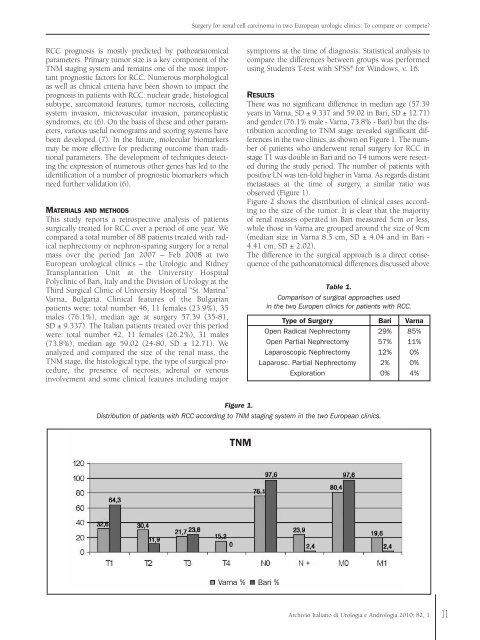
Surgery for renal cell carcinoma in two European urologic clinics: To compare or compete?RCC prognosis is mostly predicted by pathoanatomicalparameters. Primary tumor size is a key component of theTNM staging system and remains one of the most importantprognostic factors for RCC. Numerous morphologicalas well as clinical criteria have been shown to impact theprognosis in patients with RCC: nuclear grade, histologicalsubtype, sarcomatoid features, tumor necrosis, collectingsystem invasion, microvascular invasion, paraneoplasticsyndromes, etc (6). On the basis of these and other parameters,various useful nomograms and scoring systems havebeen developed (7). In the future, molecular biomarkersmay be more effective for predicting outcome than traditionalparameters. The development of techniques detectingthe expression of numerous other genes has led to theidentification of a number of prognostic biomarkers whichneed further validation (6).MATERIALS AND METHODSThis study reports a retrospective analysis of patientssurgically treated for RCC over a <strong>per</strong>iod of one year. Wecompared a total number of 88 patients treated with radicalnephrectomy or nephron-sparing surgery for a renalmass over the <strong>per</strong>iod Jan 2007 – Feb 2008 at twoEuropean urological clinics – the Urologic and KidneyTransplantation Unit at the University HospitalPolyclinic of Bari, Italy and the Division of Urology at theThird Surgical Clinic of University Hospital “St. Marina”Varna, Bulgaria. Clinical features of the Bulgarianpatients were: total number 46, 11 females (23.9%), 35males (76.1%), median age at surgery 57.39 (35-81,SD ± 9.337). The Italian patients treated over this <strong>per</strong>iodwere: total number 42, 11 females (26.2%), 31 males(73.8%), median age 59.02 (24-80, SD ± 12.71). Weanalyzed and compared the size of the renal mass, theTNM stage, the histological type, the type of surgical procedure,the presence of necrosis, adrenal or venousinvolvement and some clinical features including majorsymptoms at the time of diagnosis. Statistical analysis tocompare the differences between groups was <strong>per</strong>formedusing Student’s T-test with SPSS ® for Windows, v. 16.RESULTSThere was no significant difference in median age (57.39years in Varna, SD ± 9.337 and 59.02 in Bari, SD ± 12.71)and gender (76.1% male - Varna, 73.8% - Bari) but the distributionaccording to TNM stage revealed significant differencesin the two clinics, as shown on Figure 1. The numberof patients who underwent renal surgery for RCC instage T1 was double in Bari and no T4 tumors were resectedduring the study <strong>per</strong>iod. The number of patients withpositive LN was ten-fold higher in Varna. As regards distantmetastases at the time of surgery, a similar ratio wasobserved (Figure 1).Figure 2 shows the distribution of clinical cases accordingto the size of the tumor. It is clear that the majorityof renal masses o<strong>per</strong>ated in Bari measured 5cm or less,while those in Varna are grouped around the size of 9cm(median size in Varna 8.5 cm, SD ± 4.04 and in Bari -4.41 cm, SD ± 2.02).The difference in the surgical approach is a direct consequenceof the pathoanatomical differences discussed aboveTable 1.Comparison of surgical approaches usedin the two Europen clinics for patients with RCC.Type of Surgery Bari VarnaOpen Radical Nephrectomy 29% 85%Open Partial Nephrectomy 57% 11%Laparoscopic Nephrectomy 12% 0%Laparosc. Partial Nephrectomy 2% 0%Exploration 0% 4%Figure 1.Distribution of patients with RCC according to TNM staging system in the two European clinics.TNMVarna % Bari %Archivio Italiano di Urologia e Andrologia 2010; 82, 111
S.D. Dyakov, G. Lucarelli, A.I. Hinev, P.K. Chankov, D. Anakievski, P. Ditonno, P. Martino, F.P. Selvaggi, M. BattagliaFigure 2.Distribution of clinical cases according to the size of the tumor.Tumor size spread in two clinicsTumor size VarnaTumor size Bari(Table 1). In Varna 84.8% of the patients underwent radicalnephrectomy, 10.9% nephron-sparing surgery and4.3% explorative laparotomy only due to unresectablerenal masses. In Bari only 28.6% were treated by radicalnephrectomy, 57.1% underwent partial nephrectomy,11.9% laparoscopic nephrectomy, and 2.4% partial laparoscopicresection. This difference is significant and demonstratesthe need for a better early diagnosis of renal massesin Varna. Modern surgical approaches yield a better outcomein terms of patient recovery after surgery, better prognosisand preserved renal function. The presence of unresectablerenal masses observed only in the Varna clinic suggestspoor screening measures in Bulgaria or late referral toa specialist in urology for various reasons.The presence of necrosis in the renal mass on histologicalinvestigation is a prognostic marker included in few prognosticscore systems. We also evaluated the presence ofnecrosis, and again the result did not favour the Bulgarianpopulation. The number of histological specimens positivefor necrosis in Varna was twice