Pharmacy Services Agreement 2010 Guide for Guild members
Pharmacy Services Agreement 2010 Guide for Guild members
Pharmacy Services Agreement 2010 Guide for Guild members
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyIntroductionThis <strong>Guide</strong> does not constitute legal advice. The <strong>Guide</strong> was prepared basedon the template <strong>for</strong> the <strong>Pharmacy</strong> <strong>Services</strong> <strong>Agreement</strong> <strong>2010</strong> provided by DHBNZ.While we have been assured that this template will be applied nationally, yourown <strong>Agreement</strong> may differ from the template. In particular, Part P of the <strong>Agreement</strong>contains clauses specific to you, the provider. While every ef<strong>for</strong>t has been madeto ensure this <strong>Guide</strong> accurately reflects the template, your <strong>Agreement</strong> may differ.The interim national base <strong>Pharmacy</strong> <strong>Services</strong> <strong>Agreement</strong>(PSA) has been released. The purpose of this document isto provide <strong>Guild</strong> <strong>members</strong> with a detailed analysis of thechanges contained within the interim PSA.The PSA is available on the DHBNZ website(www.dhbnz.org.nz) in template <strong>for</strong>m. Additionally,two hard copies personalised to your pharmacy shouldhave been posted to you by your DHB <strong>for</strong> consideration.Also included in this mail out were a cover letter and alegally binding side letter regarding the Date ofDispensing definition.The interim PSA will run <strong>for</strong> a maximum period of18 months from 1 March <strong>2010</strong> to 31 August 2011.This PSA has been designed to allow the developmentof a new model <strong>for</strong> community pharmacy in thenext PSA. The <strong>Guild</strong>, DHBs and other agents will beworking together on the future PSA during this period.Your existing arrangements with your DHB continueto apply until 28 February <strong>2010</strong>.This document is in four parts. Section One is an overviewof the major changes between PSA 2007 and PSA <strong>2010</strong>.Section Two is a clause-by-clause analysis of the changes.Section Three is a user guide to PSA <strong>2010</strong>. Finally, SectionFour is a checklist to guide you through the signing process.Any updates or news will be communicated to you via<strong>Guild</strong> INTOUCH.The <strong>Guild</strong> advises <strong>members</strong> to signthe <strong>Agreement</strong>.PAGE 1
confidential – <strong>for</strong> guild <strong>members</strong> onlySection One: OverviewAs expected, there has been no change to the dispensingfee. However, there have been a number of positiveadjustments. We believe these changes will increase thenet profit of community pharmacy.The financial crisis turned the spotlight on the largeincreases in health spending over the last decade. Going<strong>for</strong>ward, it will be increasingly difficult <strong>for</strong> the governmentto justify a continuation of growth in health expenditurethat is far in excess of New Zealand’s growth rate.The <strong>Guild</strong> pushed hard on a number of issues and weachieved a number of wins. Overall, the <strong>Guild</strong> feels thatthis PSA offers a significant improvement on the PSA nowin place: We will do everything in our power as yourrepresentative to ensure that <strong>2010</strong> will be a better year<strong>for</strong> pharmacy.PSA <strong>2010</strong> is interim in nature. It is designed to providesome stability to the sector while larger discussions cantake place regarding a fresh approach to contractingpharmacy services. DHBs, PHARMAC and the <strong>Guild</strong> haveall committed resources to these ongoing discussions.FUNDING CHANGES■■ Ordinary business hours will be from 8.30am-5pm –Monday to Friday. You will be able to applyreasonable after hours’ charges outside these hours.■■ On new scripts you will now be able to claim thedispensing fee <strong>for</strong> uncollected medicines. In addition,if you cannot return the medicine to stock you will bereimbursed <strong>for</strong> the cost of the medicine. This will alsoapply to repeat scripts so long as you can show therepeat was requested.■■ A definition <strong>for</strong> the “date <strong>for</strong> dispensing” has beeninserted into the interim PSA. It defines this as thedate of collection by the patient. While DHBs arguethat this has always been implied by the contract, thishas not been the way in which pharmacy practice hasevolved. The <strong>Guild</strong> is aware that this is problematicand has been working with DHBs, Audit andCompliance and PHARMAC to achieve a workablesolution. We have DHBs’ assurances, both verballyand by way of a side letter, that this definition willnot be en<strong>for</strong>ced until all the practical implicationshave been identified and the necessary enhancementsare made within dispensing software.■■■■■■■■■■■■■■■■The <strong>Guild</strong> has obtained legal advice that the sideletter is binding on the DHBs and can be relied on byyou. This advice is available <strong>for</strong> download from themember-only section of our website.If you choose to accept your <strong>Agreement</strong>, the <strong>Guild</strong>’sadvice is to sign and date copies of each page of theside letter and attach these to each copy of your<strong>Agreement</strong>. This rein<strong>for</strong>ces that your acceptance ofthe PSA was predicated on the assurances given inthe side letter.DHBs will pay the remaining money from the $3million <strong>for</strong> the Wholesale Uplift Fee.DHBs will inject another $500,000 to address theSpecial Foods issue. The mechanism has yet to bedetermined.DHBs will provide up to $3 million to compensatepharmacies <strong>for</strong> the additional work arising from brandswitches. The mechanism <strong>for</strong> these payments topharmacy has yet to be determined.DHBs remain concerned about the large <strong>for</strong>ecastgrowth <strong>for</strong> total dispensing fee expenditure. However,they have committed not to intervene to try toreduce this <strong>for</strong>ecast growth over the term of this PSA.Dispensing volumes are <strong>for</strong>ecast to grow by 8% in2009/<strong>2010</strong> and 4.5% in <strong>2010</strong>/2011. These are DHB<strong>for</strong>ecasts; PHARMAC’s growth <strong>for</strong>ecasts are higher.Claiming can occur four times per month <strong>for</strong> pharmacistsclaiming online – this means you will get the moneyfaster. If you do not claim online, the two claim periodsand payment dates in the current PSA will continue toapply.DHBs will fund pharmacies to move to onlineclaiming. Pharmacies will be paid $500 <strong>for</strong> initialset up costs and will receive an ongoing monthlypayment of $100.On the downside, NRT will be paid at the standarddispensing fee rate. This includes Quit Cards.PAGE 2
confidential – <strong>for</strong> guild <strong>members</strong> onlyPHARMACY PRACTICE CHANGES■■ “Cherry picking” has been prohibited in the new PSA.“Cherry picking” refers to the questionable practiceof turning away difficult business and focussing onthe simple and profitable prescriptions.■■ Allowable pharmacy intervention charges have beena hot topic. The interim PSA will preserve yourexisting right to intervention charge but prohibits youfrom charging a blanket or flat fee.■■ A handful of pharmacies have been abusing the weeklyclose control system. DHBs will work with the sector todevelop guidelines that will guide Audit andCompliance in their investigations. There is no proposedchange to the legitimate use of weekly close control.ADDITIONAL NOTES■■ The variations are now contained within the PSAitself. You will need to check Part P of your<strong>Agreement</strong> to ensure that it correctly identifies thevariations that apply to you.■■ There are numerous variations that, while commonplace,do not <strong>for</strong>m part of the nationally-consistent base<strong>Agreement</strong> and there<strong>for</strong>e are not covered by this <strong>Guide</strong>(eg Medicine Use Review services, rural top-up schemesetc). Please contact your local <strong>Guild</strong> representative, <strong>Guild</strong>HQ, or your DHB if you have questions regarding theselocal variations.■■ The work on the Procedures Manual is progressingand ongoing.■■ Aseptic <strong>Pharmacy</strong> <strong>Services</strong> and Sterile Manufacturing<strong>Services</strong> have been split into two separate servicespecifications.■■ Additional work will be needed to meet therequirements of the Sterile Manufacturing <strong>Services</strong>service specification.■■ Additional work may be needed to meet therequirements of the Clozapine <strong>Services</strong> contract asthe date of dispensing must now be entered into thesupplier’s website.■■ We continue to work with the DHBs on the next PSAincluding the funding model project, as well as issuessuch as patients near death, close control, weeklyclose control and fax scripts.The deadline <strong>for</strong> having your signed <strong>Agreement</strong>returned to your DHB is 28 February <strong>2010</strong>.PAGE 3
confidential – <strong>for</strong> guild <strong>members</strong> onlySection Two: Clause-by-clause analysisThe purpose of this part of the document is to provide <strong>members</strong> that are familiar with the previous PSA with a detailedanalysis of the changes that have been made in PSA <strong>2010</strong>. For <strong>members</strong> unfamiliar with previous PSAs “Section Three:PSA <strong>2010</strong> user guide”, may provide a better starting place <strong>for</strong> understanding the structure and requirements of the PSA.Clause Change CommentContents Schedule C2 (Protocols) inserted. See comments on Schedule C2 below.Part ANo change.Part B B2.1 Commencement date of new PSA1 March <strong>2010</strong>.B2.2 Termination date of new PSA31 August 2011.The new PSA starts immediately following the expiry ofthe old PSA.The new PSA runs <strong>for</strong> 18 months. DHBs have signalled thatsome DHBs may be able to switch to a new fundingcontract be<strong>for</strong>e the completion of 18 months.Part C C2.1 More detail added. This change reflects the inclusion of more services inthe PSA. These services were previously contracted asvariations to the PSA. Now, each of these services is listedin the PSA, even if you do not do them. Part P lists whichof these services you are able to deliver and be paid <strong>for</strong>.If the service is not expressly listed in Part P as a serviceyou are contracted to provide, you cannot claim paymentunder this contract.Part C C2.2 Updated reference to another clausethat has had a numbering change.C4.1 No change. Please note that your DHB has no obligation to fund anyservices you provide to persons outside their geographicalarea unless you have their prior agreement in writing.Please check the geographic location of any rest homesyou contract to. Also note that in practice, DHBs do noten<strong>for</strong>ce this provision <strong>for</strong> individuals travelling away fromtheir homes.Part D No change. Note that the provisions of Part D do not constitute legallybinding commitments.Part E E1.3 Numerous definition changes:Insertion of Aseptic <strong>Pharmacy</strong> <strong>Services</strong>definition.Insertion of Audit and Compliancedefinition.Updated Claim Period definition.Insertion of Complex Medicine <strong>Services</strong>definition.Reflects the option of either two-times-a-month orfour-times-a-month claiming.Note that Complex Medicine is currently denoted inthe Pharmaceutical Schedule as HP1 pharmaceuticals.PAGE 4
