The DermaTologisT's BoarD review
The DermaTologisT's BoarD review
The DermaTologisT's BoarD review
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
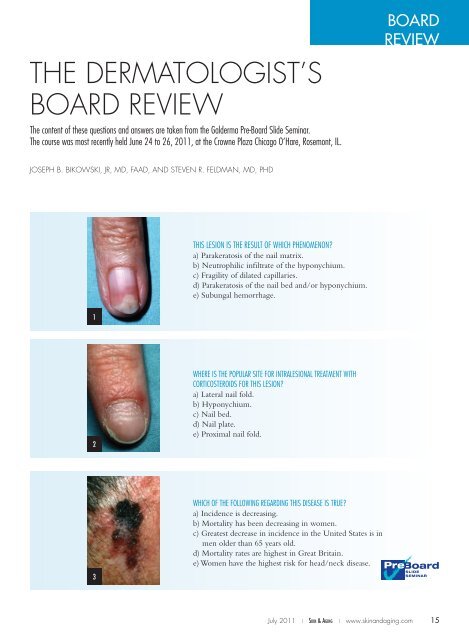
<strong>The</strong> Dermatologist’sBoard Review<strong>The</strong> content of these questions and answers are taken from the Galderma Pre-Board Slide Seminar.<strong>The</strong> course was most recently held June 24 to 26, 2011, at the Crowne Plaza Chicago O’Hare, Rosemont, IL.BoardReviewJoseph B. Bikowski, JR, MD, FAAD, and Steven R. Feldman, MD, PhDThis lesion is the result of which phenomenon?a) Parakeratosis of the nail matrix.b) Neutrophilic infiltrate of the hyponychium.c) Fragility of dilated capillaries.d) Parakeratosis of the nail bed and/or hyponychium.e) Subungal hemorrhage.12Where is the popular site for intralesional treatment withCORTICOSTeroids for this lesion?a) Lateral nail fold.b) Hyponychium.c) Nail bed.d) Nail plate.e) Proximal nail fold.3Which of the following regarding this disease is true?a) Incidence is decreasing.b) Mortality has been decreasing in women.c) Greatest decrease in incidence in the United States is inmen older than 65 years old.d) Mortality rates are highest in Great Britain.e) Women have the highest risk for head/neck disease.July 2011 | Skin & Aging | www.skinandaging.com 1515 6/30/11 10:29 AM
Board Review Answers1 and 2. Psoriasis of the Nail1. This lesion is the result of which phenomenon?d) Parakeratosis of the nail bed and/or hyponychium.2. Where is the popular site for intralesional treatment with corticosteroids for this lesion?e) Proximal nail fold.Review of Nail AnatomyNail plate: Divided into dorsal, intermediate and ventral portions,is composed of abundant calcium complexed with phosphate as hydroxyapetite.Sulfur provides the strength of the nail plate.Nail folds: Divided into dorsal and ventral proximal nail fold. Histologyis identical to the epidermis but lacks adnexal structures. <strong>The</strong>eponychium is at the junction of ventral and distal portions and representsa continuation of the stratum corneum, therefore lacking nuclei.Nail matrix: Consists mainly of keratinocytes, has unique maturationprocess and as it migrates, becomes flatter, lyse and loses nuclear contentintegrating into nail plate (onychocytes). <strong>The</strong> matrix cells keratinizewithout a granular layer. <strong>The</strong> matrix also contains melanocytes.Nail bed: Lies beneath the nail plate, lacks subcutaneous fatand also does not have a granular layer. Has parallel longitudinalridges from lunula to hyponychium interlocking with reteridges at DEJ serving to bind nail bed to nail plate.Hyponychium: Transition zone from nail bed to normal epidermis.Lunula: Visible portion of nail matrix.Embryologically, nail field appears at 9 weeks, primordialmatrix at 11 weeks, keratinization at 20 weeks, and distinct nailunit structures at 32 weeks of gestation.3. Screening, Early Detection and Trends for MelanomaWhich of the following regarding this disease is true?b) Mortality has been decreasing in women.Epidemiology: Incidence in the U.S. increasing steadily with a 200%increase over past 2 decades, with greatest rise seen in men ages 55 to64 (4x increase) and age >65 (5-fold increase). Between 1988 and1999, 2/3 of melanomas diagnosed in the U.S. were 90% 5-year survival rate overall. Mortality ratesfor melanoma are highest in New Zealand, Australia and Norway.Risk Factors: U.S. males have higher risk for head/neck andtrunk lesions. Those with >10 sunburns have a 7-fold increasein risk of upper extremity melanoma. Having more than 10Nail Findings in PsoriasisPitting: Superficial depressions in the uppermost nail plate representpsoriatic activity of dorsal nail matrix, where parakeratosis disruptsnormal keratinization. <strong>The</strong> parakeratotic cells are sloughed as the nailplate