that in Bari -37% vs 19%.Other markers of advanced disease such as involvement ofthe adrenal gland and a venous thrombus were found in asmall number of cases, that do not allow any conclusionsto be drawn, but the prevalence was again higher amongpatients in the Bulgarian site (adrenal involvement in 4cases in Varna and 2 in Bari, while there were 2 cases ofvenous thrombosis in Varna but none in Bari).We also analyzed the patients according to major symptoms:gross hematuria, pain and palpable mass at the timeof diagnosis. The <strong>per</strong>centage of patients presenting withsymptoms was 43.5% in Varna, the rest being incidentalfindings; 33.3% of the Italian patients were symptomatic atdiagnosis.DISCUSSIONKidney cancer incidence and mortality rates have increasedduring the last years in different countries. In the EuropeanUnion as a whole, mortality from kidney cancer peaked inthe early 1990s at 4.8 <strong>per</strong> 100000 men and 2.1 <strong>per</strong> 100000women, then declined to 4.1 <strong>per</strong> 100000 men and 1.8 <strong>per</strong>100000 women. This trend is the expression of a decreasedkidney cancer mortality that has been observed since theearly 1990s in many western and central European countries.In Italy the mortality rates from kidney cancer <strong>per</strong>100000 men and women were reduced by -12.3% and -13.5%, respectively, in 1992-2002. We have no data aboutthe mortality rates for Bulgaria in the <strong>per</strong>iod 1992-2002,but taking into account another country in the same geographicarea, such as Hungary, this pattern of reduced mortalityis confirmed (-4.4% and -2.6% <strong>per</strong> 100000 men andwomen, respectively) (8). These data are partly a reflectionof the decline in smoking prevalence, and partly the consequenceof the increased use of new imaging diagnosticprocedures that has anticipated the date of diagnosis, thusincreasing the incidence of early stage tumors. This earlydiagnosis, together with the introduction of new targetedtherapies, has contributed to improve the overall survivalrate of patients with kidney cancer in many Europeancountries.The treatment of renal cell cancer has rapidly evolved overthe last decade, showing a trend towards the widespreaduse of minimally invasive treatment options formerly consideredpurely ex<strong>per</strong>imental, for localized RCC .Over the past 15 years laparoscopic procedures in urologyhave become a widely used approach for many surgicalindications. In many centers laparoscopy is now an integralpart of daily practice (9). The well-known difficult learningcurve for laparoscopic procedures has led to the developmentof alternatives that shorten the learning curve andimprove surgical outcomes.In kidney surgery the popularity of hand-assisted nephrectomyis a good example of a pragmatic approach to shorteningthe learning process (10-12).The radical nephrectomy described by Robson in 1963[5], is considered the standard of care in the managementof renal tumors and still remains the gold standard forcomparison with any new surgical technique Although12Archivio Italiano di Urologia e Andrologia 2010; 82, 1
- Page 2 and 3: Official Journal of the SIEUN, the
- Page 4 and 5: ContentsHistological evaluation of
- Page 7 and 8: R. Leonardi, R. Caltabiano, S. Lanz
- Page 9 and 10: R. Leonardi, R. Caltabiano, S. Lanz
- Page 11 and 12: F. Galasso, R. Giannella, P. Bruni,
- Page 13 and 14: F. Galasso, R. Giannella, P. Bruni,
- Page 15: ORIGINAL PAPERSurgery for renal cel
- Page 19 and 20: S.D. Dyakov, G. Lucarelli, A.I. Hin
- Page 21 and 22: M. Aza, S.S. Iqbal, M.V. Muhammad,
- Page 23 and 24: Archivio Italiano di Urologia e And
- Page 25 and 26: The Clavien classification system t
- Page 27 and 28: PRESENTATIONPercutaneous nephrolith
- Page 29 and 30: Percutaneous nephrolithotomy: An ex
- Page 31 and 32: PCNL in ItalyTable 1.Number and hos
- Page 33 and 34: PCNL in ItalyFigure 3.Comparison be
- Page 35 and 36: The patient position for PNL: Does
- Page 37 and 38: PCNL: Tips and tricks in targeting,
- Page 39 and 40: Tubeless percutaneous nephrolithoto
- Page 41 and 42: PRESENTATIONHigh burden and complex
- Page 43 and 44: High burden and complex renal calcu
- Page 45 and 46: PRESENTATIONEndoscopic combined int
- Page 47 and 48: PRESENTATIONHigh burden stones: The
- Page 49 and 50: PRESENTATIONStone treatment in chil
- Page 51 and 52: Stone treatment in children: Where
- Page 53 and 54: PRESENTATIONExtracorporeal shock wa
- Page 55 and 56: PRESENTATIONPercutaneous nephrolith
- Page 57 and 58: PRESENTATIONFlexible ureteroscopy f
- Page 59 and 60: Flexible ureteroscopy for kidney st
- Page 61 and 62: Indications, prediction of success
- Page 63 and 64: Indications, prediction of success
- Page 65 and 66: Indications, prediction of success
- Page 67 and 68:
Indications, prediction of success
- Page 69 and 70:
Laparoscopic and open stone surgery
- Page 71 and 72:
Laparoscopic and open stone surgery
- Page 73 and 74:
Laparoscopic and open stone surgery
- Page 75:
Laparoscopic and open stone surgery