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentInsertion of Date of Dispensing definition.Updated Dispensing definition.The date of collection by the patient. While DHBs arguethat this has always been implied by the contract, this hasnot been the way in which pharmacy practice has evolved.The <strong>Guild</strong> is aware that this is problematic and has beenworking with DHBs, Audit and Compliance and PHARMACto achieve a workable solution.We have DHBs’ assurances, verbally and by way of sideletter, that this definition will not be en<strong>for</strong>ced until allthe practical implications have been identified and thenecessary enhancements are made within dispensingsoftware. Given the 18 month term of the agreement, thisis unlikely to have an impact on this PSA.The <strong>Guild</strong> has obtained legal advice that the side letter isbinding on the DHBs and can be relied on. This advice isavailable on the <strong>Guild</strong>’s website. We understand DHBshave obtained similar advice.If you choose to accept your <strong>Agreement</strong> the <strong>Guild</strong>’s adviceis to sign and date copies of each page of the side letterand attach these to each copy of your <strong>Agreement</strong>.This rein<strong>for</strong>ces that your acceptance of the PSA wasbased on the assurance given in the side letter.Reference to NRT Exchange Cards removed from theDispensing definition.Insertion of Monitored TherapyMedicine <strong>Services</strong> definition.Removed NRT <strong>Services</strong> definition.Removed HealthPAC definition.Insertion of Medicines Act definition.Insertion of Medicines Regulationsdefinition.Updated Payment Date definition.Removed <strong>Pharmacy</strong> NRT Proceduresdefinition.Updated Practitioner’s Supply Orderdefinition.Updated Preferred Supplier Branddefinition.Updated Prescription Item definition.Updated Procedures Manual definition.Insertion of Provision of Blood GlucoseTest Strips definition.Updated Quality Standards <strong>for</strong> <strong>Pharmacy</strong>in New Zealand definition.Note that Monitored Therapy Medicine is currentlydenoted in the Pharmaceutical Schedule as HP4pharmaceuticals.Definition now reflects up to four possible payment datesper month.The word “Practitioner” has been replaced by theword “Practitioner’s”.Definition now makes it clear that Preferred Supplierdesignation can be communicated via the PharmaceuticalSchedule and that that brand shouldbe preferentially dispensed.Prescription Items now appear on Prescription Forms,orders, or NRT Exchange Cards, as opposed to justPrescription Forms.Fixed a typo.Updated date to latest version of the Standard.PAGE 5
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentInsertion of Sector <strong>Services</strong> definition.Updated <strong>Services</strong> definition.Insertion of Special Foods Infant Formulaedefinition.Insertion of Special Foods <strong>Services</strong>definition.Insertion of Sterile Manufacturing<strong>Services</strong> definition.Removed Urgent <strong>Pharmacy</strong> definition.The definition of <strong>Services</strong> is now limited to those that youare contracted to supply.There is no longer a distinction between an Urgent<strong>Pharmacy</strong> and a pharmacy operating after hours.The effect of this is that an Urgent <strong>Pharmacy</strong> is notrestricted to charging 50 cents and is free to set their ownlevel of pharmacy charge <strong>for</strong> after hours services.Insertion of Wholesale Supply Orderdefinition.Part F F1.2 Insertion of Our assistance clause. This insertion was previously effected by theDecember 2007 variation.Part G G3.1 Amended Quality ImprovementPlan clause.G5.6 Insertion of Health EmergencyPlanning clause.G6.3 (k) Amendment to ComplaintsProcedure clause.Added the requirement to review (but not necessarilyupdate) your Quality Improvement Plan on an annualbasis.This insertion was previously effected by the December2007 variation.This clause has been appearing in variations over the last12 months or so; you have probably already signed up tothis clause or something similar. We recommend, if youhave not already done so, that you:1. Ask your DHB <strong>for</strong> their pandemic and emergency plansa. If they are not available, then check with them howyou are to proceed with meeting your obligationsunder this clause.2. Download the pandemic plan template from the<strong>Guild</strong> website.3. Modify the <strong>Guild</strong> template to your own needs, takinginto account the specifics of your pharmacy and yourDHB’s plans.4. Communicate your plan to staff.This procedure is now consistent with the DHB’scomplaints procedure, as opposed to the Ministry ofHealth’s complaint procedure.This amendment was previously effected by the December2007 variation.G7.3 Amended Declining <strong>Services</strong> clause. Inserted an “and” after subclause (c) to avoid confusion.Inserted subclauses (e) through (i). The purpose of thisamendment is to stop “cherry picking”. Please note thatthis clause does not limit your ability to decline service topatients that threaten the safety of you, your staff, yourcustomers, or the security of your premises, in any way.PAGE 6
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyClause Change CommentG7.4 Amended ConscientiousObjection clause.Part H H1.2 Amended Payment <strong>for</strong>Pharmaceuticals clause.Replaced “grounds of conscience that you candemonstrate to our satisfaction are based on a recognisedreligious or cultural belief” with “grounds of conscience thatare reasonably based on a recognised religious or culturalbelief”.This amendment was previously effected by the December2007 variation.Subclauses (b) through (g) added. These clauses utilisethe Date of Dispensing definition and allow uncollectedmedicines to be claimed. The effects of the clauses are:1. No claim may be made prior to the medicine beingcollected/delivered, unless it is an UncollectedPrescription Item.2. You must take and document reasonable steps toensure collection/delivery be<strong>for</strong>e an item can beconsidered uncollected.3. In the case of a repeat, the work must have beencarried out after a specific and express request <strong>for</strong>the repeat.4. You may not claim <strong>for</strong> an uncollected item ifthat service user has already failed to collect anidentical item.More detail on the exact processes to follow are to befound in the Procedures Manual, which is still beingworked on and has not been released at the time ofwriting. The agreed intention of this clause is to allow youto claim:1. a dispensing fee plus the cost of the medicine <strong>for</strong>work that you would reasonably expect to be collected,but wasn’t and cannot be returned tostock, or2. a dispensing fee only, where the uncollected workcan be returned to stock.H1.4 Insertion of a Claim Certification clause. You must date and personally sign each claim yousubmit, or approve and have the claim signed on yourbehalf. Use of an electronic signature and key assignedto a pharmacist is acceptable.H3.1 Amended Claim Period clause. This clause has been amended to allow <strong>for</strong> four-times-amonthclaiming. Note that four-times-a-month claiming isonly possible if you are certified as being capable of onlineclaiming, otherwise the existing twice-monthly claimperiods remain.H4.4 (c) Amended Co-Payments clause. Consistent with multiple flavours of oral supplements/complete diet special foods, only one co-payment iscollectable <strong>for</strong> multiple flavours of gluten free foods.H4.4 Deleted subclause (e). This clause setting NRT co-payments at $5.00 has beendeleted. NRT co-payments now follow the standard rules.PAGE 7
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentH4.6 Amended <strong>Pharmacy</strong> Charges clause. Subclause (a) (iv) has been deleted. This removes therestriction currently imposed on Urgent Pharmacies tocharge an additional 50 cents. All pharmacies are free todetermine their own level of after hours’ fees as persubclause (a) (v).H4.7 Amended Provision of In<strong>for</strong>mation toEligible Persons clause.H4.8 Amended Receipts <strong>for</strong> Pharmaceuticalsclause.Subclause (a) (v) has been amended. Ordinary businesshours are now 8.30am to 5pm Monday to Friday.All pharmacies are permitted to charge an after hours’fee <strong>for</strong> items collected outside of these times. In addition,if you can demonstrate that these times are not correct <strong>for</strong>your location you can agree to different times with yourDHB.Subclause (b) has been inserted. The intention of thissubclause is to prevent blanket charging. This insertionwas effected by the October 2008 variation.The wording of subclause (c) has been reordered toimprove readability.Subclause (d) has been inserted. This requires yourpharmacy charges:1. to be “fair and reasonable”2. to be explained to service users, along with reasonablesupporting evidence, if they request3. to be explained to Audit or your DHB, along withreasonable supporting evidence, if they request.Added last sentence to clause.Added subclause (b), which clarifies that the PSA does notrequire you to provide a receipt <strong>for</strong> unsubsidised items.This amendment was previously effected by the December2007 variation.H7.4 Insertion of subclause (b). Added subclause regarding online claiming. Note thatbe<strong>for</strong>e you can claim online you must first be certifiedby your DHB and by Sector <strong>Services</strong>.H8.2 Amended Resubmission of Claim clause. Amended subclauses (a) and (b)(ii). You can only resubmita part claim online:1. as part of another claim, and2. after the commencement of the next claim period.H9.1 Amended Time limit <strong>for</strong> receiving ClaimItems clause.H9.3 Amended Non submission after 12 monthsclause.“after the date when the Pharmaceutical is Dispensed”changed to “after the Date of Dispensing”.“after the date of the Service” changed to “after theDate of Dispensing”.PAGE 8
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyClause Change CommentH10.2 Inserted new Submission ofPrescriptions clause.H10.3 Inserted new Date <strong>for</strong> submission ofPrescriptions clause.While this clause is new to the PSA, the requirements ofthe clause were always contained within the ProceduresManual.Note that the Procedures Manual will make clear that eachbatch should be filed in order of the date of processing.While this clause is new to the PSA, the requirementsof the clause were always contained within the ProceduresManual.Note you may retain batches <strong>for</strong> up to five monthsfrom the Date of Dispensing.H12 (a) Amended Payment time frames clause. Amended to accommodate four-times-a-month claiming.H18 Updated Payment agents clause. “HealthPAC” updated to “Sector <strong>Services</strong>”.Part I I1.4 Amended <strong>Pharmacy</strong> <strong>Services</strong> AdvisoryGroup.The Group now consists of:1. up to five representatives nominated by pharmacysector agents2. two DHB representatives3. one Sector <strong>Services</strong> representative4. one Audit and Compliance representative, and5. one PHARMAC representative.Part JNo change.Part KNo change.Part LNo change.Part MNo change.Part N N12.3 Amended When notice effective clause. Reference to email as a valid <strong>for</strong>m of officialcommunication has been removed. The remainingmethods are facsimile, personal delivery, or fastpost.Part OPart PSchedule C1ServiceSpecificationsC1No change.Amended List of service specificationsclause.This amendment was previously effected by the December2007 variation.This Part of your <strong>Agreement</strong> is specific to you andthere<strong>for</strong>e beyond the scope of this guide.Please contact the <strong>Guild</strong> if you have questions relatingto this Part of your <strong>Agreement</strong>.<strong>Services</strong> that were previously specified as variationsnow appear in this schedule.PAGE 9
