YOUR HEALTH IN THE LAST 5 YEARSClient oneClient two2. Apart from anything you havealready told us about, during theLAST 5 YEARS have you seena doctor, nurse or other healthpr<strong>of</strong>essional for:c) Please ignore diarrhoea; foodpoisoning; indigestion; sickness orvomiting; stomach bug or upset;provided no hospital investigationhas been advised or completed.d) Please ignore chest infection; hayfever; pleurisy; upper respiratorytract infection (URTI); from whichyou have fully recovered.e) For <strong>Life</strong> only, please ignore backache; back spasm; cricked neck;fibrositis; frozen shoulder;lumbago; stiff neck; trapped nerveor operation to correct this.h) For <strong>Life</strong> only, please ignore deafness(partially or totally from birth); for allproducts, please ignore earache;ear infection; ear wax or syringing;glue ear; grommet insertion; otitis.i) Please ignore astigmatism; blackeye; blocked tear duct; conjunctivitis;dry eyes; long sighted; myopia(short sighted); squint; stye(s).j) Please ignore blood blister; boil;bunion; corn; ganglion; verruca;wart if no biopsy or hospitalinvestigation needed.k) Please ignore birthmarks whereno treatment or specialist referralhas been advised.m) Please ignore investigations relatedto pregnancy or infertility wherethe results have been confirmedas normal.n) Please ignore routine cervicalsmears and mammograms if theresults have been normal.a) raised blood pressure, raised cholesterol, orcondition affecting blood or blood vessels, forexample anaemia, excess sugar in the blood,blood clot, deep vein thrombosis?b) any condition affecting your kidneys, bladderor prostate, for example blood or protein inthe urine, stones, nephritis?c) any condition affecting your stomach,oesophagus, liver, pancreas or bowel, for exampleCrohn’s disease, ulcerative colitis, hepatitis?d) any condition affecting your lungs or breathing,for example asthma, sarcoidosis, emphysema?e) lupus, ankylosing spondylitis, gout or any form<strong>of</strong> arthritis, neck, back, spine or joint trouble, forexample rheumatoid arthritis, sciatica?f) anxiety, depression, any form <strong>of</strong> nervous ormental disorder needing treatment or counselling,chronic fatigue or persistent tiredness?g) any condition affecting your thyroid?h) any condition affecting your ears or hearing,for example Meniere’s disease, deafness?i) any condition affecting your eyes or vision,not wholly corrected by spectacles or lenses,for example cataract, blindness?j) a growth, lump, polyp or tumour <strong>of</strong> any kind?k) a mole or freckle?l) chest pain, palpitations, irregular heartbeat,paralysis, numbness, persistent tingling orpins and needles, tremor, facial pain otherthan dental pain, memory loss, dizzinessor balance problems?m) any other condition or symptom which hasneeded an angiogram, CT scan, ECG or MRI?Question 2n is applicable for females onlyn) a cervical smear or gynaecological disorder orbreast problem, for which you have needed furtherinvestigation, tests, advice, or for which you havenot yet been discharged from follow-up?Yes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes NoYes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoYes No Yes NoIf you have answered ‘Yes’ to ANY part <strong>of</strong> the above question, please complete one <strong>of</strong> the Medical Questionnaires (Part 6) BEFOREcontinuing with the next question.YOUR HEALTH IN THE LAST 12 MONTHSClient oneClient two3. Apart from anything you havealready told us about, during theLAST 12 MONTHS have you:a) Please ignore oral contraceptionpill; pregnancy; minor accidentsand injuries, for example musclestrain, pulled muscle, tornligament or tendon, or sprainedjoint, provided they have not keptyou <strong>of</strong>f work for 2 weeks for more.b) Please ignore investigationsrelated to pregnancy or infertilitywhere the results have beenconfirmed as normal.a) had any medical condition, illness or injuryfor which you have received treatment for acontinuous period <strong>of</strong> 4 weeks or more?b) had or been advised to have