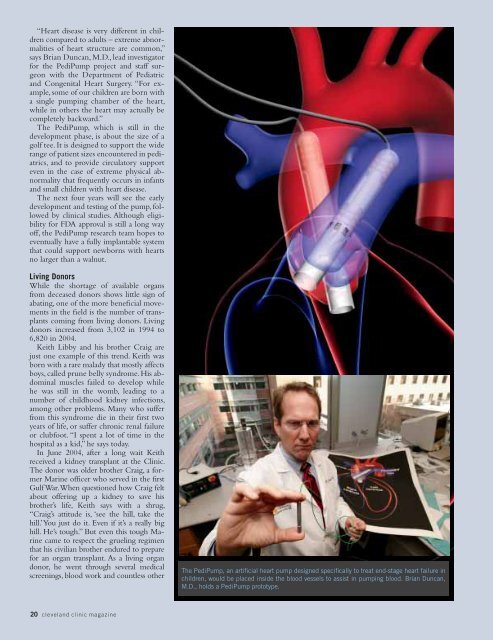
“Heart disease is very different in childrencompared to adults – extreme abnormalitiesof heart structure are common,”says Brian Duncan, M.D., lead investigatorfor the PediPump project and staff surgeonwith the Department of Pediatricand Congenital Heart Surgery. “For example,some of our children are born witha single pumping chamber of the heart,while in others the heart may actually becompletely backward.”The PediPump, which is still in thedevelopment phase, is about the size of agolf tee. It is designed to support the widerange of patient sizes encountered in pediatrics,and to provide circulatory supporteven in the case of extreme physical abnormalitythat frequently occurs in infantsand small children with heart disease.The next four years will see the earlydevelopment and testing of the pump, followedby clinical studies. Although eligibilityfor FDA approval is still a long wayoff, the PediPump research team hopes toeventually have a fully implantable systemthat could support newborns with heartsno larger than a walnut.Living DonorsWhile the shortage of available organsfrom deceased donors shows little sign ofabating, one of the more beneficial movementsin the field is the number of transplantscoming from living donors. Livingdonors increased from 3,102 in 1994 to6,820 in 2004.Keith Libby and his brother Craig arejust one example of this trend. Keith wasborn with a rare malady that mostly affectsboys, called prune belly syndrome. His abdominalmuscles failed to develop whilehe was still in the womb, leading to anumber of childhood kidney infections,among other problems. Many who sufferfrom this syndrome die in their first twoyears of life, or suffer chronic renal failureor clubfoot. “I spent a lot of time in thehospital as a kid,” he says today.In June 2004, after a long wait Keithreceived a kidney transplant at the Clinic.The donor was older brother Craig, a formerMarine officer who served in the firstGulf War. When questioned how Craig feltabout offering up a kidney to save hisbrother’s life, Keith says with a shrug,“Craig’s attitude is, ‘see the hill, take thehill.’ You just do it. Even if it’s a really bighill. He’s tough.” But even this tough Marinecame to respect the grueling regimenthat his civilian brother endured to preparefor an organ transplant. As a living organdonor, he went through several medicalscreenings, blood work and countless otherThe PediPump, an artificial heart pump designed specifically to treat end-stage heart failure inchildren, would be placed inside the blood vessels to assist in pumping blood. Brian Duncan,M.D., holds a PediPump prototype.20 cleveland clinic magazine
kinds of preparation, prompting him to askhis younger brother: “Is this what you’vebeen going through your whole life?”Since the first living donor transplant byDr. Murray on the Herrick twins in 1954,thousands of these transplants have beenperformed. In 2001, history was madewhen more transplanted organs came fromliving than from deceased donors, with themost common donation being a kidney.“In the last five years, there’s been a shiftin where kidneys are coming from,” saysDavid Goldfarb, M.D., a transplant surgeonwith the Glickman Urological Institute.“More are coming from living donors andthe outcomes are better. All of these thingsare pushing us toward living donors.”Today, 50 percent of all kidney transplantsare performed using living donors.“The long-term safety of living with onekidney has been established by the data,”says Dr. Goldfarb. “And the emergence ofminimally invasive surgery for donors hashelped, because there’s less pain and disruptioninvolved in being a donor now.”The ability to perform transplant surgeriesusing minimally invasive techniquesalso has helped increase the use of livingdonors for other organs, including theliver, lung and pancreas. “With the liver,we remove only a section from the livingdonor to use as a transplant,” explains Dr.Fung. “And because the liver has the abilityto regenerate, it eventually becomeswhole again.”Though the lung cannot regenerate itself,a single lobe can be donated and theremaining lung tissue expands to fill thedonated area.With living organ donations accountingfor only 10 percent of all liver transplantsand less than 2 percent of lung transplants,various efforts are being made to increaseorgan donations, particularly from livingdonors. Recently, the American MedicalAssociation (AMA) adopted a new ethicspolicy to guide physicians involved intransplanting organs from living donors.According to the AMA, these are the firstnational guidelines to be developed. Theguidelines include assigning living donorsan advocacy