggestiveof diagnosis of Hypohidrotic ectodermal dysplasiaOral findings are of particular interest, since patientswith hyphohidrotic ectodermal dysplasia manifestanodontia, or oligodontia, complete or partial absenceof teeth, seen both in permanent and deciduousdentition. Even the tooth erupted are conical in shape,interestingly growth of jaws are not affected. Howeverin the absence of teeth the alveolar process does notdevelop much resulting in reduction of normal verticaldimension resulting in protuberant lips. In additionhigh arch palate can be more frequent resulting inmore incidence of cleft palate. 3 In our case we hadprotrubernet lips but absence of high arch palate. Ourcase supported all the above findings except for higharch palate.Although mental retardation has been documentedin various subtypes of ectodermal dysplasiab, its realincidence per sub group is not yet firmly establishedso far. 10,11 In this case patient was well co operative anddid not have any mental retardation. In favour of thisdiagnosis the key features are sparse fine hair, conditionsof teeth and decreased sweating. The defective sweatingin this syndrome prevents adequate thermal regulationand predisposes to hyperpyrexia. Febrile seizures,brain damage and death in early life may result fromexposure to hot enviorments. 12 Our patient also wasunable to withstand hot bath or handle any vessels. Soall this is above clinical findings (hair, teeth, skin andits appendages) confirmed our case as Hypohidroticectodermal dysplasia.Reference1.2.3.4.5.6.7.8.9.10.11.12.Thurnam J. Two cases in which the skin, hair and teethwere very imperfectly developed. Proc RM Chir Soc.1848;31:71-82.Weech AA. Hereditary ectodermal dysplasia (congenitalectodermal defect). Am J Dis Child. 1929;37:766-9.Shafer WG, Hine MK, Levy BM. A text book of OralPathology 4th edition. Philadelphia: WB Saunders;1993.pp814-16.Upshaw B.Y, Montgomery.H (1949). Heriditaryectodermal dysplasia- A clinical pathological study.Archeives of dermatology and Syphilology, 60,1170.Pinheiro M, Freire-Maia N. The ectodermal dysplasias.Arch. Dermatol. Apr 1982;118(4):215-6.Pinheiro M, Freire-Maia N. Ectodermal dysplasias:a clinical classification and a causal review. Am J MedGenet. Nov 1 1994;53(2):153-62.Freire-Maia N, Lisboa-Costa T, Pagnan NA. Ectodermaldysplasias: how many?. Am J Med Genet. Nov 152001;104(1):84Thandani k(1921), A tooth less type of man : theBhudaa of India: a case linked inheritance. Journal ofheridty,12,87.De Silva, P.C(1939). Heriditary ectodermal dysplasia ofanhydirotic type. Quarterly journal of medicine,8,97.Tanner BA.Intelectual functioning and ecto.dermaldysplasia. Pediatrics 1985;75:126.Hoyme HE. Reply to Tanners letter. Paediatrics1985;75:126-7.Drago R.P and Ehrenreich T (1961). Ectodermaldysplasia anhydirotic type and prolonged fever in aninfant. New York State Journal Of Medicine, 61, 2473.Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 2, February-April 2012467