Empirical antimicrobial therapy for surgical infections in adults
Empirical antimicrobial therapy for surgical infections in adults
Empirical antimicrobial therapy for surgical infections in adults

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
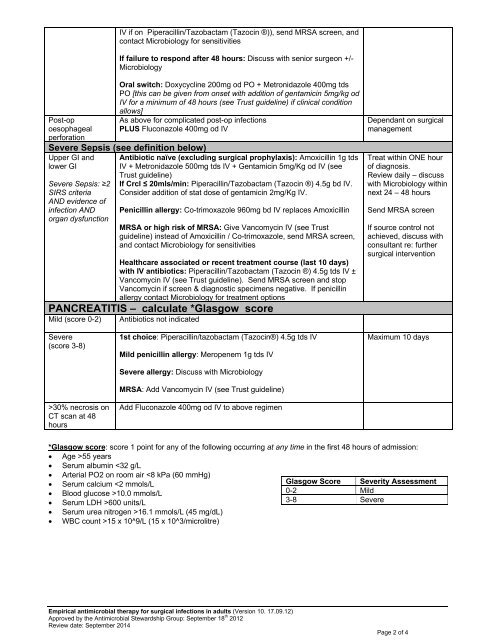
IV if on Piperacill<strong>in</strong>/Tazobactam (Tazoc<strong>in</strong> ®)), send MRSA screen, andcontact Microbiology <strong>for</strong> sensitivitiesIf failure to respond after 48 hours: Discuss with senior surgeon +/-MicrobiologyOral switch: Doxycycl<strong>in</strong>e 200mg od PO + Metronidazole 400mg tdsPO [this can be given from onset with addition of gentamic<strong>in</strong> 5mg/kg odIV <strong>for</strong> a m<strong>in</strong>imum of 48 hours (see Trust guidel<strong>in</strong>e) if cl<strong>in</strong>ical conditionallows]As above <strong>for</strong> complicated post-op <strong><strong>in</strong>fections</strong>PLUS Fluconazole 400mg od IVPost-opoesophagealper<strong>for</strong>ationSevere Sepsis (see def<strong>in</strong>ition below)Upper GI andlower GISevere Sepsis: ≥2SIRS criteriaAND evidence of<strong>in</strong>fection ANDorgan dysfunctionAntibiotic naïve (exclud<strong>in</strong>g <strong>surgical</strong> prophylaxis): Amoxicill<strong>in</strong> 1g tdsIV + Metronidazole 500mg tds IV + Gentamic<strong>in</strong> 5mg/Kg od IV (seeTrust guidel<strong>in</strong>e)If Crcl ≤ 20mls/m<strong>in</strong>: Piperacill<strong>in</strong>/Tazobactam (Tazoc<strong>in</strong> ®) 4.5g bd IV.Consider addition of stat dose of gentamic<strong>in</strong> 2mg/Kg IV.Penicill<strong>in</strong> allergy: Co-trimoxazole 960mg bd IV replaces Amoxicill<strong>in</strong>MRSA or high risk of MRSA: Give Vancomyc<strong>in</strong> IV (see Trustguidel<strong>in</strong>e) <strong>in</strong>stead of Amoxicill<strong>in</strong> / Co-trimoxazole, send MRSA screen,and contact Microbiology <strong>for</strong> sensitivitiesHealthcare associated or recent treatment course (last 10 days)with IV antibiotics: Piperacill<strong>in</strong>/Tazobactam (Tazoc<strong>in</strong> ®) 4.5g tds IV ±Vancomyc<strong>in</strong> IV (see Trust guidel<strong>in</strong>e). Send MRSA screen and stopVancomyc<strong>in</strong> if screen & diagnostic specimens negative. If penicill<strong>in</strong>allergy contact Microbiology <strong>for</strong> treatment optionsPANCREATITIS – calculate *Glasgow scoreMild (score 0-2) Antibiotics not <strong>in</strong>dicatedDependant on <strong>surgical</strong>managementTreat with<strong>in</strong> ONE hourof diagnosis.Review daily – discusswith Microbiology with<strong>in</strong>next 24 – 48 hoursSend MRSA screenIf source control notachieved, discuss withconsultant re: further<strong>surgical</strong> <strong>in</strong>terventionSevere(score 3-8)>30% necrosis onCT scan at 48hours1st choice: Piperacill<strong>in</strong>/tazobactam (Tazoc<strong>in</strong>®) 4.5g tds IVMild penicill<strong>in</strong> allergy: Meropenem 1g tds IVSevere allergy: Discuss with MicrobiologyMRSA: Add Vancomyc<strong>in</strong> IV (see Trust guidel<strong>in</strong>e)Add Fluconazole 400mg od IV to above regimenMaximum 10 days*Glasgow score: score 1 po<strong>in</strong>t <strong>for</strong> any of the follow<strong>in</strong>g occurr<strong>in</strong>g at any time <strong>in</strong> the first 48 hours of admission:• Age >55 years• Serum album<strong>in</strong> 16.1 mmols/L (45 mg/dL)• WBC count >15 x 10^9/L (15 x 10^3/microlitre)Glasgow Score Severity Assessment0-2 Mild3-8 Severe<strong>Empirical</strong> <strong>antimicrobial</strong> <strong>therapy</strong> <strong>for</strong> <strong>surgical</strong> <strong><strong>in</strong>fections</strong> <strong>in</strong> <strong>adults</strong> (Version 10. 17.09.12)Approved by the Antimicrobial Stewardship Group: September 18 th 2012Review date: September 2014Page 2 of 4