any investigationsin hospital, for example biopsy, CT scan, ECG,echocardiogram?c) had anything else for which you are awaitingreferral, investigations, results or treatmentor do you have any other symptoms for whichyou have not yet sought medical advice, forexample unexplained bleeding, weight loss,lump, growth, mole or freckle which hasrecently changed in appearance?YesYesYesNoNoNoYesYesYesNoNoNoIf you have answered ‘Yes’ to ANY part <strong>of</strong> the above question, please complete one <strong>of</strong> the Medical Questionnaires (Part 6) BEFOREcontinuing with the next question.Page 10<strong>Whole</strong> <strong>of</strong> <strong>Life</strong> Protection Plan – <strong>Application</strong> <strong>Form</strong> and Additional Questionnaires
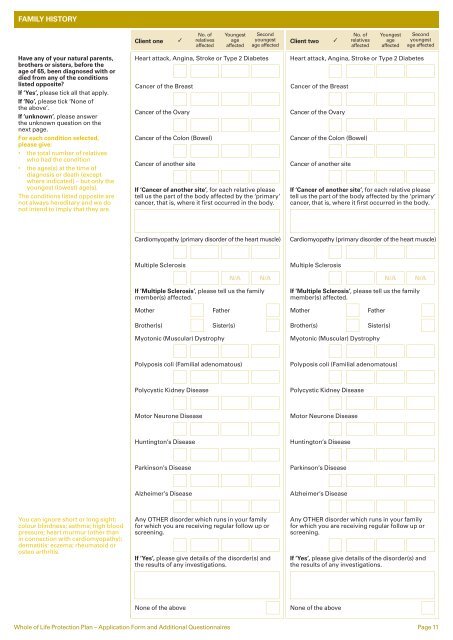
FAMILY HISTORYClient one3No. <strong>of</strong>relativesaffectedYoungestageaffectedSecondyoungestage affectedClient two3No. <strong>of</strong>relativesaffectedYoungestageaffectedSecondyoungestage affectedHave any <strong>of</strong> your natural parents,brothers or sisters, before theage <strong>of</strong> 65, been diagnosed with ordied from any <strong>of</strong> the conditionslisted opposite?If ‘Yes’, please tick all that apply.If ‘No’, please tick ‘None <strong>of</strong>the above’.If ‘unknown’, please answerthe unknown question on thenext page.For each condition selected,please give:• the total number <strong>of</strong> relativeswho had the condition• the ages(s) at the time <strong>of</strong>diagnosis or death (exceptwhere indicated) – but only theyoungest (lowest) age(s).The conditions listed opposite arenot always hereditary and we donot intend to imply that they are.Heart attack, Angina, Stroke or Type 2 DiabetesCancer <strong>of</strong> the BreastCancer <strong>of</strong> the OvaryCancer <strong>of</strong> the Colon (Bowel)Cancer <strong>of</strong> another siteIf ‘Cancer <strong>of</strong> another site’, for each relative pleasetell us the part <strong>of</strong> the body affected by the ‘primary’cancer, that is, where it first occurred in the body.Heart attack, Angina, Stroke or Type 2 DiabetesCancer <strong>of</strong> the BreastCancer <strong>of</strong> the OvaryCancer <strong>of</strong> the Colon (Bowel)Cancer <strong>of</strong> another siteIf ‘Cancer <strong>of</strong> another site’, for each relative pleasetell us the part <strong>of</strong> the body affected by the ‘primary’cancer, that is, where it first occurred in the body.Cardiomyopathy (primary disorder <strong>of</strong> the heart muscle)Cardiomyopathy (primary disorder <strong>of</strong> the heart muscle)Multiple SclerosisMultiple SclerosisN/AN/AN/AN/AIf ‘Multiple Sclerosis’, please tell us the familymember(s) affected.If ‘Multiple Sclerosis’, please tell us the familymember(s) affected.MotherFatherMotherFatherBrother(s)Sister(s)Brother(s)Sister(s)Myotonic (Muscular) DystrophyMyotonic (Muscular) DystrophyPolyposis coli (Familial adenomatous)Polyposis coli (Familial adenomatous)Polycystic Kidney DiseasePolycystic Kidney DiseaseMotor Neurone DiseaseMotor Neurone DiseaseHuntington’s DiseaseHuntington’s DiseaseParkinson’s DiseaseParkinson’s DiseaseAlzheimer’s DiseaseAlzheimer’s DiseaseYou can ignore short or long sight;colour blindness; asthma; high bloodpressure; heart murmur (other thanin connection with cardiomyopathy);dermatitis: eczema; rheumatoid orosteo arthritis.Any OTHER disorder which runs in your familyfor which you are receiving regular follow up orscreening.If ‘Yes’, please give details <strong>of</strong> the disorder(s) andthe results <strong>of</strong> any investigations.Any OTHER disorder which runs in your familyfor which you are receiving regular follow up orscreening.If ‘Yes’, please give details <strong>of</strong> the disorder(s) andthe results <strong>of</strong> any investigations.None <strong>of</strong> the aboveNone <strong>of</strong> the above<strong>Whole</strong> <strong>of</strong> <strong>Life</strong> Protection Plan – <strong>Application</strong> <strong>Form</strong> and Additional Questionnaires Page 11