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentC2Schedule C1Base <strong>Pharmacy</strong><strong>Services</strong> C3.2Inserted Service Specifications applicableto this <strong>Agreement</strong> clause.Amended Dispensing a SpecificBrand clause.C6.1 Amended Minimising barriers toaccess clause.This lists the services that you are contracted to provideyour DHB. If you believe a service that you provide ismissing from this clause you should contact your DHBimmediately. The complete list of potential services is:• Base <strong>Pharmacy</strong> <strong>Services</strong>• <strong>Pharmacy</strong> Methadone <strong>Services</strong> <strong>for</strong> Opioid Dependence(Class B Controlled Drug <strong>Services</strong>)• Aseptic <strong>Pharmacy</strong> <strong>Services</strong> (including Syringe Driver<strong>Services</strong>)• Sterile Manufacturing <strong>Services</strong>• Special Foods <strong>Services</strong>• Special Foods Infant Formulae <strong>Services</strong>• Provision of Blood Glucose Test Strips• Complex Medicine <strong>Services</strong>• <strong>Pharmacy</strong> Clozapine <strong>Services</strong> (Monitored TherapyMedicine <strong>Services</strong>).Subclause (d) has been modified to make it clear that thePharmaceutical Schedule is the means by which DHBs willcommunicate Preferred Supplier Brand status to you.The clause is now more reasonable; you now agree tominimise barriers “to the extent that such matters arewithin your reasonable control” rather than “to thegreatest extent possible”.This amendment was previously effected by the December2007 variation.6.2 Amended Opening hours clause. Subclause (b) has been inserted. This clarifies that DHBsmay individually contract after hours’ services from youif they wish. If your DHB chooses to contract after hours’services with you, the terms and conditions of this servicewill appear in Part P of your agreement.7.1 (b) Amended Processes: Provision of adviceand counselling clause.7.1 (i) Inserted Processes:NRT Programme clause.You are not obligated to accept the offer of after hours’service provision.The word “sub-paragraphs” changed to “sub-clauses”in 7.1 (b).Rather than having its own service specification,the clauses detailing the NRT programme processesnow appear as part of the Base <strong>Pharmacy</strong> <strong>Services</strong>specification in this part of the <strong>Agreement</strong>.The only substantive change from the previousservice specification is recognising that NRT cannow be dispensed pursuant to a prescription or anNRT Exchange Card.The waiting times <strong>for</strong> NRT have been relaxed, and nowcon<strong>for</strong>m to the Base <strong>Pharmacy</strong> <strong>Services</strong> waiting times.PAGE 10
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentSchedule C17.1 (j) Inserted Processes: <strong>Pharmacy</strong> Methadone<strong>Services</strong> <strong>for</strong> Opioid Dependence clause.Previously, methadone services had a separate servicespecification as part of the base contract. This allowed apharmacy to service up to two “regular” clients and anynumber of “intermittent” clients. Pharmacies wishing toservice more clients did so by means of a variation.Now, rather than having its own service specification, theclauses detailing the basic (two client) level of methadoneservice appear as part of the Base <strong>Pharmacy</strong> <strong>Services</strong>specification in this part of the <strong>Agreement</strong>.The previous variation now <strong>for</strong>ms the basis <strong>for</strong> the new<strong>Pharmacy</strong> Methadone <strong>Services</strong> <strong>for</strong> Opioid Dependence(Class B Controlled Drug <strong>Services</strong>) specification that willappear in the <strong>Agreement</strong>s of those pharmacies thatpreviously had the variation to allow more than tworegular clients. See below <strong>for</strong> more details of this service.A substantive change to this basic (two client) level ofmethadone service is contained in subclause 7.1 (j) (iii).You are now limited to a maximum of two Service Usersper claim period unless authorised in writing.7.2 (a) Amended Waiting times clause. Amended “Prescription Form” to “Prescription Form, order,or NRT Exchange Card”.7.2 (b) Amended Waiting times clause. Added “and your failure to do so [maintain adequate stocklevels] will not be considered to be an UncontrollableEvent.”8 Amended Service linkages clause. Subclause (l) added. Authorised NRT Agents in your areahas been added to the list of services with which you haveeffective links to.9 Updated Exclusions clause. Update reflects the new construction of this Schedule ofthe <strong>Agreement</strong>.<strong>Pharmacy</strong>Methadone <strong>Services</strong><strong>for</strong> OpioidDependence (ClassB Controlled Drug<strong>Services</strong>) 6.1Updated Processes clause.The relevant protocols are now contained in OpioidSubstitution Treatment New Zealand Practice <strong>Guide</strong>lines2008 (rather than 2003).PAGE 11
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentSchedule C1Aseptic <strong>Pharmacy</strong><strong>Services</strong> (includingSyringe Driver<strong>Services</strong>)Schedule C1SterileManufacturing<strong>Services</strong>Schedule C1Special Foods<strong>Services</strong>Schedule C16.2 Amended Number of Service Users clause. If you are contracted to provide this service (as opposed tothe methadone services that are part of the Base <strong>Pharmacy</strong><strong>Services</strong>) you may service any number of clients, providedthat the number is not so large as to threaten your abilityto deliver the service.8 Updated Exclusions clause. Update reflects the new construction of this Schedule ofthe <strong>Agreement</strong>.Special Foods InfantFormulae <strong>Services</strong>Schedule C1Provision of BloodGlucose Test StripsNew section inserted.New section inserted.New section inserted.New section inserted.New section inserted.What was previously known as Aseptic <strong>Services</strong> has nowbeen split into two services: Aseptic (including syringedriver) <strong>Services</strong> and Sterile Manufacturing <strong>Services</strong>.Aseptic <strong>Services</strong> require, at a minimum, an approved stillair box within a Grade D air environment.You must dispense 99% of items within 24 hours, and100% within two business days if presented during abusiness day.What was previously known as Aseptic <strong>Services</strong> has nowbeen split into two services: Aseptic (including syringedriver) <strong>Services</strong> and Sterile Manufacturing <strong>Services</strong>.Sterile <strong>Services</strong> require, at a minimum, a laminar flowcabinet or isolator (Grade A air environment) within aGrade B air environment room.You must dispense 99% of items within 24 hours, and100% within two business days if presented during abusiness day.Special Foods <strong>Services</strong> will no longer be contracted by wayof variation. Rather, you may claim <strong>for</strong> Special Foods<strong>Services</strong> if it is included in Part P and clause C2 of ScheduleC1.There are no substantive changes from the Special Foodsvariation.This service specification relates to a subset of the SpecialFoods Service and will not be available to most <strong>members</strong>.If you do not provide this Service, you may still provideinfant <strong>for</strong>mulae as Special Food (if you provide SpecialFoods <strong>Services</strong>) or, where the Pharmaceutical Scheduleallows, as a Base <strong>Pharmacy</strong> Service (if you do not provideSpecial Foods <strong>Services</strong>).This service specification relates to an arrangement thatsome pharmacies have with their DHB and will not beavailable to most <strong>members</strong>.If you do not provide this Service, you may continue toprovide test strips, where the Pharmaceutical Scheduleallows, as a Base <strong>Pharmacy</strong> Service.PAGE 12
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyClause Change CommentSchedule C1Complex Medicine<strong>Services</strong>Schedule C1<strong>Pharmacy</strong> Clozapine<strong>Services</strong> (MonitoredTherapy Medicine<strong>Services</strong>)Schedule C2New section inserted.New section added.New section added.Protocol <strong>for</strong> theDispensing ofClozapine byCommunityPharmacies1.3 Amended Check the patient is registeredwith the supplier(s) of clozapine clause.1.4 Amended Check that the prescription iswritten by an authorised prescriber clause.Complex Medicine <strong>Services</strong> will no longer be contracted byway of variation. Rather, you may claim <strong>for</strong> ComplexMedicine <strong>Services</strong> if it is included in Part P and clause C2of Schedule C1.The only change from the variation is clause 6.2 Facilitiesand settings. Your pharmacy no longer needs to beregistered with the Pharmaceutical Society; rather itshould be licensed by the licensing authority andregistered with the Ministry of Health.Clozapine <strong>Services</strong> will no longer be contracted by wayof variation. Rather, you may claim <strong>for</strong> Clozapine <strong>Services</strong>if it is included in Part P and clause C2 of Schedule C1.This specification is almost identical to the previousvariation. The changes are:• Clause 2 Service Objectives have been expanded,reiterating the pharmacist’s responsibilities.• Clause 6.4 Facilities and settings. Your pharmacy nolonger needs to be registered with the PharmaceuticalSociety; rather it should be licensed by the licensingauthority and registered with the Ministry of Health.• Clause 9.3 Qualified provider. The training ofrelevant staff should now occur at least annually,assuming training sessions are made available atthe pharmacy level.This protocol is based on the protocol that was theappendix of the previous clozapine services variation.Added to the end of the clause, “The pharmacistis required to enter the date of any dispensing onthe website <strong>for</strong> a complete record to be availableto all providers.”Reference to the Prescribers Act 1995 has been updated tothe HPCA Act, and prescribers must be “certified ascompetent in the branches of psychological medicine orpsychiatry by the Medical Council of New Zealand.”Deleted subclause (b). Rules regarding subsidy eligibilityare to be found in the Pharmaceutical Schedule.1.10 Updated Label the container clause. Note that the wording of Cautionary and Advisory label 9was altered in 2001.3 Amended Patient In<strong>for</strong>mation Recordsclause.Subclause (d) added.“The supplier Clozapine website needs to be updated withthe date of dispensing each time this occurs.”PAGE 13