extends, resulting in pits. <strong>The</strong> proximal nail fold also may be involvedin pit formation. Length of pits indicates duration of psoriaticinvolvement of the matrix; deeper pits indicate involvement of intermediateor ventral matrix.Discoloration/Onycholysis: Parakeratosis of nail bed results in “oil drop”discoloration; parakeratosis of the hyponychium results in onycholysis.Subungual hyperkeratosis: Deposition and collection of cells underthe nail plate that have not desquamated. A yellowish/greasy appearanceto the hyperkeratosis indicates strong inflammatory response, accumulationof proteinaceous material at the upper dermis and disappearanceof the stratum granulosum of the hyponychium. <strong>The</strong> white/silvery variant has less inflammation and loss of the granular layer.Splinter hemorrhages: Result from broken fragile capillaries.TreatmentCorticosteroids/Vitamin D Analogs: Pitting and ridging mayresolve with treatment of the nail folds alone. For nail bed disease(onycholysis and hyperkeratosis), medication should be applied tothe nail plate with hopes of reaching the nail bed (salicylic acidand/or occlusion may help with penetration). Combined therapywith potent corticosteroids and calcipitriol have been shownto reduce nail thickness/hyperkeratosis in psoriatic patients. <strong>The</strong>proximal nail fold and lateral nail folds are susceptible to atrophy.5-fluorouracil: Some improvement in pitting and hyperkeratosiswith twice-daily application of 1% solution to proximalnail fold for 6 months.Anthralin: Onycholysis and pitting improved a little, with noeffect on hyperkeratosis.Tazarotene: A decrease in nail pitting and onycholysis hasbeen shown with nightly application of gel.Cyclosporine: Difficult to compound, but has been shown toimprove nail psoriasis.Intralesional <strong>The</strong>rapy: Particularly effective in treating dystrophiesassociated with the nail matrix such as pitting/ridging.<strong>The</strong> proximal nail fold overlies the matrix and is a popularplace for injection. For hyperkeratosis and oil drop spots, psoriasisinvolves the nail bed, and injection here is not recommended.Injection of the lateral nail folds is technically difficult,but can result in improvement of these lesions. Concentrationsof 1 mg/cc up to 10 mg/cc have been used.Phototherapy: PUVA and UVB have shown variable results.Radiotherapy: Superficial radiotherapy has been effective butis decreasing in use. Grenz rays and electron beam therapieshave shown variable efficacy but are not regularly used.Systemic <strong>The</strong>rapy: A trial of patients with nail and skin diseasedemonstrated some effect of cyclosporine plus etretinate(1995); however, treatment of nail disease alone with systemictherapy should be frowned upon.Newer agents such as etanercept and other biologics have notroutinely been studied for their effect on nail disease in patientswho also have skin disease.upper extremity moles also increaeses risk. Patients with head/neck melanoma are typically older than those with other anatomicsites melanomas. Symptoms correlating with Breslowdepth are bleeding, pain, lump, itching and change in size.Screening: No community-wide screening for melanoma iscurrently advocated. Dermatology-led screening one time, every2 years, and annually saved 2.5, 8.8 and 10.2 quality-adjusted lifeyears per 1,000 screened, respectively. Self-skin examination leadsto the detection of 50% of thicker melanomas (physicians are betterat detection of thinner lesions). Selective screening may be recommendedfor high-risk populations: middle-aged/older men, familymembers of melanoma patients, patients with a personal history ofmelanoma, patients with non-melanomatous skin cancer/actinickeratoses, transplant patients, those with many atypical moles. n16 July 2011 | Skin & Aging | www.skinandaging.com16 6/30/11 10:29 AM