team that is primarily concernedwith the well-being of the donor,and physician support for the developmentand maintenance of a national databaseof living donor outcomes.Other groups also continue to innovatein an effort to increase living organ donations.In Ohio, a new computer organmatchingprogram - the only one of itskind in the nation - matches would-bekidney donors and recipients by lookingat the usual transplant list variables, such asage and blood type, but with one distinctdifference. With the new program, run bythe Ohio Solid Organ Transplant Consortium(OSOTC), someone in need of akidney cannot get onto this registry alone.He or she must have another person signup as a living organ donor. This paired exchangeprogram allows for better matchesas many times a person willing to donatean organ to a loved one or a friend can’tbecause they are not a match. This programallows them to donate to someonewho is a match, as long as that person hassomeone who can donate back to theoriginal person in need.Dr. Goldfarb, who performed the secondsuch paired kidney exchange transplantmade possible through the OSOTC program,says the program is a “win-win to allparties involved.” He hopes the program attractsmany more people to join and thatother states develop similar programs oftheir own.Splitting LiversIn November 2004, the Clinic’s livertransplant team learned there was a donororgan available in Michigan that was amatch for Christine Tabar, the 14-year-oldborn with biliary atresia whose liver wasrapidly failing. The organ, however, wasdesignated for a local child. Not wantingto forfeit this rare opportunity, Liver TransplantProgram Director Charles Miller,M.D., and his Clinic colleagues proposedperforming a split-liver transplant. “Thisway,” says Dr. Miller, “both lives could besaved using this one organ.”In a split-liver transplant, the liver is dividedalong the lines of its sections or lobes,so that instead of one person receiving adonated liver, two people can benefit.Most split-liver transplants involve cuttingthe liver into a three-quarter sectionand a separate one-quarter piece, with thelarger piece going to an adult and thesmaller to a child. Dr. Miller, however, hasperfected a method of bisecting the organinto two equal halves. “The advantage ofthis method is that two people still canbenefit, but one doesn’t have to be a verysmall child.”It was this innovative technique thathelped to save Christine Tabar’s life. Withprecise timing, Dr. Miller flew to Michiganand removed the necessary tissue and bloodvessels, while Dr. Fung began the surgery inCleveland to remove Tabar’s malfunctioningliver. When Dr. Miller returned withthe split liver, Dr. Fung completed thenearly day-long operation that transplantedthe new organ. Today, Tabar is back at homeplaying the sports she enjoys most.“Dr. Miller contributed significantly tothe split-liver technique used with livingdonors and he continues to improve uponthis same technique,” says Dr. Fung. “Whensplit-liver transplants were first performedin the early 1990s, the results were not optimal.With more experience and the determinationof the surgical profession, theseprocedures now produce results that arecomparable to whole liver transplants.”Expanding the Donor PoolAs transplant specialists develop a betterunderstanding of what constitutes ahealthy donor organ, many are sheddingthe more rigid parameters that might haveruled out accepting organs from donorsover a certain age. “We now use liversfrom people who are up to 86 years old,”says Dr. Miller. “That change is a result ofour better understanding of what makes agood liver good. We now have better informationregarding the risks over time ofany one part of the donor pool.”Some of that increasing sophisticationin assessing the potential donor organ poolcomes as a result of better data from researchers,and some comes from simplyhaving more medical expertise in-house.“The liver transplant team here, composedof six surgeons, has a collective experienceof more than 100 years. Withmore experience and better data, we canmake better judgments,” says Dr. Miller.Benefits of the improvements intransplantation are being felt by donorseverywhere.A year after his surgery, Keith Libbycalls himself “a blessed man. They say theaverage transplanted kidney lasts just fiveto ten years. But, personally, I think I’mgoing to go 30 years, based on how wellit’s going so far.”Helen Schtscherbak, meanwhile, hopesto join Libby some day soon. She remainsas upbeat as she can, as she patientlyawaits her new liver. “You have to trustyour doctor and the whole team that’slooking out for you, because you’re intheir hands now.”www.clevelandclinic.org 21