confidential – <strong>for</strong> guild <strong>members</strong> onlyClause Change CommentSchedule H1Payment terms3.2Schedule J1Audit Framework3.2Updated Base <strong>Pharmacy</strong> <strong>Services</strong> Fee andMultipliers clause.3.3 Updated <strong>Pharmacy</strong> servicesand Pharmaceutical payments –General clause.3.6 Inserted Payment calculation <strong>for</strong> Provisionof Blood Glucose Test Strips clause.The Base <strong>Pharmacy</strong> <strong>Services</strong> Fee is $5.30. This is thesame fee as contained in the variation of 1 October 2008,which was an increase from the previous PSA.The table of multipliers has been updated to reflect thepossible inclusion in your <strong>Agreement</strong> of Special FoodsInfant Formulae <strong>Services</strong> (multiplier of 1.00) and SterileManufacturing <strong>Services</strong> (multiplier of 3.00).Updated “Prescription Form” to “Prescription Form, order,or NRT Exchange Card”.Updated the list of Purchase Unit descriptions to includeSpecial Foods Infant Formulae <strong>Services</strong> and SterileManufacturing <strong>Services</strong>, and to delete NRT <strong>Services</strong>.Updated to reflect that NRT services are now part ofBase <strong>Pharmacy</strong> <strong>Services</strong>. The payment calculation <strong>for</strong>mulahas not changed.Some pharmacies supply test strips as per the Provision ofBlood Glucose Test Strips Service, rather than as part ofBase <strong>Pharmacy</strong> <strong>Services</strong>. This clause will not apply to themajority of <strong>members</strong>.Payment from the DHB under this service is the cost of thetest strips, plus a 10% mark-up, plus GST. There is nodispensing fee or co-payment.In addition, the provider of this service is able to charge apharmacy charge of $1.50 including GST to the ServiceUser.3.8 Inserted Online Claiming clause. This insertion pulls the online claiming variation that hasbeen rolling out throughout the country into the PSA.4 Deleted Subsidised Nicotine ReplacementTherapy <strong>Services</strong> clause.Amended Time frames <strong>for</strong> on-siteAudits clause.After being certified by your DHB and Sector <strong>Services</strong> asbeing capable of online claiming you are entitled to:1. A one-off payment of $500 plus GST <strong>for</strong> set-up costs,unless you have already claimed and received a one-offset-up payment previously (eg pharmacies in the metroAuckland area). Note that if you have already begunonline claiming but did not receive a one-off payment,you are now entitled to this payment (eg pharmacies inthe Capital and Coast area).2. A monthly payment of $100 plus GST.NRT <strong>Services</strong> are now part of Base <strong>Pharmacy</strong> <strong>Services</strong>.Subclause (e) inserted:“we will consider and decide upon actions in respectof the Audit report and provide our responses within20 Business Days of receiving it from the Auditor.”PAGE 14
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlySection Three: PSA <strong>2010</strong> user guideThe purpose of this part of the document is to provide <strong>members</strong> with a general guide to the structure and requirements ofthe PSA. It is intended to be a useful introduction to <strong>members</strong> unfamiliar with this or previous PSAs. For <strong>members</strong> familiarwith previous PSAs “Section Two: Clause-by-clause analysis”, may provide a better starting place <strong>for</strong> understanding in detailthe changes made in PSA <strong>2010</strong>.Layout of the <strong>Pharmacy</strong> <strong>Services</strong> <strong>Agreement</strong>The layout of the PSA is the same as the previous <strong>Agreement</strong>s since 2003. The PSA is broken up into 16 Parts, followed byfive Schedules. Each Part groups clauses covering similar aspects of the relationship together and each of the correspondingSchedules defines how the requirements of this part of the <strong>Agreement</strong> operate in practice. For example, Schedule H1 providesmore detail on the payment terms contained in Part H.Many of the individual clauses of the PSA are either identical or very similar to those applying to other primary careproviders. This gives greater commonality in the relationship between the DHB, pharmacies and other health providers, andfacilitates integration and teamwork between services.To help you work your way through the <strong>Agreement</strong>, the contents of each of the Parts and Schedules of the <strong>Agreement</strong> are:Part or Schedule Name Summary of section contentsPart A <strong>Guide</strong> to this <strong>Agreement</strong> General summary of the PSA and respectiveresponsibilities.Part B Key terms and execution of this <strong>Agreement</strong> Duration and term of the PSA, linkage to thePharmaceutical Schedule, the Data Specification and theProcedures Manual.Part C Summary of services to be provided Outline of <strong>Services</strong>, patient eligibility rules, and servicelocation rules.Part D General purposes and principles Purpose of the <strong>Agreement</strong>, service delivery principles andrelationship principles.Part E Definitions and construction Definitions <strong>for</strong> terms used in the PSA, and rules coveringthe construction of the PSA.Part F Maori health and other population groups Management of Maori health and other population grouphealth issues.Part G Quality specifications Quality management requirements and systems, serviceuser rights, access to services and service criteria.Part HPayment <strong>for</strong> services and Pharmaceuticals,claiming procedure and payment termsPayment <strong>for</strong> services, claiming dates, charges to patients,unnecessary dispensing, claim in<strong>for</strong>mation, claim rejection,payment time frames, interest on late payment, and accessto records.Part I Meetings, reporting, and in<strong>for</strong>mation Calling meetings between the parties and ad hocin<strong>for</strong>mation requests.Part J Audits Purpose of audit, requirements and Advisory Committeematters.Part K Dispute resolution Dispute resolution process and use of facilitatednegotiation during PSA renewal or variation.Part L Variation of <strong>Agreement</strong> Reasons <strong>for</strong> varying the PSA, procedures <strong>for</strong> varying thePSA and renewal and consultation on future <strong>Agreement</strong>s.PAGE 15
confidential – <strong>for</strong> guild <strong>members</strong> onlyPart or Schedule Name Summary of section contentsPart MPart NPart OTerms governing your dealings withthird partiesOther miscellaneous terms governingour relationshipFailure to per<strong>for</strong>m and terminationof <strong>Agreement</strong>Subcontracting, transfer of services to others,confidentiality of in<strong>for</strong>mation and incentives toprescribers.Insurance, indemnity, warranty, compliance with law andtiming of notices.Remedies available where a party fails to per<strong>for</strong>m theirobligations, suspension or termination of <strong>Agreement</strong>s andconsequences of termination.Part P Provider specific terms and conditions Allows pharmacies and DHBs to agree to supply servicesspecific to the pharmacy.Schedule C1 Service specifications Service specifications <strong>for</strong> Base <strong>Pharmacy</strong> <strong>Services</strong> plus theoptional services (see Part P <strong>for</strong> which of these servicesapply to your pharmacy): <strong>Pharmacy</strong> Methadone <strong>Services</strong><strong>for</strong> Opioid Dependence, Aseptic <strong>Pharmacy</strong> <strong>Services</strong>(including Syringe Driver <strong>Services</strong>), Sterile Manufacturing<strong>Services</strong>, Special Foods <strong>Services</strong>, Special Foods InfantFormulae <strong>Services</strong>, Provision of Blood Glucose Test Strips,Complex Medicine <strong>Services</strong>, <strong>Pharmacy</strong> Clozapine <strong>Services</strong>(Monitored Therapy Medicine <strong>Services</strong>).Schedule C2 Protocols Protocols relating to the dispensing of clozapine.Schedule H1 Payment terms Detailed payment terms including fees, mark-ups andcalculations.Schedule J1 Audit framework Audit principles, obligations, processes and timeframes.Schedule N1 Bank account details <strong>Pharmacy</strong> bank account details.Section by Section ReviewThis part of the <strong>Guide</strong> to the PSA <strong>2010</strong> draws your attention to, and explains aspects of, the <strong>Agreement</strong>. It worksits way through the <strong>Agreement</strong> following the PSA headings, but it does not provide a clause-by-clause explanation ofthe <strong>Agreement</strong>. If you have questions about sections of your <strong>Agreement</strong> not covered in the <strong>Guide</strong> you should contactthe <strong>Guild</strong>.Throughout the PSA and this <strong>Guide</strong>, the term Service Users is used to refer to patients. While the term is cumbersome,it is used in the PSA to refer specifically to patients receiving subsidised services. We have used the term in the <strong>Guide</strong> toavoid confusion.PAGE 16
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyMaori health and other populations groups (Part F)Improving Maori health is an important objective <strong>for</strong> the Government and the DHBs. All health provider Service <strong>Agreement</strong>sare required to have a section recording the provider’s commitment to improving Maori health within the circumstances oftheir practice and describing practical initiatives they can undertake. Your DHB will assist you to meet your obligationsunder this Part F.Part F of the Service <strong>Agreement</strong> template is designed to give pharmacies the flexibility to respond to the Government’sMaori health objective and their Maori community’s needs. In particular, please consider how the three initiatives detailedin clause F4.2 might be accommodated in your practice setting.It is also important to note the Government’s emphasis on improving Maori health does not mean Maori or other ServiceUsers have greater rights under the PSA. Clause F1 is explicit on this point:“To avoid doubt, and in accordance with the New Zealand Public Health and Disability Act 2000, nothing in this <strong>Agreement</strong>entitles any person to preferential access to <strong>Services</strong> on the basis of race.”F3.1: Development of MaoriHealth section in your QualityImprovement PlanF3.2: Compliance at acollective levelF4.1: Maori needsF4.2: Maori health initiativesF4.2(a) – Maori healthprogrammesF4.2(b) – labelling and adviceF4.2(c) – disposal ofcontaminated needlesPharmacies are required to develop a Maori Health section in their Quality Improvement Planif the demographic make up of their community makes it reasonable to do so. Pharmacieswith a large Maori customer base would want to do so to retain competitiveness. By contrast,pharmacies with a very small Maori customer base may consider a Maori Health section intheir Quality Improvement Plan an unreasonable use of their managerial resources.Groups of pharmacies and other providers are able to work together to meet theirMaori health obligations, provided group action does not prevent them meeting theirindividual obligations.Reducing barriers to Maori accessing services does not include being required to reduce thecost of services or discounting co-payments.The three initiatives are practical measures, which pharmacies can implement and willcontribute to Maori Service Users from either health or cultural perspectives. The clause doesnot require pharmacies to offer these services nor does it require pharmacies to ensure allMaori people use these services. Rather, it allows pharmacies and their customers to chooseto participate.Participation in Maori health initiatives will give pharmacies the chance to become part ofwider health initiatives and expand pharmacy’s participation in the integrated primary careteam. Participation is not compulsory and may be declined if it would be illegal or unethical,or the pharmacy considers involvement would be unreasonable in any way.Evidence suggests some Maori find present approaches to labelling and advice inappropriate<strong>for</strong> a variety of reasons.Some Maori find the burning of blood or other body tissues or fluids culturally unacceptable.In consequence, normal disposal methods <strong>for</strong> contaminated needles, finger prickers and thelike can be offensive.PAGE 19
confidential – <strong>for</strong> guild <strong>members</strong> onlyQuality specifications (Part G)This part of the PSA draws together all the quality management requirements of the <strong>Agreement</strong>. The focus of the part isgood business practices, rather than good dispensing practices.G2: Governance andmanagementG3: Quality managementsystemsG4: Quality requirements <strong>for</strong>MaoriThis clause requires pharmacies to have governance and management systems to ensureefficient service delivery, continuity of service, and compliance with legal, regulatory andService <strong>Agreement</strong> template obligations. This requirement is further covered in clauses G9and G10.Your existing quality plans should already meet this requirement, but are now required to bereviewed at least annually.DHBs expect pharmacies will use documented procedures to help manage service quality,update these documents as required, make sure the documents are used by staff and allow<strong>for</strong> suitable staff input into their development. These expectations follow widely used qualityimprovement methods.This requirement is part of the Government’s focus on Maori health improvement.G5: Risk management You must comply with the Health and Safety in Employment Act 1992.Furthermore, you will document policies and procedures to guide you and your staff inmeeting health and safety requirements and reporting incidents. You will co-operate with anycivil defence emergency activity in your area.New to the PSA is the requirement to develop and implement a written health emergencyplan which is consistent with the DHBs’ own pandemic and emergency plans. We recommend,if you have not already done so, that you:1. Ask your DHB <strong>for</strong> their pandemic and emergency plansa. If they are not available, then check with them how you are to proceed withmeeting your obligations under this clause.3. Download the pandemic plan template from the <strong>Guild</strong> website.4. Modify the <strong>Guild</strong> template to your own needs, taking into account the specifics of yourpharmacy and your DHB’s plans.5. Communicate your plan to staff.G6: Service users’ rights You must understand the Code of Health and Disability <strong>Services</strong> Consumer Rights, andintegrate the Code with your policies and procedures.You must make available to Service Users a written copy of the Code. Brochures are available<strong>for</strong> free to download from www.hdc.govt.nz, or you can purchase brochures and/or postersdirectly from the Heath and Disability Commissioner; click on “Order Resources” on theirhome page. Their FAQ is well worth reading and provides a good introduction to the Code andhow it impacts on you as a provider. See http://www.hdc.org.nz/aboutus/aboutus-faq.You must ensure that your service delivery approach adequately protects the privacy of theService User, including the Service Users’ personal in<strong>for</strong>mation and health in<strong>for</strong>mation.PAGE 20
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyG7.2: Service In<strong>for</strong>mationYou will have available <strong>for</strong> interested parties written in<strong>for</strong>mation that describes:a. the <strong>Services</strong> you offer;b. the location of these <strong>Services</strong>;c. the hours of access;d. how to access the <strong>Services</strong> (eg, whether a referral is required);e. Service Users’ rights and responsibilities; andf. any other in<strong>for</strong>mation to enable Eligible People to access the <strong>Services</strong>.G7.3: Declining servicesG7.4: ConscientiousobjectionThe purpose of this clause is twofold. First, it ensures that you develop and implementprocesses to ensure the immediate safety of persons to whom you are declining service,and documenting the declination. This provides a pharmacy with a firm footing should theService User lodge a complaint. This clause should be read in conjunction with section 1.7of the Code of Ethics and the Code of Health and Disability <strong>Services</strong> Consumer Rights.Second, the clause prohibits “cherry picking”. Here, “cherry picking” refers to theunscrupulous practice of declining less profitable services in order to concentrate on themore profitable services. The remuneration offered in the PSA is an averaged rate based onthe assumption that all services will be undertaken. While “cherry picking” may seem likesound business practice, it has the effect of shifting costs onto neighbouring pharmaciesand thus destabilising the sector.You have the right to not provide a service <strong>for</strong> reasons of conscience. Pharmacies exercisingthis right must follow the rules <strong>for</strong> declining services spelt out in clause G7.3.G8: The services Service delivery is required to meet current good practice. The clause provides guidance onthe current view of good practice in staffing, staff training and requirement <strong>for</strong> a plannedapproach to service delivery.Standard operating procedures prepared by pharmacies to meet their professional and auditresponsibilities are regarded as a planned approach to service delivery.G9: Staff management You will establish and implement staff management processes that are consistent with goodhuman resource practice.G12: Service User satisfactionsurveysG13: Records andadministrationYou must carry out Service User satisfaction surveys at least annually. Many pharmacies findthem a useful source of customer feedback and a worthwhile management tool. To ourknowledge, no DHB has yet insisted that this activity takes place. Note that other healthproviders are also contractually obligated to conduct Service User satisfaction surveys.You must keep good records that enable you to adequately distinguish between <strong>Services</strong> youprovide under the <strong>Agreement</strong> and other activities you are engaged in. This clause does notrequire you to treat your subsidised dispensary as a separate business unit from the rest ofthe pharmacy with its own set of accounts, etc.
confidential – <strong>for</strong> guild <strong>members</strong> onlyPayment <strong>for</strong> <strong>Services</strong> and Pharmaceuticals, claiming procedure and payment terms(Part H)This part of the Service <strong>Agreement</strong> template describes the rules surrounding payment <strong>for</strong> services, claiming procedures andthe claiming of penalty interest when either party does not meet their payment obligations. Part H should be read inconjunction with Schedule H1, the Pharmaceutical Schedule and the Procedures Manual.H1: Payment <strong>for</strong> <strong>Services</strong> andPharmaceuticalsH1.4: Claim certificationH2.1: Reliance on In<strong>for</strong>mationfrom PrescribersYou may claim, and be paid, <strong>for</strong> any subsidised Pharmaceutical dispensed pursuant to the<strong>Agreement</strong>. Note that the Pharmaceutical Schedule states that <strong>for</strong> the purposes of this<strong>Agreement</strong> HP1, HP3, and HP4 pharmaceuticals are only subsidised when dispensed from apharmacy that has been contracted to provide Complex Medicine services, Special Foodsservices, or Clozapine <strong>Services</strong>, respectively. Part P lists which services you are contractedto provide.Ordinarily, you may only claim against a Prescription Item once it has been collected.However, if a Prescription Item becomes an “Uncollected Prescription Item” you may claimagainst it. More details of this can be found in the Procedures Manual.Note that repeats can only be claimed <strong>for</strong> following a specific and express request by aService User, their caregiver, or their prescriber that has been initiated by them after theoriginal item has been dispensed.In addition, you cannot claim <strong>for</strong> an uncollected item if you have previously prepared anidentical item <strong>for</strong> that Service User that remained uncollected.All claim submissions must be signed and dated by you, or approved by you and signed onyour behalf. Online claims may be digitally signed.For the purposes of this <strong>Agreement</strong>, particularly with regards to submitting claims, you mayrely on the in<strong>for</strong>mation you receive from a Prescriber as being accurate, unless you havereason to believe otherwise.H3: Claiming generally With online claiming there are four claim periods per month. Without online claiming thereare two. Note this should be regarded as the maximum number of times you can claim permonth; you do not have to claim in every period if you do not think the more promptpayment is worth the extra administrative work required to generate claims more often.H4.1: Eligible personsH4.3 Determining andcollecting co-payments,pharmacy charges, andproduct premiumsFor online claiming the four due dates per month are: the 7 th , the 15 th , the 23 rd , and the lastday of that month.Otherwise, the two due dates are the 15 th and the last day of the month.Any claims that are submitted after the due date fall into the following claim period.The dates you receive payment relate to the due dates and are typically 20 days after thedue date. See clause H12.For any and all <strong>Services</strong> you provide under this <strong>Agreement</strong> you may only charge ServiceUsers the charges that are permissible under the <strong>Agreement</strong>.However, this does not preclude you from providing services that are related to the<strong>Services</strong> of the <strong>Agreement</strong>, yet outside the <strong>Agreement</strong>, and charging as you deemappropriate. Two examples of this are accepting a credit card payment <strong>for</strong> <strong>Services</strong>,or storing dispensed Pharmaceuticals on behalf of the Service User.You are responsible <strong>for</strong> determining and collecting the correct charges.The Ministry of Health website is the best place <strong>for</strong> up-to-date in<strong>for</strong>mation on co-payments.See http://www.moh.govt.nz/eligibility. See also clause H4.4 below <strong>for</strong> more in<strong>for</strong>mation.Your dispensary software should automatically calculate product premiums. See clause H4.5below <strong>for</strong> more in<strong>for</strong>mation.You are free to determine the level of any <strong>Pharmacy</strong> Charges you might levy, providing theyare reasonable and permissible. See clause H4.6 below <strong>for</strong> more in<strong>for</strong>mation.PAGE 22
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyH4.4 Co-payments For prescriptions that are valued at less than the co-payment, pharmacies continue to havediscretion regarding the charge to the service user, up to the value of the co-payment.The Ministry of Health website is the best place <strong>for</strong> up-to-date in<strong>for</strong>mation on co-payments.See http://www.moh.govt.nz/eligibility. Note the exclusions to co-payments listed in clauseH4.4 (b): Service Users under six, Hokianga Ward Medical trust prescriptions, antituberculoticsand antileprotics, or Class B Controlled Drugs (other than methylphenidate hydrochloride ordexamphetamine sulphate).When a Service User with a special food prescription asks <strong>for</strong> their product to be dispensedas a combination of flavours, each dispensing only carries one co-payment. Please note thisonly applies if the product is listed in the Oral Supplement/Complete Diet section or theGluten Free Foods section of the Pharmaceutical Schedule.You may charge less than the maximum permissible co-payments if you choose. This doesnot affect the payment you receive from your DHB <strong>for</strong> the <strong>Services</strong>; effectively you paythe difference between the maximum co-payment and the actual co-payment from yourown pocket.Whenever a Service User does not pay a co-payment that item does not count towards thePSC scheme.H4.5: Product premiumsH4.6: <strong>Pharmacy</strong> chargesH4.8: Receipts <strong>for</strong>PharmaceuticalsH6.3: No unnecessarydispensingNote the extra requirements if the total cost of a three month supply of an item with repeatsdispensed all-at-once (stat) is less than the co-payment.If the price of a pharmaceutical is more than the subsidy, you may charge the Service User aProduct Premium. You are free to determine the level of the premium.Your dispensary software should automatically calculate product premiums according to asimple <strong>for</strong>mula, but these premiums can be overwritten if you choose.The <strong>Guild</strong> produces and updates a Product Premium <strong>Guide</strong>. Please contact the <strong>Guild</strong> if youwould like to learn more about the <strong>Guide</strong>.Members should read this section carefully to ensure they fully understand their rights andresponsibilities when setting their charging policies.The <strong>Guild</strong> produces a guide and template regarding pharmacy charges, which can bedownloaded from our website.In general, you are free to determine the level of any <strong>Pharmacy</strong> Charges you might levy,providing they are reasonable and permissible.The anticipatory, or flat-fee, charge is expressly <strong>for</strong>bidden. Ad hoc intervention chargesremain permissible.Also note that you may charge <strong>for</strong> other services you provide to the Service Users that are inexcess of the requirements of the PSA or the Pharmaceutical Schedule. An example of thismight be accepting a credit card payment as a co-payment.You should in<strong>for</strong>m Service Users of applicable <strong>Pharmacy</strong> Charges be<strong>for</strong>e you begin work andexplain how he or she may avoid or reduce the pharmacy charge. A sign, such as the oneincluded in the <strong>Guild</strong>-produced template, is sufficient.You must provide a receipt to Service Users <strong>for</strong> any subsidised item dispensed. The receiptmust include the name of the Pharmaceutical, the cost to the Service User and the cost tothe Government.Pharmacies must not boost their revenue artificially by dispensing prescriptions unnecessarilyor more frequently than the Pharmaceutical Schedule or Procedures Manual allows.PAGE 23
confidential – <strong>for</strong> guild <strong>members</strong> onlyH7.2: Prescriber in<strong>for</strong>mationYou must provide NZMC numbers <strong>for</strong> more than 90% of the items in a claim. If a pharmacyfails to meet this target, the claim can be rejected.If a pharmacy is not receiving an NZMC number from a doctor, the numbercan be requested from the doctor, or obtained from the Medical Council(phone 04 384 7635). If these options fail the pharmacy should contact their DHB.Where the doctor supplies a PAN number on a prescription to identify the practice, this mustalso be provided.In instances where the doctor has separate PAN numbers <strong>for</strong> different practices(or a practice with a PAN number and a practice without a PAN) pharmacies mustprovide the appropriate number <strong>for</strong> the prescription. This is easily achieved bysetting up separate doctor records <strong>for</strong> each of the PAN numbers in the dispensarysystem and selecting the appropriate doctor record <strong>for</strong> the prescription.DHBs have indicated they will be happy <strong>for</strong> the proportion of PAN numberssupplied to grow over time as pharmacies receive prescriptions carrying them andrecord them in their dispensary systems.H7.3 Service User’sin<strong>for</strong>mationYou must provide patient NHI numbers where they are provided on the prescription bythe prescriber.Pharmacies are not required to validate NHI numbers are correct or obtain themwhen the prescriber does not supply them. Pharmacies simply have to supplythose NHI numbers they receive. Prescriptions not carrying an NHI number willstill be subsidised.However, the requirement to provide NHI numbers will be auditable.Pharmacies only need to record the NHI number once in the dispensary systempatient record. It will then be supplied to Sector <strong>Services</strong> each time a prescription<strong>for</strong> the patient is claimed. However, if the pharmacy receives a prescription <strong>for</strong> thepatient from a hospital or the patient moves to a new doctor, the pharmacy shouldcheck the NHI number provided against the patient record. If the NHI number isdifferent to the one in the record, the new number must be recorded in place ofthe existing number.H9: Late claim items Claims <strong>for</strong> an item must be submitted within six months of dispensing (nine months in thecase of an oral contraceptive). Claims not made within this time, may be submitted up to12 months after dispensing provided the claim is worth more than $20 and an explanation<strong>for</strong> the delay accompanies the claim.H10: Verification of claimitemThe DHB may ask a pharmacy to substantiate any claim item. Sending a copy of theprescription to the DHB will satisfy this requirement. When requested, the pharmacy has15 days to provide the prescription.Notwithstanding the above, all original prescriptions associated with a claim must besubmitted to Sector <strong>Services</strong>. If you submit claims electronically you may retain prescriptionbatches <strong>for</strong> up to five months be<strong>for</strong>e submitting them.Batches should be filed in order of the date of processing.PAGE 24
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyH12: Payment time frames Where four-times-a-month claiming is allowed (ie online claiming):• claims received by the 7th will be paid on the 28th• claims received by the 15th will be paid on the 5th of the following month• claims received by the 23rd will be paid on the 12th of the following month• claims received by the last day of the month will be paid on the 20th of thefollowing month.Where only twice-monthly claiming is allowed:• claims received by the 15th will be paid on the 5th of the following month• claims received by the last day of the month will be paid on the 20th of thefollowing month.If the payment date is not a business day, then payment shall be made on the first businessday after the above dates.H18: Payment agent Sector <strong>Services</strong> (a business unit of the Ministry of Health) is the payment agent <strong>for</strong> all DHBs.H19: Access to records Pharmacies retain the right to audit payments made to them <strong>for</strong> services.PAGE 25
confidential – <strong>for</strong> guild <strong>members</strong> onlyMeetings, reporting and in<strong>for</strong>mation (Part I)This section of the <strong>Agreement</strong> details both parties’ responsibilities in dealing with requests <strong>for</strong> meetings and the provisionof in<strong>for</strong>mation.I1: Relationship meetings Either party or their agent can request a meeting with the other to discuss the functioningof the PSA or the delivery of services. Written notice must be given. The DHB can decide tohold a requested meeting with a group of providers (including doctors or other prescribers)to discuss an issue if it considers it more appropriate or practical to handle the matter in agroup setting.I1.4: <strong>Pharmacy</strong> <strong>Services</strong>Advisory GroupIf it is important to discuss an issue urgently, the DHB may convene a special meetingby giving written notice. Pharmacies must use reasonable endeavours to attend thesespecial meetings.PSAG is a national group that:• considers operational pharmacy matters that may impact on the ability of pharmacy orDHBs to meet their obligations• clarifies any matters relating to the PSA• considers issues relating to the PSA• manages the maintenance of the Procedures Manual.PSAG comprises pharmacy representatives and government representatives and meets atleast four times a year.I2: Reporting If the DHB receives a request <strong>for</strong> in<strong>for</strong>mation from a Minister of the Crown, they may seekreasonable in<strong>for</strong>mation from a pharmacy to answer the Minister. The pharmacy must providereasonable assistance to the DHB, at the pharmacy’s cost, to provide the in<strong>for</strong>mation within amutually agreed period.I3: Specialist Database If your DHB provides you with a free database of Specialists, you must use it to enable youto comply with the PSA, the Procedures Manual and any relevant legislation.Audits (Part J)The Audit framework is essentially common to all DHB Service <strong>Agreement</strong>s with providers. We have been advised thatAudit and Compliance attempts to complete a desk audit of every pharmacy at least once every five years. If the desk auditflags unusual activity, a full investigation may commence.This Part is supported by, and should be read in conjunction with, the Audit framework provided in Schedule J1J3: Specific provisions relatingto Solvency AuditsJ4: <strong>Pharmacy</strong> AdvisoryCommitteeIf the DHB is concerned about the ability of a pharmacy to continue to provide services theymay request a certificate of solvency <strong>for</strong> the business. This certificate would be prepared bythe pharmacy’s accountant or another suitably qualified professional.If a solvency certificate fails to allay their concerns, the DHB may appoint an independentfinancial analyst to determine the business’ financial position and costs of operation. The DHBwill pay <strong>for</strong> the analysis but the analyst must not disclose any of the pharmacy’s in<strong>for</strong>mationto the DHB beyond stating whether the pharmacy’s financial position threatens its ability tomeet its Service <strong>Agreement</strong> template obligations.Your DHB may refer matters arising from a belief that you have failed to per<strong>for</strong>m yourobligations under the PSA to the <strong>Pharmacy</strong> Advisory Committee (PAC). PAC comprisesDHB-appointed and pharmacy agent-appointed representatives.PAGE 26
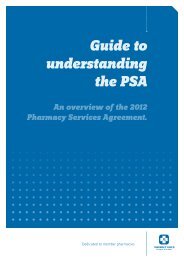
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyDispute resolution (Part K)The dispute resolution process <strong>for</strong> problems associated with the interpretation of the PSA follows a sequence of discussionof a problem, followed by mediation, followed by arbitration. This process is specified in the Health Sector Mediation andArbitration Rules 1993.K3: Facilitated Negotiation If a dispute occurs during consultation, either party may invoke facilitated negotiation if theproblem cannot be resolved by discussion.The other party must attend a facilitated negotiation session but the outcome is not bindingon either party. The costs will be shared equally.The pathway <strong>for</strong> resolving disputes is presented below.Figure 1: Process <strong>for</strong> resolving disputesDispute arisesType of disputeEligibility of a personInterpretation of anaspect of the agreementNegotiation orrenegotiation of agreementTry to resolveby agreementafter 30 dayscommences within30 days of notificationMediationRefer to Minister<strong>for</strong> resolutionArbitrationFacilitated negotiationResolutionPAGE 27
confidential – <strong>for</strong> guild <strong>members</strong> onlyVariation and renewal of the <strong>Agreement</strong> (Part L)The <strong>Agreement</strong> provides <strong>for</strong> two types of <strong>Agreement</strong> variations; those resulting from mutual agreement (voluntary) andthose resulting from a Crown Directive or a law change (compulsory).The DHBs acknowledge the importance of continuing to fund pharmacy services but this is not a guarantee they will enterinto a future agreement with a particular pharmacy.L3: Variation after review Either party may initiate a review of any aspect of the <strong>Agreement</strong> if there are any changes tothe funding available to the DHB, government pharmaceutical policy, the services pharmaciesare required to provide, or both parties agree exceptional circumstances apply.L4: Procedure <strong>for</strong> CompulsoryVariationA review is conducted by providing the other party with a written notice identifying theconcern and proposing a variation to resolve it. The other party has 20 business days toaccept or reject the proposal or make a counter proposal. If agreement is not reached, the<strong>Agreement</strong> continues in <strong>for</strong>ce.Compulsory variations will be written in a way to minimise any adverse effect on thepharmacy. The procedure <strong>for</strong> a compulsory variation involves the DHB providing a proposeddraft, the pharmacy having at least 10 days to comment after which the parties will try toreach agreement on the terms of the variation. If agreement cannot be reached, the PSA willbe varied on the terms originally proposed.A pharmacy may stop providing any service affected by a compulsory variation with sixmonths notice. If the service becomes non-viable after the variation, a shorter but reasonableperiod of notice may be given. Pharmacies should note that if they withdraw from a serviceon viability grounds the DHB may seek a solvency certificate or a solvency audit (clause J3).L5: Group negotiation Where a pharmacy initiates a voluntary variation the DHB may decide to negotiate thevariation with other pharmacies it thinks might also take up the variation. This negotiationmight be conducted in a group setting rather than individually.Pharmacies initiating a variation covering a service they have developed should protect anyunique intellectual property involved be<strong>for</strong>e initiating the review.Pharmacies asked to take part in a group negotiation should seek legal advice on theirposition under the Commerce Act be<strong>for</strong>e agreeing to participate.PAGE 28
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyDealings with third parties (Part M)This section of the <strong>Agreement</strong> pulls together the provisions involving the pharmacy’s links with other organisations andproviders, covering subcontracting relationships, assignment of the PSA, confidentiality and incentives to prescribers.Doctors face similar prohibitions on giving or accepting incentives.M2: Subcontracting Pharmacies are entitled to subcontract the provision of any aspect of the provision of servicesbut must first obtain the written agreement of the DHB. Similarly, a subcontractor may notfurther subcontract the service in question or assign the subcontract to another party withoutthe DHB’s written agreement.The pharmacy must ensure the subcontract will allow the pharmacy to honour all itsobligations with the DHB. For instance, the subcontractor is subject to the same requirementsas the pharmacy <strong>for</strong> in<strong>for</strong>mation provision and audit.M4.1: No transfer withoutconsentM6; Incentives andinducements to prescribersIf asked, the pharmacy must give the auditor a copy of the subcontract. However, the auditormust not disclose any financial arrangements from the subcontract to the DHB. The auditor isable to advise the DHB if they consider aspects of the subcontract may prejudice thepharmacy’s ability to meet its Service <strong>Agreement</strong> template obligations.You may not assign or transfer any of your obligations under the <strong>Agreement</strong> without the priorwritten consent of your DHB. This includes the sale or disposal of any majority ownership orcontrol of your business.DHBs will not unreasonably withhold consent.Pharmacies must comply with section 9.7 of the Code of Ethics. If a pharmacy breaches thisrequirement to not offer inducements to prescribers, the DHB would be able to laycomplaints with the Council against the Charge Pharmacist and the pharmacist owner.Miscellaneous terms (Part N)This section pulls together a variety of <strong>Agreement</strong> matters not conveniently situated elsewhere. Members should reviewthe section and particularly familiarise themselves with the requirement <strong>for</strong> appropriate insurance and the rules governinghow notices must be delivered and when they become effective.N4: Warranty Both parties warrant they will provide accurate in<strong>for</strong>mation to the other. Pharmacies shouldnote sub clause 4.2 ensures this warranty remains active throughout the life of the<strong>Agreement</strong>.N7: Entire <strong>Agreement</strong> There should be no agreements between you and your DHB that are not included in your PSA.Check Part P carefully to make sure all your dealings with your DHB are contained therein.In addition, we advise if you intend to sign this <strong>Agreement</strong>, you should also sign and attachthe side letter regarding the Date of Dispensing definition to the PSA. This will further solidifythe standing of the side letter.PAGE 29
confidential – <strong>for</strong> guild <strong>members</strong> onlyFailure to per<strong>for</strong>m and termination of <strong>Agreement</strong> (Part O)All agreements must provide remedies <strong>for</strong> circumstances where either party fails to meet its responsibilities. Part Oestablishes the circumstances under which the remedies can be applied, identifies the full range of remedies availableand then defines the rules under which they operate.O2: Where you have failed toper<strong>for</strong>mThe provisions of Part O only apply when a pharmacy has failed to per<strong>for</strong>m anymaterial obligation.Remedies available to the DHB include: “<strong>for</strong>cing” you to provide the Service, suspending orterminating the PSA, seeking damages and/or default interest, or referring the matter to the<strong>Pharmacy</strong> Advisory Committee.O6: Uncontrollable events If either party is unable to per<strong>for</strong>m their obligations they must advise the other party, takeall reasonable steps available to avoid or mitigate the impact of the problem and resumeper<strong>for</strong>mance as soon as they are able. If the problem lasts more than 30 days the partiesmust try to agree on the extent to which the affected service can continue to be delivered orneeds to be varied if this is possible.O8: Mutual agreement toterminateYou may mutually agree with your DHB to terminate the <strong>Agreement</strong> at any time.O9: Our right to terminate The DHB can terminate the <strong>Agreement</strong> <strong>for</strong> failure to meet a Material Obligation, inability toper<strong>for</strong>m, on the sale or closure of the pharmacy (the <strong>Agreement</strong> would usually be assignedwhen the pharmacy was sold), because of bankruptcy or receivership, because of illegalaction, because of an uncontrollable event, or on three months’ notice.O10: Your right to terminate Pharmacies may terminate the <strong>Agreement</strong> <strong>for</strong> the DHB’s failure to per<strong>for</strong>m a MaterialObligation, following a compulsory variation, because of an uncontrollable event, or on sixmonths’ notice.O11: Alternative totermination of entire<strong>Agreement</strong>As an alternative to terminating the entire <strong>Agreement</strong>, either you or the DHB can decide toterminate a pharmacy’s provision of a particular service by giving six months’ written notice.Provider specific terms and conditions (Part P)Part P allows the DHBs to contract <strong>for</strong> additional services with individual pharmacies to provide local solutions <strong>for</strong> localproblems. This section also records which, if any, of the specialised <strong>Services</strong> listed in Part C and Schedule C1 you arecontracted to supply. Due to clause N7, it is important that all your arrangements you may have with your DHB outsideof the provision of Base <strong>Pharmacy</strong> <strong>Services</strong> are listed here.Service Specifications (Schedule C1)Schedule C1 records the specifications <strong>for</strong> each of the services the pharmacy agrees to provide. The specificationsare broken down into the various services; “Base <strong>Pharmacy</strong> <strong>Services</strong>” is common to all pharmacies. In addition you maybe contracted to provide any number (or none) of the additional services from the following list:■■ <strong>Pharmacy</strong> Methadone <strong>Services</strong> <strong>for</strong> Opioid Dependence (Class B Controlled Drug <strong>Services</strong>)■■ Aseptic <strong>Pharmacy</strong> <strong>Services</strong> (including Syringe Driver <strong>Services</strong>)■■ Sterile Manufacturing <strong>Services</strong>■■ Special Foods <strong>Services</strong>■■ Special Foods Infant Formulae <strong>Services</strong>■■ Provision of Blood Glucose Test Strips■■ Complex Medicine <strong>Services</strong>■■ <strong>Pharmacy</strong> Clozapine <strong>Services</strong> (Monitored Therapy Medicine <strong>Services</strong>).Note that your <strong>Agreement</strong> contains all the above service specifications, even if you are not contracted to provide them.However, you are only contracted to supply these <strong>Services</strong> if they are listed in clause C2 of Schedule C1 and are listed inPart P.PAGE 30
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyPharmacies not providing these additional services can apply to their DHB to expand the range of services they supply.Each of the Service Specifications follows a standard template, detailing the specific requirements of each of the services.Schedule C1 Base <strong>Pharmacy</strong><strong>Services</strong> 3.2: Dispensing aSpecific BrandSchedule C1 Base <strong>Pharmacy</strong><strong>Services</strong> 6.2: Opening HoursSchedule C1 Base <strong>Pharmacy</strong><strong>Services</strong> 7.1: ProcessesSchedule C1 Base <strong>Pharmacy</strong><strong>Services</strong> 7.1 (j): MethadoneSchedule C1 Base <strong>Pharmacy</strong><strong>Services</strong> 7.2: Waiting times<strong>for</strong> serviceSchedule C1 <strong>Pharmacy</strong>Methadone <strong>Services</strong> <strong>for</strong>Opioid Dependence6.1:ProcessesSchedule C1 <strong>Pharmacy</strong>Methadone <strong>Services</strong> <strong>for</strong>Opioid Dependence 6.4:Waiting timesThe purpose of this clause is to limit your choice when dispensing generics wherever apharmaceutical is deemed “Preferred Supplier Brand” by the Pharmaceutical Schedule.Currently there are no “Preferred Supplier Brands” listed in the Pharmaceutical Schedule.Ordinarily, you must be open <strong>for</strong> a minimum of five days a week.Your DHB may additionally contract with you to offer specific after hours’ services. If this isthe case, these arrangements will be listed in Part P.Note you may choose to offer after hours’ services if you wish to; you do not need a separatecontract with your DHB if you choose to operate after hours.Base <strong>Pharmacy</strong> <strong>Services</strong> includes (and there<strong>for</strong>e the PSA covers) the dispensing of subsidisedpharmaceuticals, ensuring the completeness of in<strong>for</strong>mation on prescriptions, the provision ofadvice and counselling, maintaining Service User Records, reporting significant findings to theprescriber and administration.Base <strong>Pharmacy</strong> <strong>Services</strong> includes Practitioner Supply Orders, Bulk Supply Orders, rest homeservices, the NRT programme and Methadone (unless you have the separate “<strong>Pharmacy</strong>Methadone <strong>Services</strong> <strong>for</strong> Opioid Dependence” service listed in clause C2 of Schedule C1.If you do not have the separate “<strong>Pharmacy</strong> Methadone <strong>Services</strong> <strong>for</strong> Opioid Dependence”service listed in clause C2 of Schedule C1, you may still provide Methadone services to up totwo Service Users per claim period.If you do not wish to provide Methadone services at all, you must notify your DHB in writing.You are obligated to meet the following minimum standards:• 90% of items will be dispensed within one hour of being presented on a business day.• 99% of items dispensed within 24 hours of being presented on a business day.• 100% of items dispensed within two business days of being presented on a business day.You should maintain adequate stock levels to meet these requirements.These requirements only apply if the medicine is available in New Zealand at the time theprescription is presented. Also, these requirements only apply to pharmaceuticals covered bythe Base <strong>Pharmacy</strong> <strong>Services</strong> specification.Pharmacies facing unusual supply problems may negotiate different waiting timerequirements with the DHB. This provision would particularly apply to rural pharmacies.Additionally, these requirements do not apply if there is mutual agreement between you andthe Service User to a different waiting time. It might be a good idea to document theseagreements if you are having difficulty meeting these requirements.You agree to provide Methadone services in accordance with the community pharmacistdispensing protocol in Section 4 and 11 of the Opioid Substitution Treatment New ZealandPractice <strong>Guide</strong>lines 2008. A copy of the guidelines is available at http://www.moh.govt.nz/moh.nsf/indexmh/opioid-substitution-treatment-guidelines-dec2008?OpenFor existing approved Service User: 95% should receive their dose within 15 minutes and100% within 30 minutes of arriving at the pharmacy.For newly-approved Service Users: 95% should receive their dose within 30 minutes and100% within two hours, provided all documentation is satisfactory.Schedule C1 <strong>Pharmacy</strong>Methadone <strong>Services</strong> <strong>for</strong>Opioid Dependence 6.5(b):Facilities and settingsThe provision of the Service is to be carried out in a private and confidential manner, whichminimises the concerns of other Service Users.PAGE 31
confidential – <strong>for</strong> guild <strong>members</strong> onlySchedule C1 <strong>Pharmacy</strong>Methadone <strong>Services</strong> <strong>for</strong>Opioid Dependence 9: QualityrequirementsSchedule C1 Aseptic<strong>Pharmacy</strong> <strong>Services</strong> (includingSyringe Driver <strong>Services</strong>)Schedule C1 Aseptic<strong>Pharmacy</strong> <strong>Services</strong> (includingSyringe Driver <strong>Services</strong>) 6.3:Waiting timesSchedule C1 SterileManufacturing <strong>Services</strong>Schedule C1 SterileManufacturing <strong>Services</strong> 6.3:waiting TimesSchedule C1 Special Foods<strong>Services</strong>Schedule C1 Special FoodsInfant Formulae <strong>Services</strong>Schedule C1 Provision ofBlood Glucose Test StripsSchedule C1 ComplexMedicine <strong>Services</strong>Schedule C1 <strong>Pharmacy</strong>Clozapine <strong>Services</strong> (MonitoredTherapy Medicine <strong>Services</strong>)<strong>Services</strong> must be provided by a pharmacist.This PSA now splits out Sterile Manufacturing services from Aseptic services. Graseby pumpsremain with Aseptic services.Aseptic preparations should be made within a Grade D air environment. Syringes shouldadditionally be prepared within an approved still air box.The New Zealand Code of Good Manufacturing Practice can be ordered from Medsafe.99% of aseptic preparations must be dispensed within 24 hours.100% of aseptic preparations must be dispensed within two business days.Or by mutual agreement with the Service User.Sterile preparations should be made within laminar flow cabinet or isolator (Grade A airenvironments) within a Grade B air environment room.99% of sterile preparations must be dispensed within 24 hours.100% of sterile preparations must be dispensed within two business days.Or by mutual agreement with the Service User.Note that the Pharmaceutical Schedule stipulates that HP3 products (ie most special foods)are only subsidised when dispensed from a pharmacy with a Special Foods <strong>Services</strong> contract.There<strong>for</strong>e, if you do not have Special Foods <strong>Services</strong> listed in Part P, you may not claim <strong>for</strong>dispensing these Special Foods.DHBs have indicated that extra money will be made available <strong>for</strong> the providers of specialfoods (approximately $500,000 per annum nationally) to address the margin losses on thecost of goods sold. The mechanism <strong>for</strong> this injection of funds is yet to be determined.Some pharmacies have special arrangements regarding infant <strong>for</strong>mulae. This section will notaffect most <strong>members</strong>. If you do not have this section, you are still able to dispense and claim<strong>for</strong> infant <strong>for</strong>mulae under Special Foods <strong>Services</strong>.Some pharmacies have special arrangements regarding test strips. This section will not affectmost <strong>members</strong>. If you do not have this section, you are still able to dispense and claim <strong>for</strong>test strips under Base <strong>Pharmacy</strong> <strong>Services</strong>.Note that the Pharmaceutical Schedule stipulates that HP1 pharmaceuticals are onlysubsidised when dispensed from a pharmacy with a Complex Medicines <strong>Services</strong> contract.There<strong>for</strong>e, if you do not have Complex Medicines <strong>Services</strong> listed in Part P, you may notclaim <strong>for</strong> dispensing HP1 medicines.This service specification should be read in conjunction with Schedule C2 Protocol <strong>for</strong> theDispensing of Clozapine by Community Pharmacies.Note that Clozapine <strong>Services</strong> can only be provided by a pharmacist that has completed thenecessary clozapine-specific training.If you have further questions regarding Clozapine <strong>Services</strong> please contact the <strong>Guild</strong>.PAGE 32
confidential – <strong>for</strong> – <strong>for</strong> guild guild <strong>members</strong> only onlyPayment terms (Schedule H1)This Schedule draws together the payment terms <strong>for</strong> all the services pharmacy provides under the PSA. Pharmacies agreeingto provide additional services under Part P of the Service <strong>Agreement</strong> template may find this also varies Schedule H1.The basis <strong>for</strong> claiming is fee-<strong>for</strong>-service. The basic <strong>for</strong>mula is:Amount claimable =Dispensing Fee + Drug subsidy and margin – Co-paymentYour dispensary software should automatically generate the correct claim amounts <strong>for</strong> each dispensing.Dispensing feeEach prescription item generates a dispensing fee of $5.30 (excluding GST). This dispensing fee is then multiplied by theapplicable multiplier. For most services the multiplier is one. However, more complicated dispensings tend to have highermultipliers to reflect the additional professional input. For example, Monitored Therapy Medicine <strong>Services</strong> has a multiplierof two. There<strong>for</strong>e, each clozapine dispensing generates a dispensing fee of $10.60 ($5.30 x 2), plus GST.Drug subsidy and marginYou are able to claim the subsidy <strong>for</strong> each pharmaceutical that is listed in the Pharmaceutical Schedule. The side letterregarding the date of dispensing definition confirms that the correct subsidy to be claimed is the subsidy that applied asat the date the prescription was presented, not the date the pharmaceuticals were collected.In addition to the subsidy, you are able to claim a mark-up on the subsidy. This mark-up is erroneously referred to as amargin in the <strong>Agreement</strong>. For almost all pharmacies the mark-up is either 4% or 5%.■■ A mark-up of 5% is applied to all products where the subsidy price of the pack listed in the Pharmaceutical Schedule is$150 or greater. It is designed to compensate <strong>for</strong> the additional risks associated with broken packs of slow moving lines.■■ A mark-up of 5% is applied to all products listed as a Special Food in the Pharmaceutical Schedule.■■ For all other products, the mark-up is 4%.Subsidies and mark-ups are all stated as excluding GST.Co-paymentFinally, the claim amount is reduced by the co-payment that was applicable on that item. Note that the co-paymentincludes GST.Regardless of the actual co-payment you collected, the amount the claim is reduced by is the maximum co-payment youcould have collected. This ensures that pharmacies that choose to discount the co-payments they charge bear the cost ofthat discounting, not the DHB.Product Premiums and <strong>Pharmacy</strong> ChargesIn addition to the amounts you may claim from the DHB, which is covered by this schedule, some additional amounts maybe charged directly to the service user. Please refer to clauses H4.5 (Product Premiums) and H4.6 (<strong>Pharmacy</strong> Charges) <strong>for</strong>permissible charges.Also note that you may charge <strong>for</strong> other services you provide to the Service Users that are in excess of the requirements ofthe PSA or the Pharmaceutical Schedule. An example of this might be accepting a credit card payment as a co-payment.Audit framework (Schedule J1)This Schedule provides detail of the audit framework arising from the <strong>Agreement</strong>, in particular specifying the obligations ofthe auditor and the pharmacy, timeframes and a generic process outline.PAGE 33
confidential – <strong>for</strong> guild <strong>members</strong> onlySection Four: PSA <strong>2010</strong> checklistPlease note that the PSA places many other requirements on you that are not listed in the checklist. Fully complying withthe checklist does not mean you have fully discharged your obligations under the PSA.Be<strong>for</strong>e deciding whether to accept the new <strong>Agreement</strong>, you should:1. Read this <strong>Guide</strong> to the PSA.2. Read your PSA.3. Check Part P <strong>for</strong> completeness. This part now lists all the contractual arrangements/variations that youhave with your DHB.4. Check clause C2 of Schedule C1 <strong>for</strong> completeness. This clause lists which of the service specificationscontained in the Schedule you are contracted to provide.5. Carefully consider the aspects of the PSA where the relationship between pharmacy and the DHB haschanged and understand the implications of these changes <strong>for</strong> your pharmacy. These aspects are identifiedin this <strong>Guide</strong>.6. Seek advice about any aspect of the PSA you do not understand or have concerns about.7. Identify any groups of patients located outside the DHB’s boundaries routinely served by your pharmacy.8. Consider whether you want to expand the range of services provided by your pharmacy and identify suchservices <strong>for</strong> future discussion with your DHB.If you decide to accept the <strong>Agreement</strong>, you need to:1. Sign, date and fill in all the relevant sections in Part B3 of both copies of the <strong>Agreement</strong>.2. Initial each page of both copies of the <strong>Agreement</strong>.3. Copy the side letter. Initial each page of the side letter and attach to the <strong>Agreement</strong>.4. Fill in the relevant sections of Schedule N1: Bank account details in both copies of the <strong>Agreement</strong>.5. Sign, date and attach a copy of each page of the side letter regarding the date of dispensing to both copiesof the <strong>Agreement</strong>.6. Recheck you have initialled, signed, dated and filled in all the relevant sections of both copies of the<strong>Agreement</strong> and have attached copies of the side letter as identified above.7. Send both signed copies of the <strong>Agreement</strong> to your DHB to be received by 28 February <strong>2010</strong>.8. If you routinely provide services to a group of patients outside your DHB’s area, contact your DHB toexchange an agreement in writing to continue to service these patients.9. If you want to expand the range of services you provide, eg Clozapine or Complex Medicines, contact yourDHB to discuss.10. Diarise an annual review of your Quality Improvement Plan (clause G3.1).11. Develop and implement a written Health Emergency Plan (clause G5.6).If you decide not to accept the <strong>Agreement</strong>, or any part thereof, you need to:1. Contact your DHB to explain your concern(s) and make arrangements to negotiate directly with theDHB on those matters.PAGE 34
confidential – <strong>for</strong> guild <strong>members</strong> onlyNotesPAGE 35
confidential – <strong>for</strong> guild <strong>members</strong> onlyNotesPAGE 36
confidential – <strong>for</strong> guild <strong>members</strong> only
confidential – <strong>for</strong> guild <strong>members</strong> onlyPHARMACY GUILD OF NEW ZEALAND (INC)<strong>Pharmacy</strong> House 124 Dixon Street, Te Aro, Wellington 6011PO Box 27139, Marion Square, Wellington 6141Ph 04 802 8200 Fax 04 384 8085 www.pgnz.org.nz